
Abstract
BACKGROUND AND PURPOSE: Secondary-progressive MS is characterized by reduced acute inflammation and contrast enhancement but with increased axonal degeneration and cognitive/clinical disability that worsens with advanced disease. Relative recirculation, extracted from DSC is a surrogate measure of BBB integrity. We hypothesized that normal-appearing white matter relative recirculation is reduced in cognitively impaired compared with nonimpaired secondary-progressive MS, reflecting more advanced disease.
MATERIALS AND METHODS: Cognitive performance was classified as impaired or nonimpaired by use of Minimal Assessment of Cognitive Function In MS test components. Demographic data, brain parenchymal fraction, WM lesion fraction, and weighted mean normal-appearing white matter relative recirculation were compared in cognitively dichotomized groups. Univariate and multivariate logistic regressions were used to study the association between cognitive test results and normal-appearing white matter relative recirculation.
RESULTS: The mean (SD) age of 36 patients with secondary-progressive MS studied was 55.9 ± 9.3 years; 13 of 36 (36%) patients were male. A highly significant difference between normal-appearing white matter relative recirculation and WM lesion relative recirculation was present for all patients (P < .001). Normal-appearing white matter relative recirculation in impaired patients was significantly lower than in nonimpaired subjects for the Symbol Digit Modalities Test (P = .007), Controlled Word Association Test (P = .008), and Paced Auditory Serial Addition Test (P = .024). The Expanded Disability Status Scale demonstrated an inverse correlation with normal-appearing white matter relative recirculation (r = −0.319, P = .075). After adjustment for confounders, significant normal-appearing white matter relative recirculation reduction persisted for the Symbol Digit Modalities Test (P = .023) and the Paced Auditory Serial Addition Test (P = .047) but not for the Controlled Word Association Test (P = .13) in impaired patients.
CONCLUSIONS: Significant normal-appearing white matter relative recirculation reduction exists in cognitively impaired patients with secondary-progressive MS, localizing to the domains of processing speed and working memory.
ABBREVIATIONS:
- rR
- relative recirculation
- NAWM
- normal-appearing white matter
- SPMS
- secondary-progressive MS
- RRMS
- relapsing-remitting MS
MS is the most common inflammatory demyelinating disease of the central nervous system. Although the underlying etiology of the disease is still largely unknown, inflammation, demyelination, and neurodegeneration are pathologically implicated and eventually cause long-term impairment.1 Cognitive impairment is reported in 40–70% of MS cases,2 and the frequency and expression of impairment increases with disease duration.3 Secondary-progressive MS is clinically distinct from relapsing-remitting MS. Patients with secondary-progressive MS do not manifest acute attacks4 and demonstrate diminished response to immunosuppressives,4 reduced lesional gadolinium enhancement,5 and diffuse NAWM inflammation and axonal injury.6
Traditional structural markers including WM lesion load and cortical and WM atrophy demonstrate variable correlation with cognitive impairment.7 Advanced MR imaging techniques are increasingly being investigated as surrogate markers of cognition. Techniques such as magnetization transfer imaging,8 diffusion-weighted imaging,9 functional MR imaging,10 MR spectroscopy,11 and perfusion imaging12 have previously been described. In RRMS, localized inflammation and BBB breakdown depicted with gadolinium-enhanced T1-weighted MR imaging are traditionally associated with disease activity.13,14 Unlike RRMS, SPMS is characterized by reduced acute inflammation and few contrast- enhancing lesions.5 A number of mechanisms are described for the reduced apparent inflammation, including “compartmentalization” of the inflammatory response behind an intact BBB,6 balanced inflammation, activation of endogenous neuroprotection mechanisms,15,16 and continued neurodegeneration independent of inflammation.6,17 Despite a reduction of acute inflammatory changes, SPMS is associated with a higher prevalence of axonal degeneration, disability, and cognitive impairment, particularly in the domains of attention and processing speed. These functional domains may therefore serve as markers of more advanced axonal degeneration, distinguishing SPMS subgroups with more advanced disease.18
Relative recirculation (rR), a parameter extracted from DSC MR imaging, is shown to successfully identify regions of BBB breakdown in patients with brain tumors,19,20 Moyamoya syndrome,21 and acute ischemic stroke.22 rR is a quantitative measure of contrast recirculation abnormalities after the first pass and is a practical surrogate for BBB permeability estimates that does not necessitate a separate dynamic contrast-enhanced MR imaging acquisition.22 The role of rR as a surrogate measure of BBB integrity in MS has not been evaluated. The purpose of this study was to compare rR in SPMS subgroups with and without cognitive impairment. We hypothesized that NAWM rR would be lower in cognitively impaired compared with nonimpaired patients with SPMS, reflecting a more advanced disease state. We also hypothesized that rR would be higher in WM lesions compared with NAWM.
Materials and Methods
Patient Cohort
The study was performed in accordance with our institution's guidelines for human research. Written informed consent was obtained for all imaging studies. Patients with clinically diagnosed SPMS were prospectively recruited from tertiary referral clinics. Two senior neurologists (20 years of experience) screened potential subjects to ensure they fulfilled the revised McDonald criteria. Exclusion criteria included patients with a history of drug/alcohol abuse, disease modifying drug or steroid use within the last 6 months, premorbid psychiatric history, head injury with loss of consciousness, concurrent medical diseases (eg, cerebrovascular disease), and MR imaging or contrast agent contraindications. Thirty-six patients with secondary-progressive MS fulfilled the screening criteria and were included in the study. Demographic data obtained included age, sex, years of education, and disease duration. Expanded Disability Status Scale assessment and cognitive testing was completed by a senior neurologist. No Expanded Disability Status Scale threshold was applied to patient eligibility. Neurologic examination, Expanded Disability Status Scale, and neurocognitive assessments were completed in order, on the same day within 6 hours of each other.
Imaging Protocol
Imaging parameters included volumetric T1 turbo field-echo (TR/TE/flip angle: 9.5 ms/2.3 ms/12°; number of averages: 1; FOV: 24 cm; matrix size: 256 × 164; section thickness: 1.4 mm); proton attenuation/T2 (TR/TE/flip angle: 2900 ms/10.7 ms/90°; FOV: 23 cm; matrix: 256 × 261; section thickness: 3 mm); field-echo echo-planar imaging DSC (for rR calculation) (TR/TE/flip angle: 1610 ms/30 ms/60°; FOV: 22 cm; section thickness: 4 mm; matrix: 128 × 128; in-plane voxel size: 1.7 × 1.7 mm; no gap; signal bandwidth: 1260 Hz/pixel). Ten milliliters of gadobutrol (Gadovist; Bayer, Toronto, Canada) (1 mmol/mL) was administered by a power injector at a rate of 5 mL/s followed by a 25-mL bolus of saline at 5 mL/s. Sixty volumes were acquired at 1.6-second intervals with the injection occurring at the 10th volume. DSC acquisition covered 10 cm (25 sections at 4 mm per section) and extended from the cerebral convexity to the midbrain level. Acquisition placement was supervised by an experienced neuroradiologist (8 years of experience) to ensure consistent coverage across patients.
Image Analysis
Gray matter, WM, and CSF were segmented from T1-weighted scans by use of a previously validated tissue segmentation method.23 Segmented regions were imported into Analyze 8.0 (Analyze AVW, Rochester, Minnesota),24 and WM lesion regions of interest were manually drawn. Brain parenchymal and WM lesion fractions were calculated as previously described.25 NAWM regions of interest were selected from within the WM tissue by use of four 16-voxel blocks located in anterior and posterior regions of both hemispheres. All WM lesion and NAWM regions of interest were subsequently co-registered to the equivalent DSC-MR imaging datasets by means of the rigid body algorithm of Statistical Parametric Mapping version 8 (SPM8; Wellcome Department of Imaging Neuroscience, London, United Kingdom). Contrast enhancement was systematically evaluated by use of a cross-reference tool by comparing FLAIR and proton attenuation/T2 lesions with precontrast and postcontrast imaging.
rR was calculated within each region of interest by use of in-house software (MR Analyst version 4.0) developed in Matlab (MathWorks, Natick, Massachusetts).22 In brief, selected DSC perfusion datasets were preprocessed by inspecting signal intensity versus time curves for outlier data points. Spurious points were identified by visual inspection and replaced with interpolated values. The first 2 dynamic phases were automatically omitted because magnetization cannot be assumed to have reached steady-state this early in the series. For each region of interest and each DSC image, the T2* relaxation rate was determined by evaluating the change in signal intensity from baseline and assuming26:
 ΔR2*measured data were subsequently fitted to a γ-variate function to produce a theoretic first-pass ΔR2*theoretic curve, that is, one that was free of recirculation effects. The rR was calculated as described by Kassner et al27 as:
ΔR2*measured data were subsequently fitted to a γ-variate function to produce a theoretic first-pass ΔR2*theoretic curve, that is, one that was free of recirculation effects. The rR was calculated as described by Kassner et al27 as:
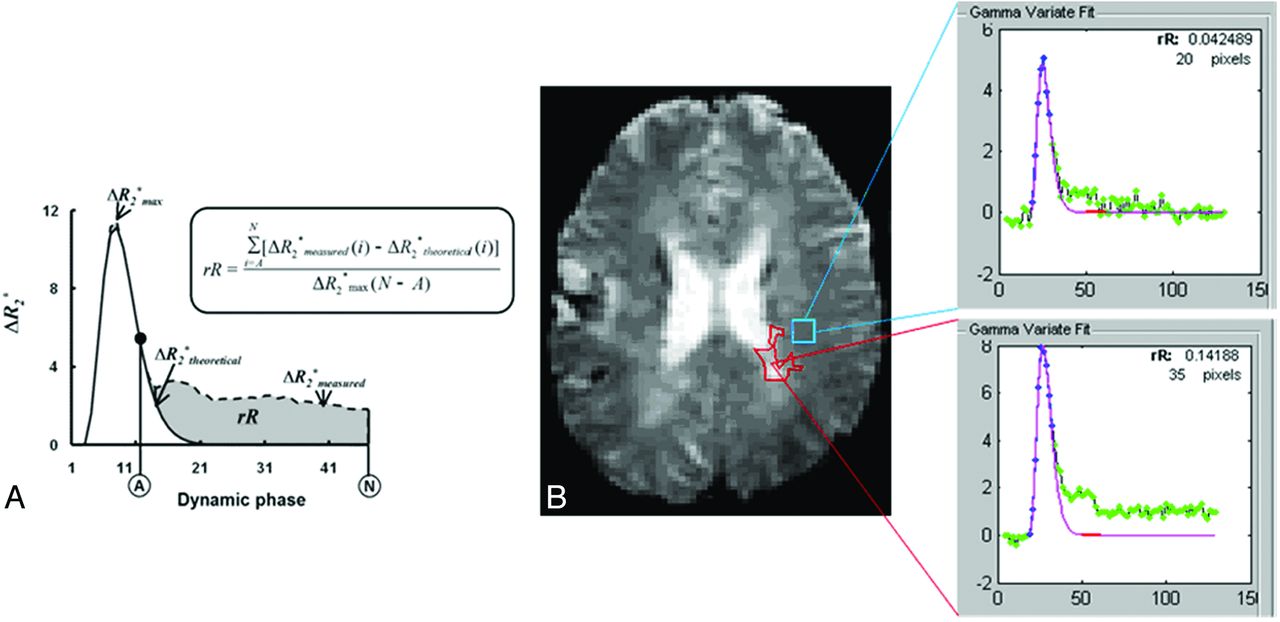
 where ΔR2*max is the maximum of ΔR2*theoretical, A is the dynamic phase corresponding to the onset of the recirculation phase measured at half-height of the descending aspect of the ΔR2* curve, and N is the final dynamic phase (Fig 1). Mean WM lesion rR and NAWM rR were determined for each patient by calculating the weighted average over WM lesion and NAWM regions of interest, respectively.
where ΔR2*max is the maximum of ΔR2*theoretical, A is the dynamic phase corresponding to the onset of the recirculation phase measured at half-height of the descending aspect of the ΔR2* curve, and N is the final dynamic phase (Fig 1). Mean WM lesion rR and NAWM rR were determined for each patient by calculating the weighted average over WM lesion and NAWM regions of interest, respectively.

A, Estimation of rR by use of the ΔR2* versus time curve measured from the DSC regions of interest (ΔR2*measured) as well as its γ-variate fit (ΔR2*fit). ΔR2*max is the maximum of ΔR2*theoretical. A is the dynamic phase corresponding to the onset of the recirculation phase measured at half-height of the descending aspect of the ΔR2* curve, and N is the final DSC phase. B, Example of rR measurement: case 733, section 11, perfusion scan. MS lesion (red region of interest) and NAWM (blue region of interest) and rR calculation results. rR for WM lesion is 0.142; rR for NAWM region is 0.042.
Cognitive Assessment
Cognitive assessments were performed by a neuropsychiatrist (20 years of experience) by use of an MS-specific neurocognitive tool, which is a 90-minute neurocognitive test proposed by an expert panel for clinical monitoring and research.28 The Minimal Assessment of Cognitive Function in Multiple Sclerosis is a comprehensive and efficient assessment tool consisting of 7 neuropsychological tests: Paced Auditory Serial Addition Test [working memory/processing speed], Symbol Digit Modalities Test [processing speed], California Verbal Learning Test, 2nd edition [verbal memory], Brief Visuospatial Memory Test, revised [visuospatial memory], Delis-Kaplan Executive Function System [executive function], Controlled Word Association Test [verbal fluency], and judgment of line orientation [visuospatial perception].Impairment on an individual test was defined as scoring >1.5 standard deviations below normative data from healthy controls. Beck Depression Inventory and the Expanded Disability Status Scale were also obtained.
Statistical Analysis
Univariate comparisons of demographic data for impaired and nonimpaired groups were performed by use of the Mann-Whitney rank sum test. Demographic data were expressed as mean (SD) for continuous variables such as age, education, and disease duration; median with interquartile range for categorical variables such as the Beck Depression Inventory and the Expanded Disability Status Scale; and proportions for binary data such as sex. Segmented regional data for brain parenchymal fraction, gray matter fraction, WM fraction, and WM lesion fraction were similarly compared. The 10th and 90th percentile values for rR distribution of each group were calculated, and values beyond these limits were excluded. For each cognitive test, potentially confounding factors of age, sex, years of education, disease duration, Beck Depression Inventory score, Expanded Disability Status Scale, brain parenchymal fraction, WM fraction, WM lesion fraction, and gray matter fraction were compared. Potential confounders with P values <0.3 (On-line Table) were included in further multivariate logistic regression. All statistical analyses were performed in SigmaStat3.5 (Systat Software, San Jose, California).
Results
There were 36 patients, with a mean (SD) age of 55.9 ± 9.3 years; 13 of 36 (36%) were male. Mean (SD) years of education and disease duration were 15.3 (2.6) and 20.4 (10.0). Median (IQR) for the Beck Depression Inventory and the Expanded Disability Status Scale were 8 (5–11) and 6.5 (6.0–7.0). Mean (SD) brain parenchymal fraction, WM fraction, WM lesion fraction, and gray matter fraction were 80.6 (4.1), 36.7 (3.0), 1.4 (1.2), and 41.5 (2.4), respectively. A highly significant difference between NAWM rR and WM lesion rR was present for all patients (P < .001; Fig 2). No enhancing WM lesions were present in either SPMS subgroup.

rR values of NAWM and WM lesion.
No significant differences between NAWM rR in impaired and nonimpaired patients were observed for the Brief Visuospatial Memory Test (P = .161), judgment of line orientation (P = .493), California Verbal Learning Test (P = .669), or Delis-Kaplan Executive Function System (P = .680) impairment. NAWM rR was significantly lower in impaired patients than in nonimpaired subjects for the Symbol Digit Modalities Test (P = .007), Controlled Word Association Test (P = .008), and Paced Auditory Serial Addition Test (P = .024) (On-line Table). The mean WM lesion fraction was higher in impaired patients (0.02) than in nonimpaired (0.01) for all tests (Symbol Digit Modalities Test: P = .020; Controlled Word Association Test: P = .014; and Paced Auditory Serial Addition Test: P = .033). No significant correlation was found between NAWM rR with brain parenchymal fraction (ρ = 0.010; P = .955), WM fraction (ρ = 0.187; P = .272), WM lesion fraction (ρ = −0.260; P = .124), or GM fraction (ρ = −0.295; P = .080).
After adjusting for confounders (Table 1), significant NAWM rR reduction persisted in impaired patients for the Symbol Digit Modalities Test (P = .023) and Paced Auditory Serial Addition Test (P = .047) (Table) but not for the Controlled Word Association Test impairment (P = .13). Figure 3 illustrates the distribution of rR values of NAWM for impaired and nonimpaired Symbol Digit Modalities Test and Paced Auditory Serial Addition Test groups. The Paced Auditory Serial Addition Test and Symbol Digit Modalities Test in impaired patients demonstrated a 3.2- and 4.6-year longer disease duration than in their nonimpaired counterparts. The difference did not however reach clinical significance (P = .3 and P = .6, respectively).
Outcomes of multivariate logistic regression analyses for NAWM rR after controlling for potential confounders

rR values of NAWM are significantly lower in impaired than in nonimpaired groups by use of A, the Symbol Digit Modalities Test (P = .007), and B, the Paced Auditory Serial Addition Test (P = .024).
The Expanded Disability Status Scale demonstrated an inverse correlation with NAWM rR (correlation coefficient = −0.319, P = .075).
Discussion
NAWM rR reduction was present in patients with secondary-progressive MS with poor performance on the Paced Auditory Serial Addition Test and Symbol Digit Modalities Test representing deficits in processing speed and working memory. NAWM rR values were significantly lower in impaired patients persisting after correction for potential confounding factors. Secondarily, WM lesion rR was higher than NAWM for all patients irrespective of cognitive impairment and in the absence of overt contrast enhancement.
Acute inflammation and BBB permeability in RRMS, manifesting as enhancing lesions, are linked with clinical and cognitive disability. The progressive phase of MS, however has a distinct disease pathogenesis compared with the acute or relapsing-remitting phases.29,30 SPMS is characterized by progressive axonal degeneration with clinical and cognitive disability but little lesion enhancement. A number of explanations for these findings are offered. Concepts of balanced inflammation, activation of endogenous neuroprotection mechanisms,15,16 entrapped inflammation behind intact or repaired BBB,6 and continued neurodegeneration independent of inflammation17 were previously proposed. Zeis et al15 demonstrated that genes known to be involved in anti-inflammatory and protective mechanisms are upregulated more regularly than pro-inflammatory mechanisms in NAWM in progressive MS. Correlation between brain atrophy and cognitive impairment increases with longer disease duration and SPMS subtype, in which impairment is reported in 50% of patients.2,3,18 In the present study, therefore, the association between cognitive impairment as a marker of disease severity and rR reduction as a surrogate marker of reduced measurable inflammation is expected. Supporting the association between disease duration, increased disability, and inflammation is the observed negative correlation between NAWM rR and disease severity (measured by the Expanded Disability Status Scale) in the present study.31 Additionally, cognitively impaired patients demonstrated longer disease duration than did cognitively nonimpaired patients, though this did not reach statistical significance.
Information processing speed and working memory are the most affected cognitive domains in patients with MS.3,32 The Symbol Digit Modalities Test and Paced Auditory Serial Addition Test have been shown in large series to be sensitive indicators of impairments in these domains.33 Both the Symbol Digit Modalities Test and Paced Auditory Serial Addition Test correlate with several brain imaging findings such as lesion volume and central cerebral atrophy.34⇓–36 The correlation expectedly increases with disease duration and SPMS subtype reflecting greater disease burden and axonal degeneration.18 Previous studies also show that NAWM abnormalities, even independent of lesion location, may correlate with cognition response.37 NAWM abnormalities measured by diffusion-weighted MR imaging also predict the speed of information deficits in MS.3,14 Our study, like others,3 highlights the need for longitudinal study of associations between NAWM abnormalities and cognitive impairment.
In RRMS, contrast enhancement indicates increased risk of relapses and may also be associated with long-term dysfunction.38 However, contrast enhancement is weakly correlated with clinical attacks39 and is age-dependent.40 For enhancement to be present, a critical but unknown degree of BBB permeability must be present. Prior quantitative analysis of enhancement demonstrates the dose and time dependency of enhancement and the relative insensitivity of qualitative designation of enhancement.41 rR as a surrogate marker of permeability was first studied in brain tumors19,20 and Moyamoya syndrome.21 More recently, rR was shown to strongly correlate (r = 0.67) with an established measure of BBB permeability (KPS) in acute ischemic stroke.22 Relative recirculation has the advantage of being extracted from standard DSC-MR imaging acquisitions without the need for a further contrast injection required for KPS determination. This is particularly important given the relationship between increasing contrast use and nephrogenic systemic fibrosis.42 Additionally, unlike KPS, the technique is model-free, with no need to obtain an input function avoiding a potential source of noise,43 as recently described.44 Last, rR provides a surrogate measure of BBB permeability as a continuum as compared with the current “binary” view of contrast enhancement as present or absent.
The study is limited by a relatively small sample size. As an exploratory study, we analyzed a strictly homogeneous selection of patients with secondary-progressive MS, controlling for multiple potentially confounding structural parameters. Pragmatically, because of high lesion load, NAWM was selected from the bilateral centrum semiovale, representing the largest WM region available for interrogation. Cognition represents a complex interplay of multiple domains that cannot be captured by a single region of interest at any location. However, injury to the centrum is strongly associated with neurocognitive dysfunction in leukoaraiosis,45 carbon monoxide poisoning,46 and trauma,47 potentially mediated by “disconnection” of important projection and association fibers.45 However, despite these limitations, significant results were obtained for the Paced Auditory Serial Addition Test and the Symbol Digit Modalities Test, both sensitive indicators of information processing speed and working memory. Although perfusion and permeability techniques offer potential useful adjuncts to conventional imaging for monitoring disease activity, they are affected by recent bouts of acute inflammation, disease-modifying drugs, and steroid use. These limitations may limit their applicability in relapsing-remitting MS subgroups as the result of the heterogeneous nature of treatment and inflammation present but are less of a concern within the secondary-progressive MS subgroup. We limited our focus to patients with secondary-progressive MS because of the higher rate of cognitive impairment and relative stability of the disease. Future studies would benefit from control comparison and well-controlled relapsing-remitting MS cohorts. Nevertheless, the results appear clinically meaningful, warranting further exploration of the association between rR, cognition, disease progression, and treatment response. If an association is found, rR could be a useful target for future pharmacologic and rehabilitative treatment strategies.
Conclusions
Significant NAWM rR reduction exists in cognitively impaired patients with SPMS, localizing to the domains of processing speed and working memory.
Footnotes
Disclosures: Andrea Kassner—RELATED: Grant: Canada Research Chair, Comments: Salary award and research allowance. Anthony Feinstein—UNRELATED: Grants/Grants Pending: MS Society of Canada;* Payment for Lectures (including service on speakers bureaus): Speakers honoraria paid to me from Merck Serono, Biogen, Teva, and Novartis; Royalties: Cambridge University Press. Richard Aviv—RELATED: Grant: MS Society,* PSI,* (*money paid to institution).
REFERENCES
- Received November 8, 2012.
- Accepted after revision December 19, 2012.
- © 2013 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.