
Article Figures & Data
Figures
- FIG 1.
Flow-chart to identify target lesions for CE (A), non-CE (B), and “mixed” (C) tumors. * the size condition for measurable disease is: ≥10 mm on 3 ⊥ planes for 3D images with thin slice (more often applied to CE disease), or ≥ 10 mm on in-plane ⊥ diameters and visible on ≥2 slices for 2D images with thicker slice (more often applied to non-CE disease). Of note, these conditions apply to trials employing bidimensional measurements for treatment response assessment, while for trials employing volumetric segmentations various strategies can be applied for the identification of target lesions (please refer to the dedicated paragraph in the main text). ° “mixed” tumors is short for “tumors with both CE and non-CE components”. † in mixed tumors, up to a total of 4 target lesions is allowed (i.e., x + y ≤ 4).
- FIG 2.
Guidelines and tips for bidirectional “2D” measurements. The measurement protocol for target lesions with 3D images and 2D imaging (A) is used both to verify that the lesion meets the criteria for “measurable disease” and to obtain measurements to calculate the tumor burden. Measurements in CE tumors (B) should not include the surgical cavity or cystic areas, and should avoid areas where the lesion shows necrotic features or is not distinguishable from post-surgical meningeal thickening. In non-CE tumors (C), the presence of infiltrative disease with unclear boundaries can pose a serious challenge when performing measurements. If possible, slices where the tumor shows more defined margins should be preferred for target lesion measurements. In “mixed” tumors (D), the CE lesions lie within the boundaries of non-CE lesions. CE and non-CE target lesions should be measured separately and not necessarily on the same plane/slice. Then, longitudinal changes in CE- and non-CE tumor burden are tracked in parallel to define the response category.
- FIG. 3
Schema for determining radiographic treatment response assessment as per RANO 2.0. To assess MR/PR, the change in tumor burden should be compared to the baseline MRI, while for PD it should be compared to the nadir. In clinical trials applying the “mixed” tumor criteria, the whole evaluation should be performed in parallel for both the CE and the non-CE tumor burden at each timepoint in order to assign the response category (e.g., PD, SD, PR, …), then the overall response category is assigned based on both CE and non-CE categories: PD+SD/MR/PR/CR=PD; MR/PR+SD=MR/PR; CR+SD/MR/PR=SD/MR/PR; SD+SD=SD (see text for details). ° the additional categories preliminary and durable “minor response” (MR: > –50% and < –25% 2D or > –65% and < –40% 3D) should be taken into consideration, only for non-CE disease. * confirmation scans obtained after ≥4 weeks to confirm PD can be waived in the following scenarios: in CE tumors ≥3 months after RT completion and if the treatment does not include agents highly associated with PsP; in the evaluation of non-CE progression in non-CE tumors or mixed tumors (as PsP is typically contrast-enhancing). Confirmation scans after ≥4 weeks to confirm durable MR/PR/CR are always required. If a patient is lost to follow-up (censored) before obtaining a confirmation scan (when required), the last timepoint showing preliminary CR/PR/MR/PD is classified as SD.
- FIG 4.
RANO 2.0 evaluations in example cases of newly-diagnosed CE glioblastoma. In case A, radiographic findings are stable (stable disease, SD) for 13.1 months from baseline, in the absence of measurable disease around the resection cavity. The appearance of a new measurable CE nodule after ≥12 weeks after RT completion (at 16.8 months in this case) classifies PD generally without the need of a confirmatory scan (unless clearly required by the trial), and the study treatment is stopped. In case B, the first follow-up scan shows early progressive disease (PD) <12 weeks after RT completion, “preliminary PD” (prel. PD) is annotated, the patient is kept on treatment, and a confirmation scan is obtained after ≥4 weeks. After confirmation of PD, the treatment is stopped and the confirmed PD (conf. PD) event is backdated to the day of preliminary PD. The time interval between the post-RT baseline scan and the date of confirmed PD corresponds to the time of progression (TTP). In case C, the first follow-up scan shows early PD <12 weeks after RT completion, annotated as preliminary PD. The confirmation scan after >4 weeks shows substantially stable findings, with no further size increase of the target lesion, therefore the preliminary PD timepoint is reclassified as pseudoprogression (PsP), and the patient is kept on treatment.
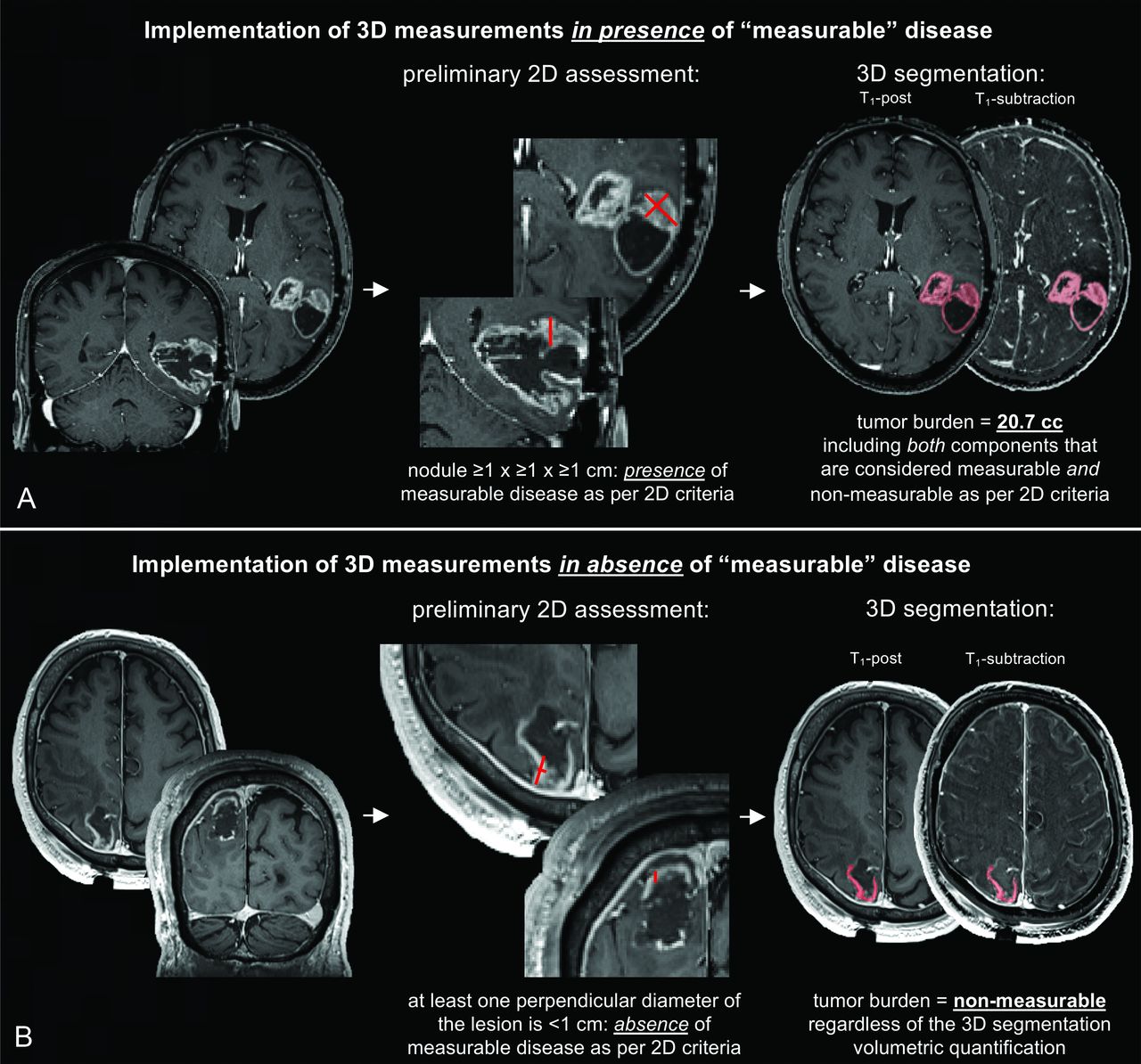
- FIG 5.
Proposed implementation of volumetric (3D) assessments. A preliminary evaluation should be performed to confirm the presence of measurable disease according to the classic bidimensional criteria. If 2D-defined measurable disease is present, the volumetric tumor burden may be computed by including the whole segmentation of the appropriate tissue (e.g., only CE tissue for CE tumors) which comprises both 2D-defined measurable components and 2D-defined non-measurable components (A). A quality check should always be performed by the reader to correct errors in the segmentation, for instance to exclude vascular structures or healthy meningeal tissue. If 2D-defined measurable disease is absent, the volumetric tumor burden should be set to “non-measurable”, regardless of the 3D segmentation (B). In the cases shown, T1-subtraction maps were used to only include in the segmentation voxels that showed increased T1-weighted signal when comparing post- to pre-contrast T1-weighted normalized images.





Tables
RANO 2.0 overview Baseline Newly diagnosed tumors Post-RT scan Recurrent tumors Pre-Tx scan Tumor components to evaluate CE tissue In all tumors Non-CE tissue - In non-CE tumors- In “mixed” tumors with CE + non-CE components- Optional in CE tumors for trials using agents that affectvascular permeability (e.g., antiangiogenic) Measurement technique Sum of bidimensional products or volumetric segmentations Thresholds applied to target lesions CR complete disappearance of all lesions PD ≥ +25% in sum of bidimensional productsor ≥ +40% in volume PR ≤ –50% in sum of bidimensional productsor ≤ –65% in volume MRa ≤ –25% and > –50% in sum of bidimensional productsor ≤ –40% and > –65% in volume SD criteria for CR / PR / MR / PD are not met Confirmatory scans (performed after >4 weeks) For PD - Mandatory for CE tumors ≤12 weeks from RT- Optional for CE tumors >12 weeks from RT (recommended for agentsb highly associated with PsP) - Unnecessary for non-CE tumors For CR/PR Mandatory for all tumors at all timepoints RANO 2.0 categories Complete Response (CR) – compare to baseline disappearance of target and non-target lesions sustained for ≥4 weeksa and no new lesionsb and clinical status is stable or improved and off corticosteroids (or on physiologic replacement dose) Partial Response (PR) – compare to baseline at least 50% decrease in tumor burden with 2D measurements, or 65% with 3D measurements, sustained for ≥4 weeksa,e and no newly-measurable lesionsb,c,d and clinical status is stable or improved and corticosteroid dose is stable compared to baseline (or on physiologic replacement dose) Minor Response (MR, only applicable to non-CE disease) – compare to baseline 25% to 50% decrease in tumor burden with 2D measurements, or 40% to 65% with 3D measurements, sustained for ≥4 weeksa and no newly-measurable lesionsb,c,d and clinical status is stable or improved and corticosteroid dose is stable compared to baseline (or on physiologic replacement) Progressive Disease (PD)f – compare to nadir at least 25% increase in tumor burden with 2D measurements, or 40% with 3D measurements, with or without confirmation scan after ≥4 weeksg or appearance of newly-measurable lesionsb,c,d or appearance of leptomeningeal disease or clinical deterioration not ascribable to steroid dose reduction or other causes apart from the tumor or failure to return for evaluation as a result of death or clinical deterioration Stable Disease (SD) all scenarios that do not meet criteria for CR, PR, MR, or PD. e.g., stable radiographic findings without clinical deterioration. Note:—CE indicates contrast-enhancing; CR, complete response; MR, minor response; PD, progressive disease; PsP, pseudoprogression; PR, partial response; SD, stable disease.
↵a Confirmation scans after ≥4 weeks to confirm durable MR/PR/CR are always required. If confirmed, MR/PR/CR is backdated to the date of preliminary MR/PR/CR. If a patient is lost to follow-up (censored) before confirmation, preliminary CR/PR/MR is considered SD.
↵b Disregard new non-CE lesions unequivocally ascribable to post-RT.
↵c Either new measurable lesions or previously non-measurable lesions that became measurable and grew ≥5x≥5 mm.
↵d For CE-tumors, only CE lesions should be considered.
↵e In mixed tumors, the assessment should be performed in-parallel for both CE and non-CE components, then combined.
↵f Corticosteroid dose increase alone does not define PD.
↵g Confirmation scans for PD can be waived: in CE tumors >3 months after RT completion not treated with agents highly associated with PsP; in the evaluation of non-CE progression in non-CE tumors or mixed tumors.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- ABBREVIATIONS:
- STANDARDIZED BRAIN TUMOR IMAGING PROTOCOL (BTIP) AND RADIOGRAPHIC READ PARADIGMS
- OVERVIEW OF UPDATES IN RANO 2.0
- DEFINITIONS OF MEASURABLE, NON-MEASURABLE, AND TARGET LESIONS (FIGURE 1)
- METHODOLOGY FOR 2D MEASUREMENTS (FIGURE 2)
- STEP-BY-STEP GUIDE TO RANO 2.0 RADIOGRAPHIC READS
- ADDITIONAL NOTES ON THE EVALUATION OF CE AND NON-CE DISEASE
- CORRESPONDENCE BETWEEN 2D AND 3D MEASUREMENTS
- CLINICAL DETERIORATION AND CORTICOSTEROID USE
- CONCLUSIONS
- Footnotes
- REFERENCES
- Figures & Data
- Supplemental
- Info & Metrics
- Responses
- References