Abstract
SUMMARY: Radiographic assessment plays a crucial role in the management of patients with central nervous system (CNS) tumors, aiding in treatment planning and evaluation of therapeutic efficacy by quantifying response. Recently, an updated version of the Response Assessment in Neuro-Oncology (RANO) criteria (RANO 2.0) was developed to improve upon prior criteria and provide an updated, standardized framework for assessing treatment response in clinical trials for gliomas in adults. This article provides an overview of significant updates to the criteria including (1) the use of a unified set of criteria for high and low grade gliomas in adults; (2) the use of the post-radiotherapy MRI scan as the baseline for evaluation in newly diagnosed high-grade gliomas; (3) the option for the trial to mandate a confirmation scan to more reliably distinguish pseudoprogression from tumor progression; (4) the option of using volumetric tumor measurements; and (5) the removal of subjective non-enhancing tumor evaluations in predominantly enhancing gliomas (except for specific therapeutic modalities). Step-by-step pragmatic guidance is hereby provided for the neuroradiologist and imaging core lab involved in operationalization and technical execution of RANO 2.0 in clinical trials, including the display of representative cases and in-depth discussion of challenging scenarios.
ABBREVIATIONS:
- BTIP
- Brain Tumor Imaging Protocol
- CE
- Contrast-Enhancing
- CNS
- Central Nervous System
- CR
- Complete Response
- ECOG
- Eastern Cooperative Oncology Group
- HGG
- High-Grade Glioma
- IDH
- Isocitrate Dehydrogenase
- IRF
- Independent Radiologic Facility
- KPS
- Karnofsky Performance Status
- LGG
- Low-Grade Glioma
- MR
- Minor Response
- mRANO
- Modified RANO
- NANO
- Neurological Assessment in Neuro-Oncology
- ORR
- Objective Response Rate
- OS
- Overall Survival
- PD
- Progressive Disease
- PFS
- Progression-Free Survival
- PR
- Partial Response
- PsP
- Pseudoprogression
- RANO
- Response Assessment in Neuro-Oncology
- RECIST
- Response Evaluation Criteria In Solid Tumors
- RT
- Radiation Therapy
- SD
- Stable Disease
- Tx
- Treatment
Gliomas are the most common malignant primary brain tumors1 and have few effective therapies2,3. Overall survival (OS) is considered the definitive benchmark for determining treatment efficacy in gliomas, but can be clouded by several confounding factors – particularly in single-arm phase I-II trials – including age, tumor size, molecular status and neurological status, and off-study therapies before or after the treatment of interest4,5. To gain a more accurate understanding of the value of a given treatment, earlier radiographic endpoints are desirable, including objective response rate (ORR) and progression-free survival (PFS)6.
Starting in 2010, the Response Assessment in Neuro-Oncology (RANO) Working Group developed updated response criteria for high- (RANO-HGG)7 and low-grade gliomas (RANO-LGG)8, aiming to enhance the reliability and comparability of response assessments in clinical trials. In 2017, “modified” RANO criteria (mRANO)9 were introduced after years of data collection and experience with the original RANO. mRANO introduced new concepts that are now integrated into the RANO 2.0 criteria10, including the use of the post-radiotherapy (post-RT) MRI as baseline scan in newly diagnosed glioblastoma, volumetric equivalent thresholds for response, the removal of non-contrast-enhancing (non-CE) areas evaluation in glioblastoma, and the requirement for confirmation scan to distinguish progression from pseudoprogression (PsP) – the latter being limited to the first 3 months after RT completion in RANO 2.0 or limited to agents at high risk of PsP (e.g., immunotherapies).
Since the 2021 classification of CNS tumors11, based on combined histological and molecular characteristics, often blurs the traditional distinction between HGGs and LGGs, RANO 2.0 guidelines10 propose unified criteria for all gliomas, based on recent data from clinical trials12,13. This article presents a summary of changes and a guide for how to operationalize RANO 2.0 in clinical trials.
STANDARDIZED BRAIN TUMOR IMAGING PROTOCOL (BTIP) AND RADIOGRAPHIC READ PARADIGMS
RANO 2.0 recommends the use of the standardized glioma BTIP14,15 for clinical trials (Online Supplemental Data), which features parameter-matched pre- and post-contrast 3D T1-weighted images with high spatial resolution (≤1.5 mm isotropic), and either 2D (with ≤4 mm slice thickness) or 3D (≤1.5 mm isotropic) T2-weighted and T2-weighted FLAIR images15. 3D T2w and T2w-FLAIR images are encouraged, if available, as they allow better multiplanar reconstruction, tilt adjustment, image registration and volumetric segmentation, which may be preferred in slower growing LGGs as some evidence shows better inter-reader agreement compared to 2D measurements16. Although not included in the RANO evaluations, it is encouraged for clinical trials to collect standardized DSC perfusion acquisitions as part of the imaging protocol15,17.
In addition to the acquisition protocol, the radiographic read paradigm should also be standardized for clinical trials. Later stage clinical trials often require a central review of imaging studies at an independent radiologic facility (IRF) for determination of both eligibility and radiographic response18. Eligibility reads in recurrent trials should confirm disease progression before the enrollment10, while eligibility reads to rule out the presence of contrast-enhancement (CE) in LGG, multifocal disease, or lesions larger than a certain size may also be performed if required by the particular trial. For response, the IRF should adopt a specific read paradigm in collaboration with the sponsor, which will dictate standardized procedures for the reading queue and for the adjudication design, as previously described18 (Online Supplemental Data). According to different reading queue designs, images can be presented either simultaneously or sequentially, and the corresponding timepoints can be displayed either in chronological or randomized order, either with a “locked” modality or a “hybrid” modality (Online Supplemental Data).
OVERVIEW OF UPDATES IN RANO 2.0
Improvements to RANO (Table 1) were based on consensus recommendations agreed upon by a panel of expert neuroradiologists, neuro-oncologists, neurologists, neurosurgeons, radiation oncologists, and imaging scientists, based on RANO-HGG7, RANO-LGG8, and mRANO9 recommendations, practical considerations, and data gathered from clinical trials12. Importantly, RANO 2.0 allow a degree of flexibility, depending on the trial and sponsor needs, and provide standardized language to be incorporated into the protocol document.
Main features of RANO 2.0
Baseline Scan
For newly diagnosed glioblastoma, the first post-RT scan (21-35 days after RT completion) should be used as a reference baseline for response assessment, not the post-surgical or the pre-RT scan. While these scans may be considered in the clinical practice, they should not be evaluated in RANO reads for clinical trials. This recommendation is based on the fact that post-surgical pre-RT scan is typically performed prior to trial enrollment, therefore frequently off study protocol, and is often contaminated by post-surgical changes which can confound the assessment of disease burden. More importantly, subsequent analyses have demonstrated that tumor shrinkage19 and PFS12 are better correlated with OS using the first post-RT scan as a reference. Additionally, this scan is often used as a reference in clinical practice due to uncertain radiographic changes during chemoradiation (i.e., possible PsP). Since the radiographic endpoint in the newly-diagnosed setting is typically PFS, the first post-RT scan should also be used as baseline in trials testing RT schemes and/or treatments concomitant with RT to better mitigate issues related to identification of disease progression. The post-surgical MRI acquired within 72 hours after surgery should still be used to evaluate post-surgical complications and extent of resection.
Also in trials for newly diagnosed gliomas that do not involve RT, such as some LGG trials, the MRI acquired up to 72 hours post-surgery is not recommended as a baseline for treatment response assessment. Instead, a pre-treatment (pre-Tx) scan should be acquired and used as a baseline, with a standardized timing (defined in the study protocol) with regards both to the day of surgery, to allow sufficient time for post-surgical changes to resolve, and to the day of treatment initiation, to minimize interval tumor growth prior to the start of therapy (≤14 days between the pre-Tx scan and treatment initiation).
For recurrent gliomas, a pre-Tx scan should be used as baseline, with a standardized time interval before the start of treatment. The time interval should be as short as possible to minimize the degree of tumor growth taking place between the pre-Tx scan and the start of the treatment20, and should always be ≤14 days and preferably ≤1 week10. For trials testing re-irradiation in the recurrent setting, the choice of the baseline scan (pre- or post- re-irradiation) should be selected depending on the radiographic endpoint (ORR or PFS), noting that post-RT changes can complicate response assessment probably even more so in the recurrent setting.
Type of Tumor Components to Evaluate (CE and/or Non-CE)
RANO 2.0 acknowledges three radiographic presentations of gliomas: CE tumors, non-CE tumors, and “tumors with both enhancing and non-enhancing components” (“mixed” gliomas for brevity). Typical glioblastomas presenting as predominantly enhancing lesions are considered CE tumors, whereas tumors that are largely non-enhancing and only present spots/nodules of enhancement should be categorized as “mixed” (e.g., some grade 3 IDH-mutant gliomas). These three radiographic presentations correspond to dedicated RANO 2.0 rules for response assessment. The choice between applying the “CE tumor” rules or the “mixed tumor” rules should be prospectively defined and uniformly applied across all enrolled patients within a trial, depending on the expected radiographic features of the enrolled patients as per the inclusion/exclusion criteria. A clinical trial enrolling patients with tumors that are expected to present as “mixed” may choose to adopt the dedicated criteria and uniformly apply them to all patients, regardless of the case-by-case radiographic appearance. As an example, some recent trials decided to evaluate both CE and non-CE components in recurrent grade 3 astrocytomas (NCT02796261) and in diffuse midline gliomas (NCT05009992).
For all tumors (CE, non-CE, and mixed) the changes in CE components are crucial to establish treatment response, including either the size change of existing CE areas and/or the appearance of new CE lesions. On the other hand, assessing changes in non-CE components is required for non-CE tumors and mixed tumors, but is not required for CE tumors such as glioblastoma (although optional for trials testing agents that are expected to significantly reduce vascular permeability – e.g., anti-angiogenic medications). Data suggests that the evaluation of non-CE areas in glioblastoma does not provide much value, adds complexity and costs, and does not improve the association between PFS and OS12,21.
Measurement Technique
Either bidirectional diameters (“2D measurements”) or volumetric assessments (“3D measurements”) can be used in RANO 2.0. With 2D measurements, the tumor burden is computed by adding the products of the two perpendicular diameters of each target lesion (i.e., sum of bidirectional products). 3D measurements are based on lesion segmentation, whether manual, semi-automated, or fully automated (when available). All segmentations should be formally approved by the human reader. Within a given trial, 2D or 3D measurements should be chosen a priori and applied consistently.
Thresholds for Response and Progression
The 2D thresholds for response and progression in RANO 2.0 are unchanged from previous RANO, while 3D thresholds are adopted from mRANO. Radiographic progressive disease (PD) or preliminary PD is defined as a 25% (2D measurements) or a 40% (3D measurements) increase in tumor burden. Partial response (PR) or preliminary PR is defined as a 50% (2D measurements) or a 65% (3D measurements) decrease in tumor burden. Finally, a minor response (MR) category is applicable only to non-CE components, if a tumor burden decrease is observed in the range of 25–50% (2D) or 40–65% (3D).
Use of Confirmation Scans for Response and Progression
For response (MR/PR/CR), confirmation scans after ≥4 weeks to demonstrate durable response are required, consistent with all previous RANO guidelines. As for PD, confirmation scans were required for mRANO, and optional in the original RANO-HGG in case of uncertainty or borderline progression. RANO 2.0 only requires confirmation of progression ≤12 weeks after RT completion. Additionally, confirmation of progression is optional if progression occurs >12 weeks after RT completion, but strongly advised in trials testing agents that are expected to be highly associated with PsP (e.g., immunotherapies). In the recurrent setting there can be significant tumor growth between the baseline or screening scans and the start of treatment which can “artificially” trigger a PD categorization at the first follow-up even if the treatment is effective20. Ideally, a “hyperacute” baseline scan should be acquired 1-2 days before treatment initiation to negate the influence of this interval growth20. However, if this is not possible, an alternative approach would be to consider confirmation of progression for lesions showing progressive disease at the first follow-up scan. The conditions for when and if to use confirmation scans for progression should be dictated by the sponsor and articulated in the study protocol and imaging charter. Of note, after PD confirmation, the date of PD should be backdated, as explained in the following paragraphs.
DEFINITIONS OF MEASURABLE, NON-MEASURABLE, AND TARGET LESIONS (FIGURE 1)
Measurable disease is defined as one or more lesions with clear margins and meeting a minimal size threshold. On 3D images, a measurable lesion should have ≥10 mm diameters in all three perpendicular planes. On 2D images, the size threshold is met if both in-plane diameters are ≥10 mm on ≥2 consecutive slices. These criteria apply to both CE and non-CE disease, although in CE tumors only CE lesions can be considered as “target” lesions.

Flow-chart to identify target lesions for CE (A), non-CE (B), and “mixed” (C) tumors. * the size condition for measurable disease is: ≥10 mm on 3 ⊥ planes for 3D images with thin slice (more often applied to CE disease), or ≥ 10 mm on in-plane ⊥ diameters and visible on ≥2 slices for 2D images with thicker slice (more often applied to non-CE disease). Of note, these conditions apply to trials employing bidimensional measurements for treatment response assessment, while for trials employing volumetric segmentations various strategies can be applied for the identification of target lesions (please refer to the dedicated paragraph in the main text). ° “mixed” tumors is short for “tumors with both CE and non-CE components”. † in mixed tumors, up to a total of 4 target lesions is allowed (i.e., x + y ≤ 4).
Non-measurable disease includes all lesions not meeting the criteria for measurable disease, either because they are smaller or because their margins are ill-defined. Of note, measurements should never include cystic or necrotic portions, nor the resection cavity. For instance, the rim enhancement surrounding the surgical cavity or surrounding cystic components should be categorized as non-measurable, unless presenting an enhancing nodule that meets the criteria for measurable disease.
Target lesions are measurable lesions selected to be used for the longitudinal quantification of tumor burden. If the baseline scan shows multiple measurable lesions, ≥3 lesions (≥4 for “mixed” tumors) can be selected as target lesions and their size is combined to quantify the overall tumor burden. Identifying multiple components as target lesions may also be acceptable in cases where a single lesion features two or more separated measurable components connected by non-measurable components (e.g., two clear distinct CE nodules located along a pericavitary rim enhancement, or two well-demarcated non-CE nodules connected by infiltrative components with unclear boundaries). In case of >3 measurable lesions, larger lesions are preferred as targets, or preferably lesions that showed a size increase on the eligibility read (for recurrent tumors). If a simultaneous presentation or a “hybrid” reading queue is used, the choice of target lesions can also be informed by their on-study growth.
Non-target lesions should be evaluated or monitored, but their size is not incorporated in the assessment of the overall tumor burden. If previously non-measurable lesions grow and become measurable, they can become target lesions, and their size is then incorporated into the overall tumor burden.
METHODOLOGY FOR 2D MEASUREMENTS (FIGURE 2)

Guidelines and tips for bidirectional “2D” measurements. The measurement protocol for target lesions with 3D images and 2D imaging (A) is used both to verify that the lesion meets the criteria for “measurable disease” and to obtain measurements to calculate the tumor burden. Measurements in CE tumors (B) should not include the surgical cavity or cystic areas, and should avoid areas where the lesion shows necrotic features or is not distinguishable from post-surgical meningeal thickening. In non-CE tumors (C), the presence of infiltrative disease with unclear boundaries can pose a serious challenge when performing measurements. If possible, slices where the tumor shows more defined margins should be preferred for target lesion measurements. In “mixed” tumors (D), the CE lesions lie within the boundaries of non-CE lesions. CE and non-CE target lesions should be measured separately and not necessarily on the same plane/slice. Then, longitudinal changes in CE- and non-CE tumor burden are tracked in parallel to define the response category.
Measurement Protocol
When 2D measurements are used, the overall tumor burden should be calculated as the sum of all bidimensional products of target lesions. Target lesions should be measured on the plane and the slice where they display the largest area (the “main” plane and slice), and the reader should measure the lesion in additional planes (with 3D imaging) or slices (with 2D imaging) to confirm that the conditions for “measurable” disease are met (Figure 2A).
CE Tumors
Only CE regions should be included in the measurements of target lesions. Voxels representing the surgical cavity or cystic components should be excluded from the diameters (Figure 2B), as well as areas with T1-hyperintensity on pre-contrast images. T1-weighted digital subtraction maps may be helpful to avoid including areas of inherent T1-shortening in the CE-measurements9. Additionally, readers should avoid measuring tumor size on slices that contain excessive necrotic components or where the boundaries between neoplastic CE tissue and post-surgical meningeal thickening/scarring are not clear (Figure 2B). As discussed, non-CE disease is not included in the tumor burden computation for CE tumors.
Non-CE Tumors
Areas of non-CE disease should be identified on T2w and T2w-FLAIR images, and can be used as target lesions as long as they meet the criteria for “measurable disease” in non-CE and mixed tumors. Non-CE components should be measured on the sequence where they appear the largest (T2w or T2w-FLAIR), as long as consistency across timepoints is observed. As mentioned, in order to meet criteria for “measurable disease”, lesions should not only display a certain size, but also present clearly defined margins. Since non-CE disease can show infiltrative growth patterns with poor demarcation, slices where the non-CE lesion shows more clearly defined borders should be preferred for the 2D measurements (Figure 2C). However, when tumors present with predominantly infiltrative components, it is reasonable to select target lesions with margins that are, to some extent, indistinct, rather than classifying the whole lesion as “non-measurable”.
“Mixed” Tumors
For mixed tumors with primarily non-CE disease and some measurable CE-components, both CE and non-CE areas should be evaluated separately, with separate target lesions. While CE disease is always localized within T2-hyperintense regions of the tumor and changes will frequently evolve consistently with any changes in non-CE tumor, both total CE- and non-CE tumor burden should be computed separately when evaluating radiographic response for each timepoint (Figure 2D).
Consistency Across Timepoints
When selecting and measuring target lesions, the reader may encounter challenging scenarios (e.g., Figure 2), and be forced to perform measurements that are, to some extent, arbitrary. This might include 2D measurements of an irregular lesion or 3D measurement of an infiltrating or partly necrotic lesion with boundaries that are not clearly defined. While standardization of MRI acquisitions helps with consistency, this issue is still quite common and the reader should attempt to maintain maximal consistency across timepoints in the selection of slices, also employing coregistration tools if available. Consistency may be further maximized by “simultaneous” or “hybrid” reading queue designs18 that allow the reader to adjust the measurements at different timepoints. Readers should clearly describe in the patient source document which images and slices were used for the measurements.
STEP-BY-STEP GUIDE TO RANO 2.0 RADIOGRAPHIC READS
No Measurable Disease at Baseline
If the baseline scan shows no measurable disease, the best possible response on subsequent imaging is SD (Figure 3). No objective responses (MR/PR/CR) can be obtained without a measurable target lesion at baseline. The lesion maintains SD if no new measurable disease is observed at follow-up time points. If the lesion develops new measurable disease, or if a non-measurable component (only CE components, in case of CE tumors) existed in the previous scan and grows sufficiently in comparison to the initial lesion size (i.e., ≥5 × ≥5 mm), the time point response is PD and the treatment is stopped if confirmation is not required for trial operation (Figure 4A) (i.e., if not explicitly required, then only after 12 weeks after RT completion or for non-CE disease). If a confirmation scan is required, the first scan showing progression is annotated as “preliminary PD”, and an additional MRI should be obtained after ≥4 weeks for glioblastoma or at the next scheduled follow-up as indicated in the trial design. Confirmed PD is assigned only if the confirmation scan shows an additional size increase of the measurable disease (≥25% with product of bidimensional 2D measurements or ≥40% with 3D volumetric segmentation compared to preliminary PD), in which case the treatment is stopped, and the day of PD is backdated to the day of preliminary PD. If the tumor does not continue to grow, the preliminary PD time point is considered a confirmed PsP (i.e., SD), the confirmation scan timepoint is annotated as SD, and the treatment is continued until additional evidence of PD compared to the date of confirmed PsP or the nadir after confirmed PsP.

Schema for determining radiographic treatment response assessment as per RANO 2.0. To assess MR/PR, the change in tumor burden should be compared to the baseline MRI, while for PD it should be compared to the nadir. In clinical trials applying the “mixed” tumor criteria, the whole evaluation should be performed in parallel for both the CE and the non-CE tumor burden at each timepoint in order to assign the response category (e.g., PD, SD, PR, …), then the overall response category is assigned based on both CE and non-CE categories: PD+SD/MR/PR/CR=PD; MR/PR+SD=MR/PR; CR+SD/MR/PR=SD/MR/PR; SD+SD=SD (see text for details). ° the additional categories preliminary and durable “minor response” (MR: > –50% and < –25% 2D or > –65% and < –40% 3D) should be taken into consideration, only for non-CE disease. * confirmation scans obtained after ≥4 weeks to confirm PD can be waived in the following scenarios: in CE tumors ≥3 months after RT completion and if the treatment does not include agents highly associated with PsP; in the evaluation of non-CE progression in non-CE tumors or mixed tumors (as PsP is typically contrast-enhancing). Confirmation scans after ≥4 weeks to confirm durable MR/PR/CR are always required. If a patient is lost to follow-up (censored) before obtaining a confirmation scan (when required), the last timepoint showing preliminary CR/PR/MR/PD is classified as SD.

RANO 2.0 evaluations in example cases of newly-diagnosed CE glioblastoma. In case A, radiographic findings are stable (stable disease, SD) for 13.1 months from baseline, in the absence of measurable disease around the resection cavity. The appearance of a new measurable CE nodule after ≥12 weeks after RT completion (at 16.8 months in this case) classifies PD generally without the need of a confirmatory scan (unless clearly required by the trial), and the study treatment is stopped. In case B, the first follow-up scan shows early progressive disease (PD) <12 weeks after RT completion, “preliminary PD” (prel. PD) is annotated, the patient is kept on treatment, and a confirmation scan is obtained after ≥4 weeks. After confirmation of PD, the treatment is stopped and the confirmed PD (conf. PD) event is backdated to the day of preliminary PD. The time interval between the post-RT baseline scan and the date of confirmed PD corresponds to the time of progression (TTP). In case C, the first follow-up scan shows early PD <12 weeks after RT completion, annotated as preliminary PD. The confirmation scan after >4 weeks shows substantially stable findings, with no further size increase of the target lesion, therefore the preliminary PD timepoint is reclassified as pseudoprogression (PsP), and the patient is kept on treatment.
Measurable Disease at Baseline followed by Progressive Disease
If the disease burden is “measurable” at baseline, any timepoint showing size increase ≥25% (2D) or ≥40% (3D) compared to nadir or baseline is labeled as either preliminary PD (if confirmation scans are required) or PD (if there is no need for confirmation scans) (Figure 3; Table 2). In case a new measurable lesion is observed, this does not automatically determine PD. The scan is categorized as preliminary PD/PD only if the overall disease burden (including the measurements of the new lesion) exceeds ≥25% (2D) or ≥40% (3D) compared to nadir or baseline. The treatment is stopped only if confirmation scans are not required or if a confirmation scan (after ≥4 weeks) shows additional PD relative to the date of preliminary PD (Figure 4B). If the confirmation scan shows additional progression, PD is backdated to the day of preliminary PD. If the confirmation scan shows stable or improved findings, the timepoint exhibiting preliminary PD is labeled as “confirmed PsP” (Figure 4C; see No Measurable Disease at Baseline), and treatment is continued until further evidence of progression.
Summary of RANO 2.0 criteria
Measurable Disease at Baseline followed by Radiographic Response
Preliminary MR/PR/CR is assigned when a scan demonstrates a size reduction of tumor burden (computed from target lesions) below the corresponding threshold (PR: 50% 2D or 65% 3D; MR: 25% 2D or 40% 3D; CR: disappearance of all lesions) compared to baseline, and no new measurable lesions are observed (Figure 3; Table 2). A confirmed MR/PR/CR is then assigned only if the following scan (after ≥4 weeks) verifies the tumor has maintained shrinkage below the specific thresholds for MR/PR/CR compared to baseline. Unlike PD, MR/PR/CR always require confirmation scans to confirm response. The duration of response is determined from the time of initial response to disease progression. In case the nadir scan has no measurable disease, further PD will be assigned according to the same rules as in case of “No Measurable Disease at Baseline” (see above).
Measurable Disease at Baseline followed by Stable Disease
All scenarios that do not meet criteria for PD or MR/PR/CR are labeled as SD and treatment is continued. SD is also assigned in case the patient is lost to follow-up (censored) after unconfirmed MR/PR/CR or after unconfirmed preliminary PD (if confirmation of PD is required).
Follow-up after Confirmed Pseudoprogression
In case of previously confirmed PsP, any follow-up scans showing a ≥25% (2D) or ≥40% (3D) increase in tumor burden compared to either PsP or nadir after PsP should be labeled as confirmed PD. In this case, the treatment is stopped and no additional confirmation scans required, and the date of PD is not backdated (i.e., the date of the 2nd progressive disease event is the date of progression). A response after PsP (“PR/CR after PsP”) is possible only if the tumor burden meets the thresholds for response compared to baseline, not compared to the PsP timepoint where progressive enhancement was noted, similar to iRECIST recommendations22.
ADDITIONAL NOTES ON THE EVALUATION OF CE AND NON-CE DISEASE
Assessment of CE Disease
In CE tumors, CE tumor burden is quantified only with target lesions and then the response category is defined following the recommended thresholds. In non-CE tumors, the appearance of a new measurable CE lesion should define preliminary PD or PD (depending on whether a confirmation scan is required, which should be pre-specified in the study protocol).
Assessment of Non-CE Disease
In non-CE tumors, non-CE tumor burden is quantified with target lesions and then the response category is defined following the recommended thresholds. New areas of non-CE signal alterations should only be categorized as PD if they are not ascribable to obvious RT-induced changes. As this distinction is often very challenging and potentially arbitrary, we advise to only ascribe to RT those T2w/FLAIR signal alterations that can be unequivocally attributed to well-established radiographic patterns, such as findings typical of radiation leukoencephalopathy, which acknowledges “capping” of the ventricular horns and confluent homogeneous white matter hyperintensity without mass effect23.
In CE tumors, as mentioned, non-CE disease should not be assessed, apart from trials testing agents that significantly reduce blood-brain barrier permeability (e.g., anti-angiogenic agents), in which CE may not accurately reflect the actual tumor burden. In this case, no strict methodology is required for the evaluation of non-CE tissue in CE tumors. Two possible approaches may be adopted to evaluate non-CE components: diameters/segmentations as proposed for mixed tumors (see below), or a qualitative assessment (“worsened” vs “stable/improved”) similar to 2010 RANO-HGG7. Since CE tumors typically present extensive T2w/FLAIR hyperintese alterations with contamination from vasogenic edema, a qualitative approach may be preferred in these cases. The methodology should ultimately be agreed upon by the sponsor and the contract research organization18 and clearly stated in the imaging charter prior to the initiation of the trial.
Mixed Tumors
In “mixed” tumors, CE and non-CE tumor burden should be tracked separately, with dedicated target lesions, and both should be compared to the proposed thresholds at each timepoint. Then, if either one demonstrates PD, the overall response category is PD. If either one shows MR/PR/CR and the other one shows SD, the overall response category is MR/PR. CR is the overall response category only if both CE and non-CE disease show CR. Similarly, SD is the overall response category only if both CE and non-CE disease show SD. Importantly, the assessment of non-CE components in mixed tumors should not include vasogenic edema. While in typical mixed tumors (i.e., largely non-CE tumors with some CE foci) the vasogenic component of the T2w/FLAIR hyperintense signal is minimal, in cases with more pronounced blood-brain barrier breakdown the distinction between vasogenic edema and non-CE tumor tissue is not trivial and potentially arbitrary.
Leptomeningeal Disease
The appearance of new and clear leptomeningeal involvement is sufficient to determine PD, and can be evaluated on post-contrast T1w images and/or post-contrast T2w-FLAIR images (if acquired as a BTIP variation)15. Given the impact of this scenario, which would cause the treatment to be stopped and the patient to be put off-study, it is recommended to only indicate unequivocal and extensive leptomeningeal spread during radiographic reads.
CORRESPONDENCE BETWEEN 2D AND 3D MEASUREMENTS
The sum of bidirectional products (2D measurements) or the volume quantification following segmentation (3D measurements) are both valid approaches for the quantification of tumor burden in RANO 2.0. However, while the rules to operationalize 2D measurements are precisely stated and have been used in trials for decades, instructions to convert such rules to 3D measurements are not strictly dictated.
Measurable Disease
As previously discussed, 2D measurements dictate that measurable disease is defined as a lesion with either: three ≥10 mm perpendicular diameters (if 3D imaging is used), or two ≥10 mm in-plane perpendicular diameters on two adjacent slices (if 2D imaging is used). However, RANO 2.0 criteria do not clearly describe how to extrapolate these criteria to 3D. Indeed, volumetric lesion segmentation potentially allows measurement of lesions that would be classically considered non-measurable by 2D assessments. A clear example is the rim of enhancement surrounding a surgical cavity or surrounding a necrotic/cystic area where there is no nodule to define a clear target lesion in 2D. As such, there should be some guidance on best practices for when and how to use 3D measurements for the purposes of radiographic response assessment.
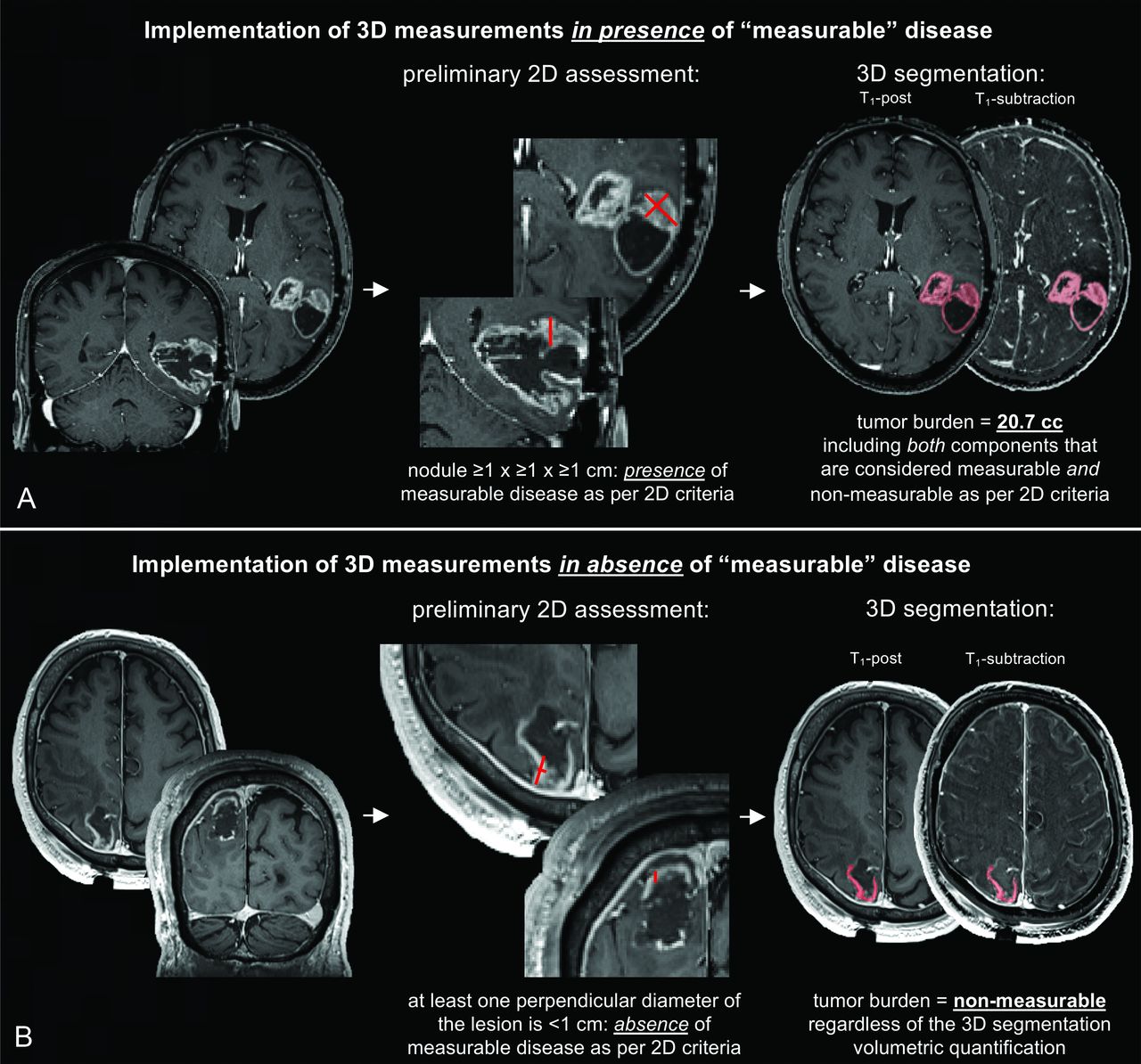
For multicenter clinical trials with a central read evaluation, it is advisable to confirm presence of measurable disease using 2D criteria, especially during eligibility reads at the local sites, followed by use of volumetric measurements centrally of all appropriate signal alterations (e.g., all CE tissue for HGG or all tumoral non-CE alterations in LGG) without distinction of measurable and non-measurable components (Figure 5A). Conversely, if baseline images do not exhibit a measurable lesion using 2D criteria, regardless of the volume on 3D segmentation, the scan should be considered to show no measurable disease (Figure 5B). This approach both preserves the historic definitions of measurable disease and is the most pragmatic solution, as editing 3D segmentations to precisely match 2D criteria would require additional, time-consuming and relatively arbitrary steps for the radiologist.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proposed implementation of volumetric (3D) assessments. A preliminary evaluation should be performed to confirm the presence of measurable disease according to the classic bidimensional criteria. If 2D-defined measurable disease is present, the volumetric tumor burden may be computed by including the whole segmentation of the appropriate tissue (e.g., only CE tissue for CE tumors) which comprises both 2D-defined measurable components and 2D-defined non-measurable components (A). A quality check should always be performed by the reader to correct errors in the segmentation, for instance to exclude vascular structures or healthy meningeal tissue. If 2D-defined measurable disease is absent, the volumetric tumor burden should be set to “non-measurable”, regardless of the 3D segmentation (B). In the cases shown, T1-subtraction maps were used to only include in the segmentation voxels that showed increased T1-weighted signal when comparing post- to pre-contrast T1-weighted normalized images.
Target Lesions
In cases of multifocal lesions, up to 3 measurable lesions can be selected as target lesions for 2D measurements. When this is translated to 3D volumetric measurements, one could decide to include only 2D-defined target lesions, target lesions and non-target lesions, or all disease that is thought to be present irrespective of lesion designation. In agreement with the previously proposed solution, it may be favorable to include all signal alterations in the segmentations as this would result in a more accurate overall estimate of tumor burden, would arguably result in a better inter-reader agreement, and would avoid partial segmentations that only include some of the lesions24.
Mixed Tumors
In mixed tumors with CE and non-CE components, CE lesions lie within non-CE lesions. Therefore, with 2D measurements, the diameters of non-CE lesions also include CE lesions, inevitably. Tumor segmentations allow to separately classify voxels as belonging to the CE area or the non-CE area. When 3D assessments are employed, it is advisable to obtain one segmentation for CE areas, and a separate segmentation for the whole T2-hyperintense lesion, which encompasses both CE and non-CE areas, for consistency with the 2D method.
General Recommendations
Overall, it is recommended that multicenter studies using an IRF for central review, or single center studies, utilize 3D measurements with the same software package for all patients to ensure consistency within the trial. Additionally, 3D measurements should preferably be applied to volumetrically acquired images to further limit the contributions of partial volume effects.
CLINICAL DETERIORATION AND CORTICOSTEROID USE
The assessment of clinical or neurological status and the change in corticosteroid dose are also required for the response assessment. Clinical deterioration not ascribable to steroid dose reduction or other causes apart from the tumor is sufficient to define PD, independently from radiographic findings and without the need for confirmation scans. This may be defined a number of ways, including KPS, ECOG, NANO, or simply “better”, “stable”, or “worse”, and should be clearly defined in the trial protocol and imaging charter.
Changes in corticosteroid dose are known to alter the degree of contrast enhancement25 and extent of cerebral edema26 and therefore should also be considered when evaluating radiographic response9,10. If a patient exhibits a response (CR/PR/MR) and corticosteroids are increased beyond 2 mg per day dexamethasone or equivalent compared to baseline, the response is downgraded to SD because steroids could explain the observed tumor shrinkage. Additionally, to qualify for CR, patients must be either off steroids or on physiological replacement dose, otherwise the response is downgraded to MR/PR if the corticosteroid dose is stable compared to baseline. Conversely, if a patient exhibits radiographic evidence of disease progression (PD) but steroid dose has been decreased relative to the nadir, the response should be changed to SD and the patient should continue treatment. Importantly, an increase in corticosteroid dose alone, without clinical or radiographic progression at the time of evaluation, does not dictate disease progression.
CONCLUSIONS
The RANO 2.0 criteria provide unified and improved rules for the standardized determination of radiographic response in adult gliomas on clinical trials. Neuroradiologists and imaging core labs should be aware of the aforementioned suggestions and operational recommendations to maximize the accuracy and reliability of identifying potential therapeutic effects in patients with adult gliomas.
Footnotes
Benjamin M. Ellingson and Francesco Sanvito contributed equally.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- Received May 6, 2024.
- Accepted after revision June 22, 2024.
- © 2024 by American Journal of Neuroradiology