
SUMMARY:
Temporal lobe epilepsy is a common form of epilepsy that is often associated with hippocampal sclerosis (HS). Although HS is commonly considered a binary assessment in radiologic evaluation, it is known that histopathologic changes occur in distinct clusters. Some subtypes of HS only affect certain subfields, resulting in minimal changes to the overall volume of the hippocampus. This is likely a major reason why whole hippocampal volumetrics have underperformed versus expert readers in the diagnosis of HS. With recent advancements in MRI technology, it is now possible to characterize the substructure of the hippocampus more accurately. However, this is not consistently addressed in radiographic evaluations. The histologic subtype of HS is critical for prognosis and treatment decision-making, necessitating improved radiologic classification of HS. The International League Against Epilepsy (ILAE) has issued a consensus classification scheme for subtyping HS histopathologic changes. This review aims to explore how the ILAE subtypes of HS correlate with radiographic findings, introduce a grading system that integrates radiologic and pathologic reporting in HS, and outline an approach to detecting HS subtypes by using MRI. This framework will not only benefit current clinical evaluations, but also enhance future studies involving high-resolution MRI in temporal lobe epilepsy.
ABBREVIATIONS:
- CA
- cornu ammonis
- DG
- dentate gyrus
- HS
- hippocampal sclerosis
- ILAE
- International League Against Epilepsy
- SRLM
- strata radiatum, lacunosum, and moleculare layers
- TLE
- temporal lobe epilepsy
Epilepsy is a prevalent and debilitating condition that affects nearly 50 million individuals worldwide.1 Among the various types of epilepsy, mesial temporal lobe epilepsy (TLE) is one of the most common and is frequently associated with hippocampal sclerosis (HS). Neuroimaging plays a crucial role in the evaluation of TLE, particularly in the diagnosis of HS. A positive imaging diagnosis of HS in TLE strongly predicts the success of surgical intervention in controlling seizures.2 Despite the critical importance of HS diagnosis on MRI, a wide range of reported sensitivity and specificity remains.
Traditionally, the diagnosis of HS relies on 3 main radiographic features: whole hippocampal atrophy, increased T2 signal, and/or loss of internal architecture.3 However, these features may not always correspond with the histologic patterns of HS and may fail to detect changes in specific subfields of the hippocampus.4 In some cases, epileptogenic hippocampi with microscopic alterations primarily limited to certain subfields may appear normal in signal and total volume on MRI.5 Therefore, subfield analysis is crucial for HS diagnosis in certain patients. High-resolution MRI can be used for subfield analysis, but it is not consistently addressed in radiographic evaluations, leading to underdiagnosis of HS.6
To capture the full range of histopathologic changes in HS, the International League Against Epilepsy (ILAE) has proposed a histologic grading system that categorizes HS into 4 distinct types: no HS, classic HS (type 1), cornu ammonis (CA) 1-predominant HS (type 2), and CA4-predominant HS (type 3).7 With advancements in MRI technology (e.g., improvements in acceleration techniques, head coil design, and increasing use of high-field MRI systems), a more detailed evaluation of the internal structure of the hippocampus is now possible. This review aims to explore the radiographic correlates of the ILAE subtypes of HS, introduce a grading system that fosters a harmonious integration of radiologic and pathologic reporting in HS, and outline an approach to detecting HS subtypes by using MRI.
OVERVIEW OF HIPPOCAMPAL ANATOMY
The MR diagnosis of HS is historically based on the altered volume and signal in the hippocampal formations and the loss of internal architecture. However, a significant proportion of epileptogenic hippocampi that have been reported to be normal in volume and signal on MRI have been shown to harbor subfield alterations on histopathologic assessment,8,9 which may be detectable with recent advances in MRI. In cases of HS, particularly type 2 or type 3, it is common for the total volume of the hippocampus to be relatively preserved. Therefore, a thorough understanding of hippocampal anatomy, which can be visualized by using routine high-resolution clinical MRI, is crucial for assessing the subtype of HS.
The hippocampus is a curved structure located in the medial temporal lobe that arcs around the midbrain on both sides of the brain. It is approximately 4.5 cm long and can be divided into 3 segments:
Anterior expanded head: this segment is transversely oriented and exhibits prominent elevations along the superior surface, referred to as hippocampal digitations.
Middle cylindrical body: this segment is sagittally oriented and curves around the midbrain.
Posterior tail: this segment is transversely oriented and tapers beneath the splenium.
The hippocampus has an interlocking bilaminar architecture composed of the CA (hippocampus proper) and the dentate gyrus (DG; fascia dentata), separated by the hippocampal sulcus. The hippocampal sulcus can be further divided into deep and superficial parts. The superficial part, known as the superficial hippocampal sulcus, is visible on the medial temporal surface. The deep part disappears during embryogenesis, leaving behind remnants that are often observed as hippocampal sulcus remnant cysts. With minor variations, the interlocking architecture of the CA and DG remains consistent throughout the entire length of the hippocampus.
Hippocampal Body
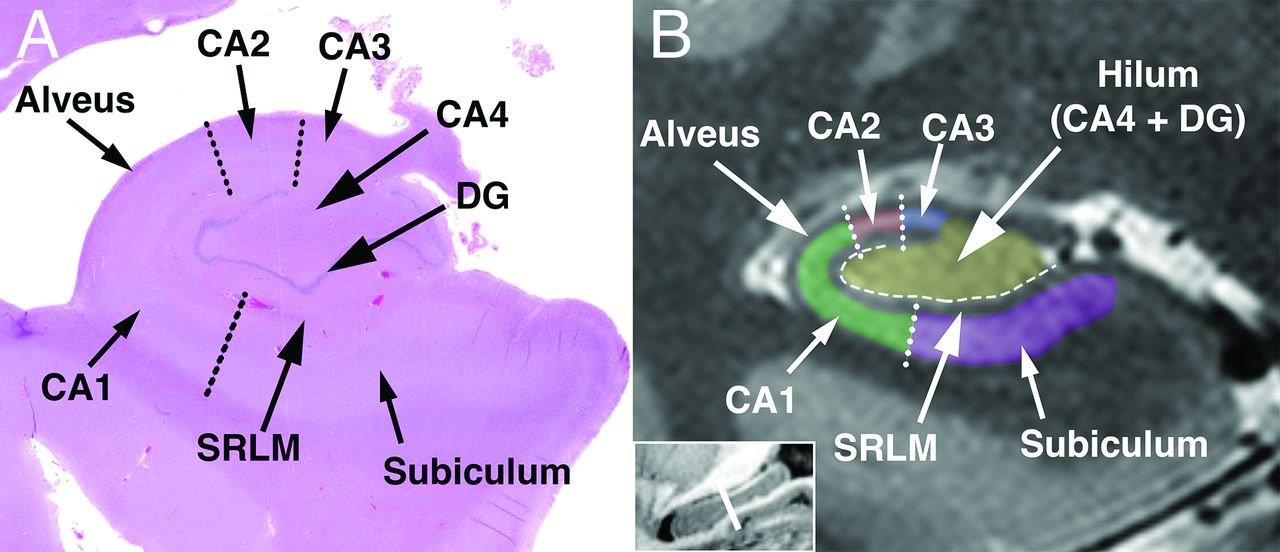
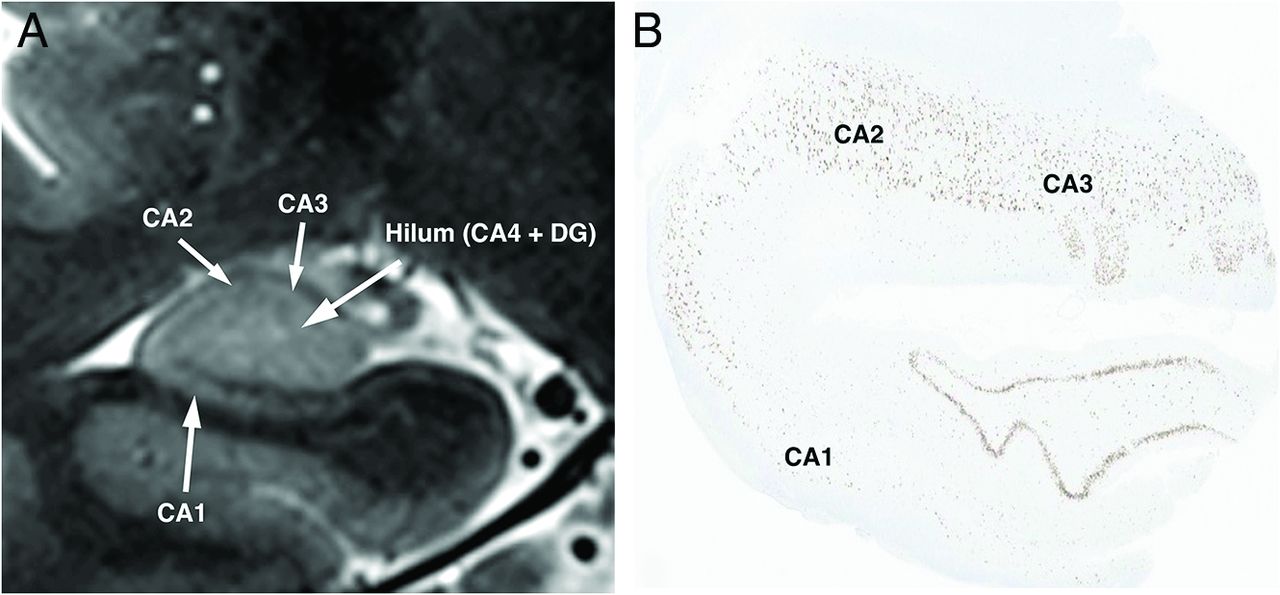
In coronal sections of the hippocampal body, the CA is divided into 4 subfields, specifically CA1–CA4 (Figs 1 and 2). CA1 represents the horizontal and lateral ascending portion of the CA, which extends laterally from the subiculum (Figs 1 and 2). The subiculum forms a transition between the neocortex of the parahippocampal gyrus and the hippocampal allocortex. It runs horizontally along the undersurface of the hippocampus and merges with CA1. CA2 is the superior-most curving subfield terminating in CA3. CA4 is located within the concavity of the hilum and is enveloped by the DG, distinguishing it from CA3. On routine clinical MRI, CA4 cannot be easily differentiated from the DG, and the 2 structures appear as a central homogeneous structure referred to as the hippocampal hilum (Figs 1 and 2).

Normal hippocampal anatomy. A, Coronal histologic section through the body of the hippocampus compared with (B) coronal 7T T2-weighted 2D turbo-spin-echo MRI. Dotted lines represent approximate subfield borders, and dashed line represents the location of the hippocampal sulcus.

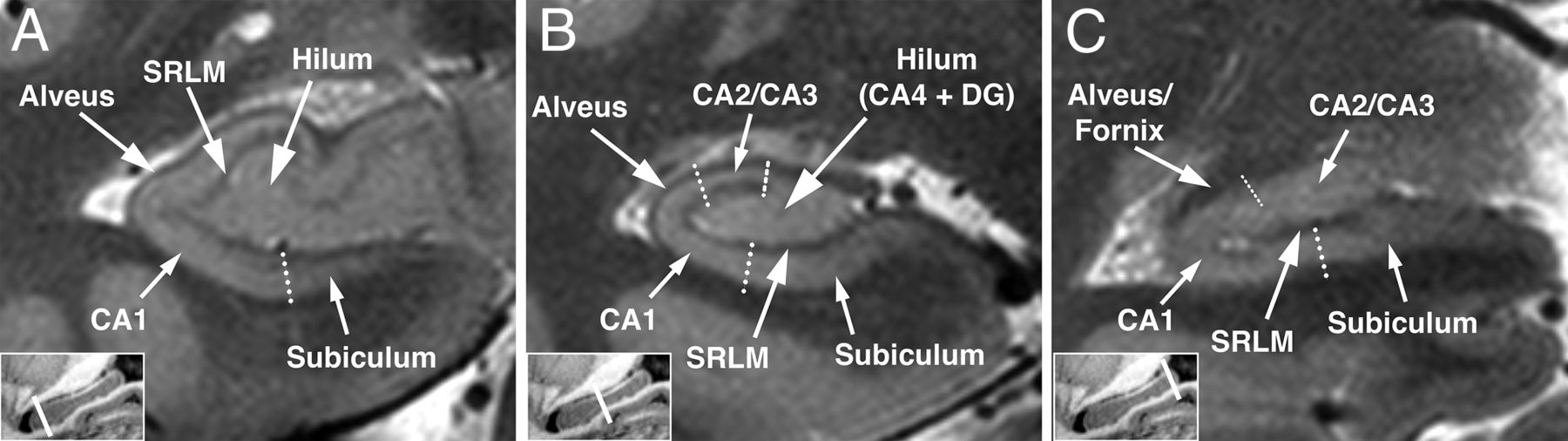
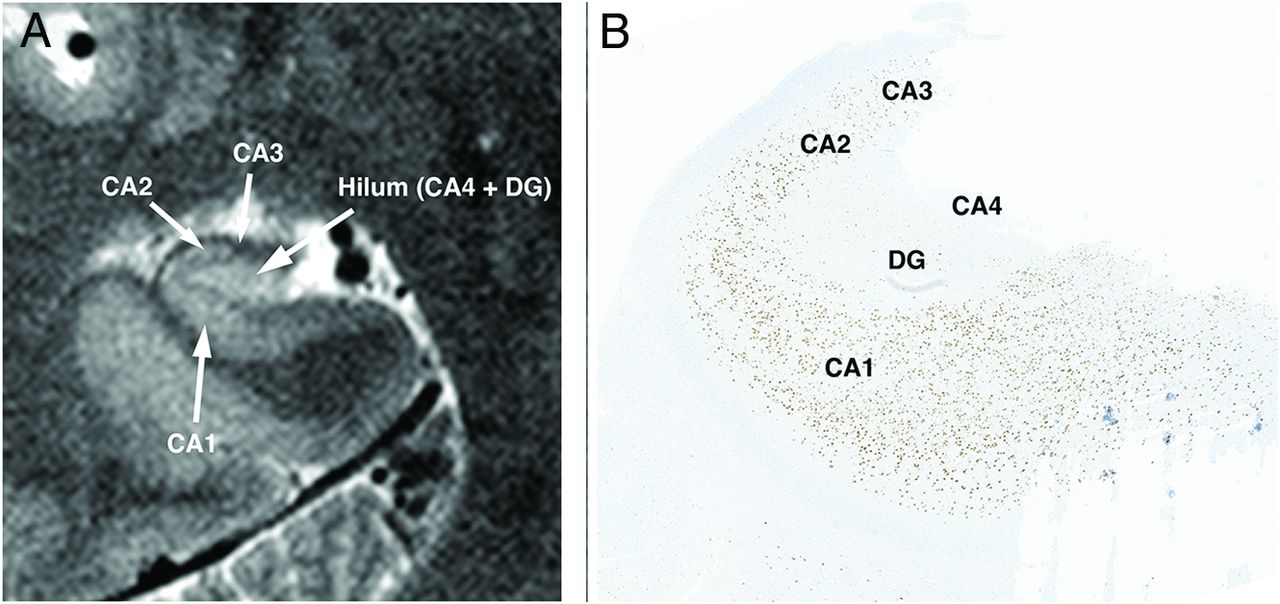
Normal hippocampal anatomy. Oblique coronal 7T T2-weighted 2D turbo-spin-echo through the hippocampus shows the normal hippocampal head (A), body (B), and tail (C).
The CA can be divided into 6 layers (outermost surface to deepest): the alveus, stratum oriens, stratum pyramidale, stratum radiatum, stratum lacunosum, and stratum moleculare. The outer surface along the ventricular interface is covered by the alveus, which consists of hippocampal and subicular efferent axons. The alveus converges into the fimbria. The deepest layer, the stratum moleculare, abuts the vestigial hippocampal sulcus. On MRI, the strata oriens and pyramidale form a thicker outer T2 hyperintense and T1 hypointense band of the CA, tapering from the CA1 to CA3 subfields (Fig 1B). The strata radiatum, lacunosum, and moleculare (SRLM) together create a thinner T2 hypointense and T1 hyperintense stripe that extends along the inner surface of the subiculum, CA1, CA2, and CA3, parallel to the hippocampal sulcus (Fig 1). SRLM is a defining boundary of the hippocampal subfields on MRI, separating the CA from the hippocampal hilum.
Hippocampal Head
On the most anterior coronal sections of the hippocampal head (Fig 2), the digitations are exclusively formed by the convolutions of CA. The DG, which is absent in the most anterior sections, becomes visible in midsections as 2 to 3 complete or incomplete rings surrounded by the undulating CA. In the most posterior sections through the head, the dentate appears as a single undulating oblong ring surrounding CA4. In the hippocampal head, the layered arrangement of the CA and dentate is essentially the same as that in the body. The distinct stripes of CA and dentate typically merge into a single band, as remnants of the hippocampal fissure are rarely observed.
Hippocampal Tail
The hippocampal tail tapers posteriorly, and its architecture is best observed in its anterior portions, specifically at the point where the fimbria and crus of the fornix intersect (Fig 2). The tail is composed of 3 distinct layers, namely the upper and lower bright bands, with a dark layer interposed between them. These upper and lower bright stripes represent the continuation of CA3 and CA1/subiculum, respectively, from the body of the hippocampus. Within the inner hypointense layer of the tail, remnants of the hippocampal sulcus can frequently be observed.
PATHOPHYSIOLOGY OF HS IN EPILEPSY
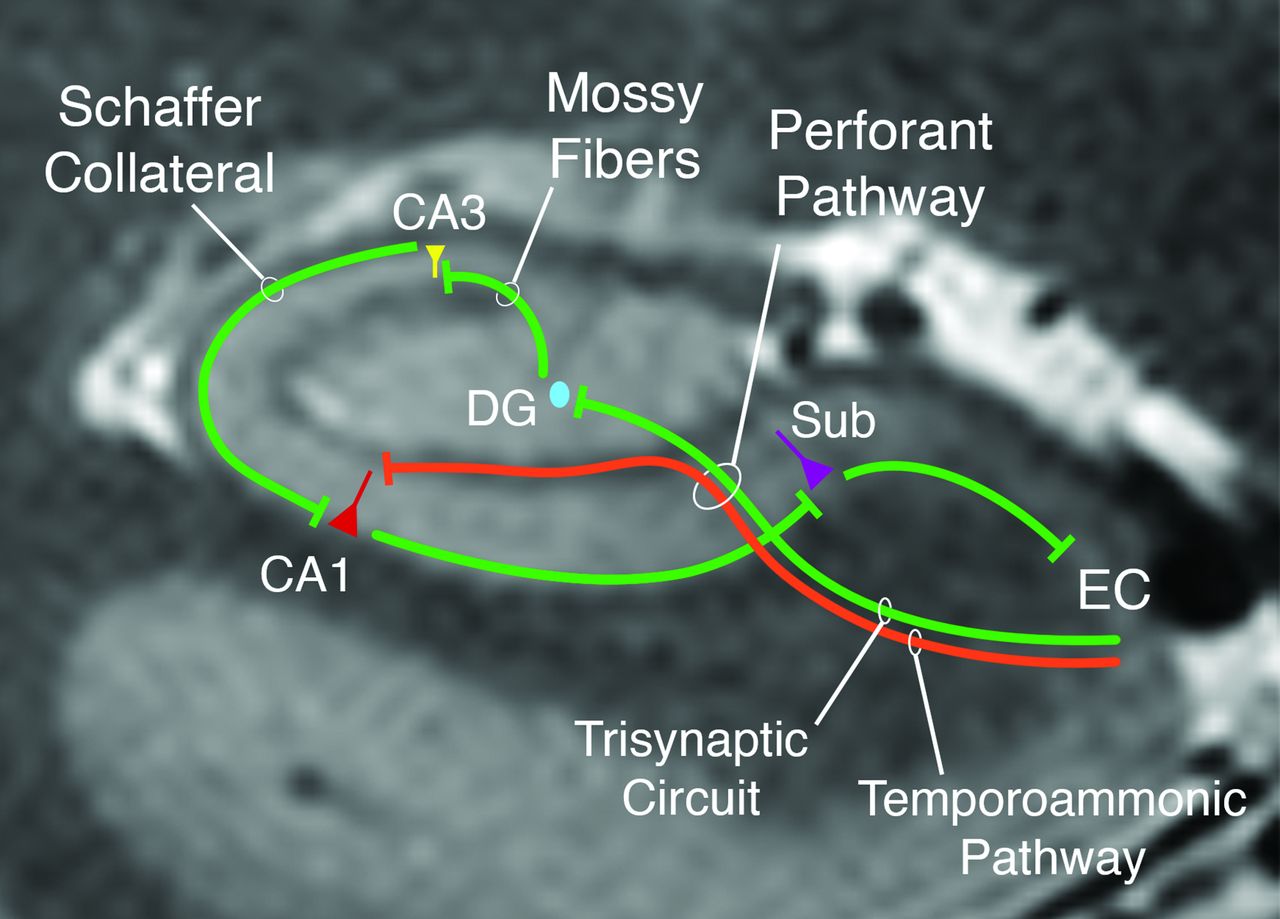
TLE tends to become more resistant to treatment over time due to the progression of seizure-induced damage in the hippocampus and synaptic reorganization. In pathologic specimens of patients with TLE, damage to both CA1 and CA4 is consistently present, although in varying proportions. This damage and reorganization in CA1 and CA4 regions are partly due to their intrinsically greater susceptibility to cellular hypoxia.10 The pathophysiology of HS primarily involves 2 distinct hippocampal circuits: the trisynaptic pathway and the temporoammonic pathway (Fig 3).

Illustration of the 2 primary hippocampal circuits implicated in hippocampal damage from temporal lobe epilepsy, the trisynaptic and temporoammonic pathways. The classic trisynaptic pathway projects from layer II of the entorhinal cortex (EC) to the DG via the perforant pathway for the first synapse. The second synapse is from the granule cells in the DG to the pyramidal layer of the CA3 region. The third synapse is formed by CA3 neurons projecting to CA1 neurons through Schaffer collaterals. Meanwhile, the temporoammonic pathway consists of monosynaptic connections from layer III of the EC projecting directly to the pyramidal layers of CA1. Sub = subiculum.
The trisynaptic pathway involves projections from the entorhinal cortex to the granule cells in the DG (via the perforant pathway), then to pyramidal neurons in CA3 (via mossy cell fibers), to the pyramidal neurons of CA1 (via Schaffer collaterals), and then to the subiculum. Synaptic reorganization of mossy fibers has been a major focus of research, because it is thought to contribute to hippocampal hyperexcitability through abnormal excitatory collaterals. Recently, paradoxical excitatory transformation of normally inhibitory CA1 pyramidal axons projecting to the subiculum has also been implicated.10,11 Disruption of the trisynaptic pathway, along with neuronal loss and reorganization in CA1, leads to simultaneous disinhibition and synchronization of spontaneous excitability in the subiculum, driving epileptogenesis in HS. The ensuing neuronal depletion is invariably paired with pronounced reactive astrogliosis, resulting in tissue hardening, historically known as Ammon horn sclerosis but now commonly referred to as HS (Fig 4).

Patterns of reactive astrogliosis on glial fibrillary acidic protein (GFAP) staining of hippocampal tissue. Hippocampal tissue in a patient with no HS shows a single GFAP staining reactive astrocyte (A, arrow). Moderate number of GFAP reactive astrogliosis is noted in a different patient with long-standing epilepsy (B, arrows) with decreased neuronal attenuation. Severe reactive astrogliosis characterized by attenuated meshwork of GFAP-labeled fine processes (C) in a hippocampal specimen of a patient with advanced ILAE type 1 HS.
Ongoing seizure activity and neuronal loss in CA4 also leads to mossy fiber sprouting into the granule cell layer in the DG. The presence of mossy fiber sprouting is typically absent in the pathologic specimens of patients with TLE without HS. Hyperexcitability of neurons in the granule cell layer seems to be directly linked to the extent of mossy fiber sprouting. It is believed that this aberrant circuit contributes to the development of epilepsy in HS by amplifying neuronal hyperexcitability.12 Therefore, surgical resection or ablation of the atrophic hippocampus, which includes the regions where mossy fiber sprouting occurs, is crucial for effectively managing epilepsy in patients with HS.
In addition to its role in the trisynaptic circuit, the perforant pathway also directly connects the entorhinal cortex not only to the DG, but also to all subfields of the hippocampal formation, including CA1. This temporoammonic pathway, characterized by weakly connected and functionally delimited direct entorhinal input (from layer III entorhinal cortical neurons via the perforant pathway) to CA1 (Fig 3), is believed to undergo a several-fold excitatory transformation in TLE, which potentiates CA1 pyramidal cell hyperexcitability through an independent mechanism. The up-regulation of the temporoammonic pathway, along with the paradoxically excitatory reorganization of CA1 pyramidal output, may constitute a highly efficient reverberating circuit for seizure propagation in the hippocampus.13
ILAE CLASSIFICATION OF HS IN EPILEPSY
The initial steps toward a consensus pathologic classification of HS were demonstrated by Blumcke et al.4 This study expanded upon previous attempts at quantitative pathologic HS classification by Wyler et al.14 Although practical, the Wyler classification lacked integration with clinical phenotypes and prevalent HS patterns. Building on the prior work by Blumcke et al,4 the ILAE issued an international consensus on the pathologic classification of HS in 2013 with 4 distinct HS subgroups identified.7
The most common HS type, affecting 60%–80% of surgical patients with TLE, is ILAE type 1. Type 1 is classified by the involvement of all hippocampal subfields, with CA1 often the most affected, but also with moderate or severe involvement of other subfields (Fig 5). Type 1 also includes the commonly described “classic” or “severe/total cell loss” described in radiologic and histologic studies of HS. Type 2 HS, on the other hand, exhibits predominant CA1 cell loss, but with minimal involvement of other subfields (Fig 6). This “CA1-predominant” pattern is less common, affecting 5%–10% of surgical patients with TLE. Type 3 HS is the least common, affecting 4%–7% of surgical patients with TLE. It is characterized by predominant cell loss in CA4 and DG, with minimal involvement of CA1, CA2, and CA3 (historical “end folium sclerosis”) (Fig 7). Type 3 HS may be more frequently present in cases of dual pathology, such as neocortical lesions or Rasmussen encephalitis.7 Finally, the “No HS” subgroup comprises approximately 20% of patients with TLE, with histopathology only showing reactive gliosis without significant neuronal cell loss.

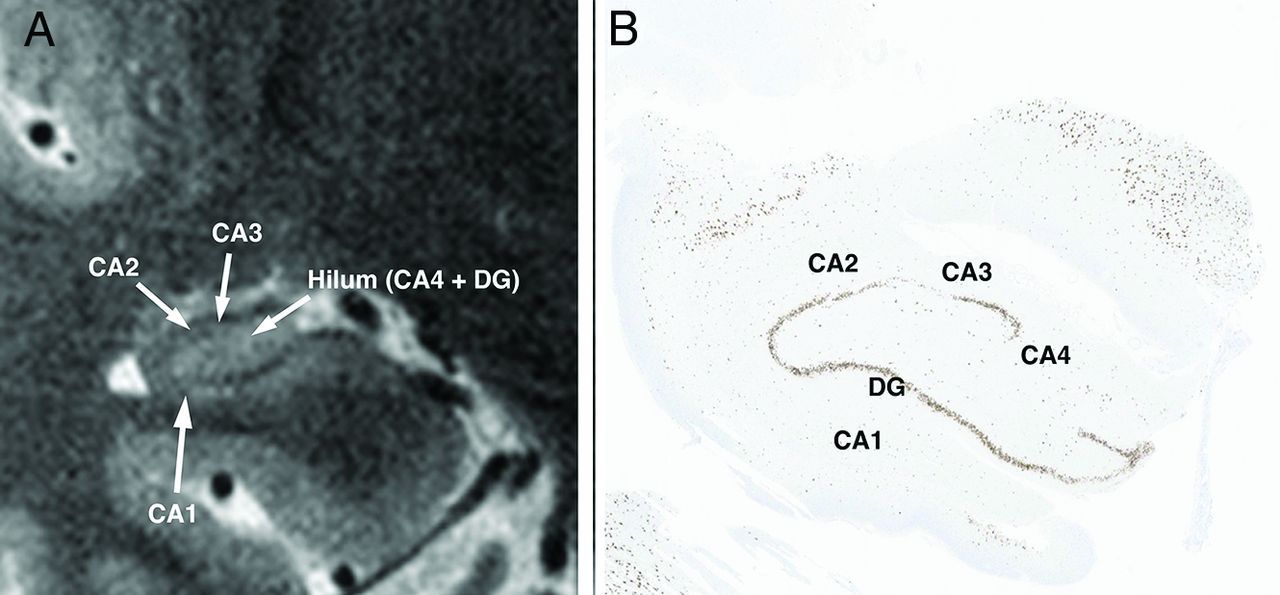
Type 1 ILAE HS. A, Oblique coronal T2-weighted image shows volume loss affecting CA1–CA3 and the hippocampal hilum. B, Microscopy by using neuronal nuclear (NeuN), a marker of neuronal cells, confirms the MRI findings with severe neuronal loss throughout CA1–CA4 along with neuronal loss in the DG.

HS ILAE type 2 (CA1-predominant neuronal cell loss and gliosis). A, Oblique coronal T2-weighted image shows atrophy of the CA1 segment of hippocampus on coronal T2-weighted MRI with loss of the normal tapering of CA1 from the CA1-subiculum junction to the CA1–CA2 junction. There is relative sparing of the hilum and other CA segments. B, Microscopy by using NeuN marker shows moderate neuronal loss limited to the CA1 sector with preserved neuronal attenuation in other CA sectors.

HS ILAE type 3 (hilar predominant neuronal cell loss and gliosis). A, Oblique coronal T2-weighted image shows atrophy of the hilum of hippocampus on coronal T2-weighted MRI, as evidenced by overall decrease in volume and height of the hilum. There is relative sparing of CA1–CA3, which show no substantial volume loss or loss of tapering of CA1–CA3. B, Microscopy by using NeuN marker shows moderate neuronal loss limited to the hilum region with preserved neuronal attenuation in CA1–CA3.
CLINICAL IMPLICATIONS OF THE ILAE CLASSIFICATION OF HS
The detection and classification of HS play a crucial role in the clinical management of drug-resistant temporal lobe epilepsy, influencing both presurgical evaluation and surgical decision-making. Mesial TLE associated with HS is a distinct epilepsy syndrome with characteristic clinical features, such as focal aware seizures (auras) associated with déjà vu, fear, phantosmia, and an increasing epigastric sensation, leading to a fixed stare, impaired awareness, and oral-alimentary automatisms.15 The duration of these events typically ranges from 30 to 60 seconds, followed by varying degrees of postictal confusion, fatigue, and amnesia for the event. Comorbid depression and anxiety are common. HS has been associated with material-specific memory impairment, with impaired verbal memory functions being the most common finding in cases of left-sided HS.16 Type 1 and 3 HS are also associated with more severe declarative memory impairments compared with type 2 HS.17 Routine interictal EEG often shows focal anterior temporal epileptiform discharges and/or regional temporal delta slowing.18 Type 1 HS is more frequently associated with bilateral tonic-clonic seizures.19 Types 2 and 3 HS have less specific clinical features, although they are more commonly associated with focal to bilateral tonic-clonic seizures, status epilepticus, and a family history of epilepsy.20 Type 3 HS is more likely to be associated with a second (dual) pathology.7 These factors may contribute to varying surgical outcomes among HS subtypes.20
The etiology of HS can be genetic, acquired, or a combination of both.7 Demographic data, such as sex, TLE side, age at epilepsy onset, seizure frequency, total estimated seizures, and age at surgery, have not consistently shown correlations with HS subtype. On the other hand, the age at the initial precipitating event (eg, febrile seizure, encephalitis, trauma, first seizure without precipitating injury, etc) significantly influences the HS subtype.7 Studies suggest that early-life epileptogenic neurotoxicity has more pronounced effects on the developing temporal lobes compared with the more resistant mature brain structures in older patients.21 This hypothesis is supported by the higher prevalence of type 1 HS in patients with an initial precipitating event at a younger age (median 2–3 years), whereas those with no HS are older at the time of the initial precipitating event (median 16 years). Type 2 and type 3 fall in between, with a median age at the initial precipitating event of 6 and 13 years, respectively.7
Surgical interventions, such as temporal lobe resection, yield better outcomes compared with medication alone in cases of drug-resistant TLE.22⇓⇓-25 In particular, patients with unilateral HS on MRI have particularly favorable surgical outcomes.8,26⇓-28 However, the frequency of favorable postsurgical outcomes is not universal across all HS subtypes, with higher rates of seizure freedom and Engel class I outcomes observed in type 1 HS compared with types 2 and 3.4,7,26 Postsurgical outcomes in TLE also have a relationship with postoperative memory and cognitive decline, and this aspect needs to be considered when advising patients before surgery. Individuals without HS generally exhibit better preoperative cognitive and memory functioning, which consequently places them at a greater risk of experiencing postoperative decline.29 Moreover, the specific type of HS may influence the degree of postoperative cognitive decline, as there is some evidence suggesting more pronounced verbal memory loss in patients with type 2 HS compared with those with types 1 and 3.17 However, the lack of standardized neuropsychological testing methods contributes to inconsistent findings on the postoperative cognitive impact.30 These differences in prognostication play a significant role in surgical decision-making, highlighting the value of using an MRI-based classification system for HS subtypes.
Patients with lesional TLE associated with HS are also favorable candidates for less invasive procedures, such as laser interstitial thermal therapy, which has been shown to decrease the risk of language (naming) morbidity31 and potentially reduce the risk of postoperative memory decline compared with more extensive surgeries like anterior temporal lobectomy.29 However, patients without HS may also have a favorable postoperative outcome with respect to seizure-related outcome following laser interstitial thermal therapy,28 although it is usually more effective when HS is present.32 Responsive neurostimulation may also be an option for patients with bilateral HS,4 dual pathology, or those at a higher risk of cognitive and memory decline after unilateral resection. Recently, there has been an increase in the use of thalamic deep brain stimulation for epilepsy, specifically targeting the anterior nucleus of the thalamus, which has been beneficial for patients with TLE.33,34 However, the effects of HS on deep brain stimulation are not fully understood, as some studies have shown changes in network stimulation effects in patients with severe HS.35,36 In summary, with the expanding array of surgical interventions for TLE, preoperative identification and categorization of HS are becoming increasingly important in guiding the selection of the most effective treatment strategy and minimizing postoperative cognitive deficits.
PROPOSED RADIOLOGIC TYPES CORRELATING WITH ILAE PATHOLOGY CLASSIFICATION
The proposed radiologic classification for HS was developed with the intention of closely aligning with the ILAE pathology classification (Table). The primary objective of MRI classification is to qualitatively assess hippocampal volume loss, including subfield analysis. To conduct hippocampal subfield analysis, one must have knowledge of the anatomic locations of the different subfields, as there are no distinct anatomic boundaries between many of these structures on MRI. The subfields evaluated during MRI analysis consist of CA1, CA2/CA3, and CA4/DG (hilum) (Figs 1 and 2). Differentiating between CA4 and the DG is not reliably achievable on MRI. Secondary supportive findings include increased T2 signal and architectural distortion of the normal internal hippocampal anatomy. Although these findings support the diagnosis of HS, they should not be used in isolation without considering volume loss to diagnose HS. The proposed radiologic classification based on MRI analysis is as follows:
Type 1 (classic HS): severe volume loss across all hippocampal subfields or, less commonly, severe volume loss of CA1 and the hilum with sparing of CA2/CA3.
Type 2 (CA1-predominant HS): isolated or disproportionately severe volume loss in CA1 compared with all other subfields. Mild volume loss may be present across other subfields, but the volume loss in CA1 is clearly more pronounced than in all other subfields.
Type 3 (hilar predominant HS): isolated or disproportionately severe volume loss of the hilum (CA4/DG). Mild volume loss may be present across other subfields, but the volume loss in the hilar region is definitively greater than in all other subfields.
No HS: no volume loss in any of the subfields.
Proposed radiologic HS grading
QUALITATIVE ASSESSMENT OF HS
The most vital MR image for diagnosing HS is high-resolution coronal T2 TSE.6 It has been preferred to use 2D T2 TSE sequences over 3D TSE sequences because a high in-plane resolution is necessary to adequately assess hippocampal subfields.37 It is essential to emphasize the importance of slice orientation orthogonal to the long axis of the hippocampus, high in-plane resolution (0.5 × 0.5 mm or higher), and slice thickness of ≤2 mm in coronal T2-weighted MRI of the temporal lobe. Due to these resolution requirements, higher field strength scanners offer significant improvement in assessing hippocampal subfield morphology and should be preferred for epilepsy evaluations.38 At 3T, a slice thickness of approximately 2 mm is feasible and often sufficient for evaluating the internal architecture of the hippocampus. At 7T, the slice thickness can be further reduced in the 2D TSE sequence to nearly 1 mm, with a higher in-plane resolution of approximately 0.3 × 0.3 mm. Other sequences, particularly high-resolution 3D isotropic T1-weighted sequences, are less valuable for accurately assessing subfields but can be used to support findings from the coronal T2 TSE sequence. T2 FLAIR is not suitable as a primary tool for screening the hippocampus due to its poorer SNR and contrast. Although increased FLAIR signal may be observed in the sclerotic hippocampus, it is rarely present in milder cases of HS, which limits its sensitivity. Furthermore, hippocampi are often falsely identified as abnormal on FLAIR images due to the relatively increased T2 FLAIR signal in the allocortex compared with other cortical areas, as well as artifactual signal asymmetry caused by B1+ transmit variations, which disproportionately affect the inversion pulse.
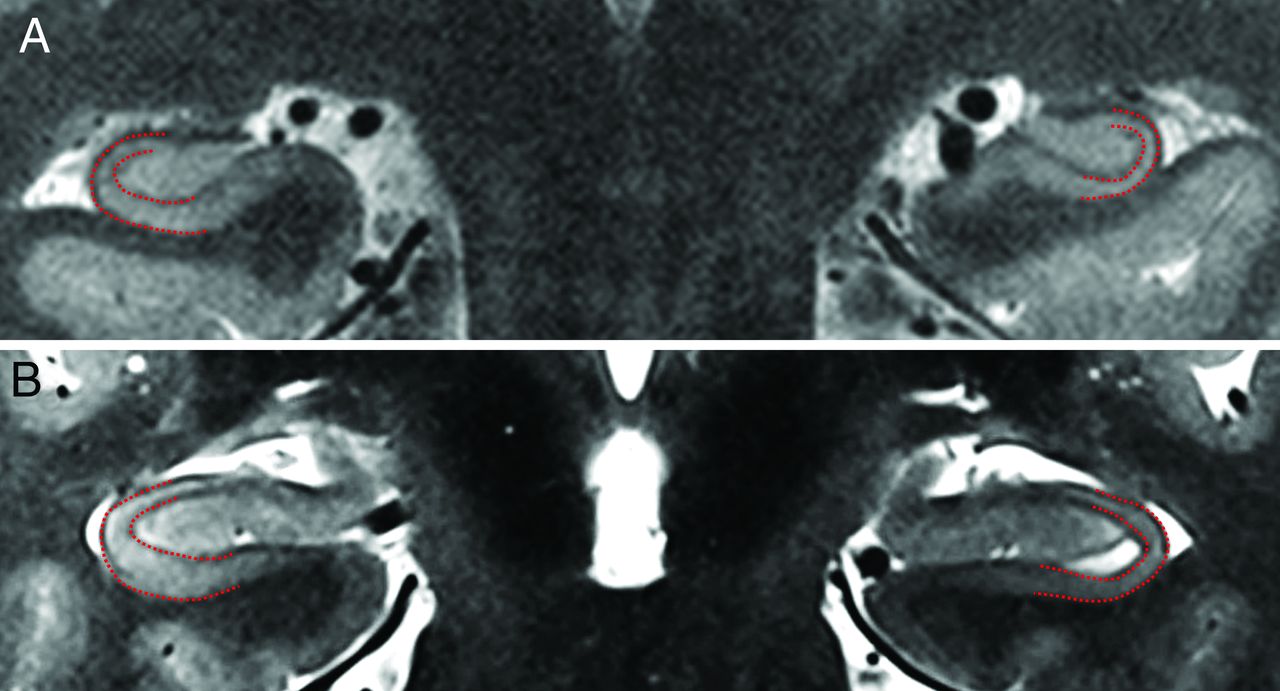
There are several practical tips for visual subfield analysis. First, recognition of the normal smooth tapering of the CA and subiculum can be a useful benchmark for the detection of subtle injury to CA1.6 When CA1 is damaged, the normal tapering is lost, resulting in a similar width between the subiculum and CA1 compared with CA2 (Fig 8). Recognition of isolated hilar volume loss is challenging. On average, the height of the normal hilum, measured from the fimbria to the base of the hilum at the SRLM (the thin hypointense stripe on T2 MRI), is approximately 4 mm.6 Evaluating symmetry between the sides may aid in assessing the CA or hilum, but it can be difficult in cases of bilateral HS or in the presence of other anatomic variations, such as incomplete hippocampal inversion. It should also be noted that the right hippocampus is typically slightly larger than the left in most normal subjects.6,39

ILAE type 2 HS with predominant CA1 cell loss and gliosis. A, Oblique coronal T2-weighted image shows the normal tapering of the right CA1 (red outline) as it extends from the subiculum toward CA2. In the left hippocampus, there is loss of this normal tapering (red outline) with a flat appearance of CA1 having similar width at its inferior junction with the subiculum and its superior junction at CA2. B, Oblique coronal T2-weighted image in another patient shows the normal tapering of CA1 (red outline) in the right hippocampus compared with the abnormal left hippocampus showing a flat appearance and loss of tapering in CA1 (red outline).
Secondary signs of HS are also commonly used to assess hippocampal volume loss. Enlargement of the temporal horn ipsilateral to the side of HS is commonly observed and is a useful finding leading to scrutiny of the ipsilateral hippocampus. However, isolated dilation of the temporal horn can occur in the absence of HS and should not be relied upon as the sole diagnostic criterion. Furthermore, subtle changes in subfield volumes, such as those in types 2 and 3, may not result in visually noticeable overall hippocampal volume loss.5 This highlights the importance of assessing the subfields to accurately evaluate hippocampal pathology.
Other reported signs of HS, such as increased T2/FLAIR signal and architectural distortion, can provide valuable evidence for the confirmation of HS. However, it is important not to rely solely on these signs for the diagnosis of HS. These signs can also be observed in various other pathologies affecting the hippocampus, including postictal changes or autoimmune epilepsy, particularly when T2/FLAIR hyperintensity is not associated with hippocampal volume loss. Architectural distortion refers to the “blurring” of the internal architecture of the hippocampus, which in practice refers to the nonvisualization of SRLM separating the bright bands of the CA from the hilum. The limited spatial resolution of the T2 TSE coronal sequence often leads to this “blurring” phenomenon due to partial volume averaging of the SRLM from hippocampal undulations on 3T MRI (“hippocampal dentation”). Cases of architectural blurring at 1.5T or 3T are often found to be normal when reevaluated at 7T. To invoke architectural distortion on a 3T MRI, the “blurring” should be observed on multiple contiguous T2 coronal slices rather than just a single slice.
QUANTITATIVE ASSESSMENT OF HS
Most quantitative studies on HS have primarily focused on measuring hippocampal volumes by using automated or manual techniques. Despite the abundance of studies, the results have been highly variable. One of the main reasons for this variability may be the lack of standardization, as different studies have used diverse study populations, imaging sequences, magnetic field strengths, and segmentation algorithms. For instance, when using the same commercially available segmentation tool, Azab et al40 found that automated hippocampal volume measurements were marginally more accurate than those made by expert readers (79.4% versus 72.6%) by using a combination of 1.5T and 3T MRI. In contrast, by using the same tool, Louis et al3 found that the expert reader had significantly higher accuracy compared with automated segmentation (93.4% versus 69.9%) exclusively by using 3T MRI. These differences suggest that superior MRI quality may enhance reader performance, possibly due to improved ability to discern more subtle morphologic and subfield alterations.
Volumetric tools that solely rely on measuring whole hippocampal volumes have inherent limitations due to the pathologic mechanism of HS in epilepsy. While “classic” type 1 HS might be expected to be more readily identified by using whole hippocampal volumes due to the overall extent of damage, types 2 and 3 may be more challenging. For example, the CA4-DG complex accounts for approximately one-fifth of the total hippocampal volume,41 which means that many cases of type 3 HS may be underestimated when using whole hippocampal volumes. Indeed, studies have shown that the histologic volumes of CA1, CA4, and DG did not correlate with MRI measurements of whole hippocampal volume,5 highlighting the diagnostic limitations of relying solely on whole hippocampal volumes for detecting type 2 and type 3 HS.
As MRI techniques have advanced, there has been growing interest in the segmentation and volumetrics of hippocampal subfields. Some studies have shown promising results by using automated subfield segmentation42 for the lateralization of TLE. However, other studies have found that the volumes of CA1 and CA4 from histopathology did not correlate with the respective subfield volumetrics obtained from MRI by using standard field strength MRI.5 Ultra-highfield MRI shows promise for hippocampal volumetrics due to its ability to provide high-resolution imaging of the hippocampus through enhanced SNR.43 Nonetheless, studies have yielded conflicting results with automated subfield measurements at 7T that either do not align with known pathophysiology or do not match histologic findings.41
In summary, whole hippocampal volumetrics have inherent limitations in detecting subtle HS, particularly type 2 and 3 HS. Many studies examining whole hippocampal volumes suffer from selection bias, as patients who proceed to surgery are more likely to exhibit more obvious imaging changes. Others44 that rely on “consensus” clinical diagnosis without pathologic validation are also likely biased, as imaging likely played a significant role in the determination of TLE in these cohorts, resulting in the inclusion of more patients with evident imaging abnormalities. Although subfield volumetrics show potential in improving detection rates and facilitating automated HS subtype classification, the effectiveness of these techniques depends on high-resolution MRI, which may not be widely accessible. Currently, quantitative hippocampal imaging has not demonstrated a definitive advantage over expert readers in everyday clinical applications, emphasizing the need for additional research to refine and validate these methods.
DISCUSSION
HS is the most common pathology in patients with TLE. Although HS is commonly considered a binary assessment in radiologic evaluation, it is well-known that the histopathologic changes occur in distinct clusters.4,7 As discussed, studies have demonstrated that these histopathologic changes have significant clinical implications for patient management, prognosis, and surgical considerations.16⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓-32 Therefore, early and accurate characterization of HS types through in vivo imaging is crucial. Recent advancements in MRI technology have enabled the detection of many of these changes with increasing accuracy. Therefore, we propose a radiologic classification scheme that aligns with the ILAE pathology classification, aiming to improve clinical communication, decision-making, and serve as a foundation for future developments in MRI technology and quantitative neuroimaging for patients with TLE.
The precise pathogenesis of HS is still not fully understood; however, the age at which the initial precipitating event occurs is an essential factor, with a younger age of the initial event corresponding to more severe forms of HS. Meanwhile, a later age of onset is less frequently associated with HS. Other demographic factors such as seizure frequency, number of lifetime seizures, sex, and age at surgery have not consistently been linked to HS subtypes. After temporal lobe resection, patients with type 1 HS are more likely to achieve seizure freedom and experience lower rates of verbal memory decline.4,17,26 Furthermore, type 1 HS is associated with better outcomes from less invasive surgical treatments, such as laser interstitial thermal therapy.32 The implications of HS on neuromodulation approaches, such as deep brain stimulation and responsive neurostimulation, are currently not well understood.35,36 These factors underscore the importance of distinguishing HS subtypes on MRI to assess specific treatment outcomes and guide future decision-making.
With recent advancements in MRI technology, it is now possible to characterize hippocampal substructure more accurately. Routine 3T MRI, specifically T2 coronal TSE sequences, can be optimized to confidently evaluate subtle changes within the subfields of the hippocampus. The use of 7T MRI, which is becoming increasingly common in the assessment of patients with epilepsy, allows for even more precise assessment of these changes. The aim of this study is to present a comprehensive framework for systematically assessing hippocampal injury, particularly as it applies to the radiologic classification of HS subtypes. However, it is important to acknowledge that distinguishing between these subtypes can be challenging in certain cases, as even histology does not achieve perfect interobserver agreement. After multiple iterations aimed at improving accuracy, the mean overall κ value for subtype classification on histology was found to be 0.75, with the highest agreement observed for cases with no HS (mean κ = 0.91). Based on the available data, it may be more clinically significant to differentiate type 1 HS from types 2 and 3. Furthermore, it is crucial to recognize the often-overlooked clinical observation of distinguishing between a normal hippocampus and HS types 2 and 3, where there may be more subtle overall hippocampal volume change. Ideally, the proposed framework will benefit clinical evaluations, as well as serve as a guide to development of new automated tools to aid in diagnosis of HS subtypes beyond solely volumetric measurements. Last, future studies will be needed to assess the clinical performance of this model versus histologic findings.
CONCLUSIONS
HS is a prevalent structural anomaly observed in individuals diagnosed with TLE. This condition holds significant implications for clinical presentation, prognosis, and treatment planning. Although classic HS (type 1) has been widely acknowledged and identified in radiology, other subtypes have received less recognition and characterization. To address this gap, the advancement of MRI technology has rendered it possible to better assess the morphology of hippocampal subfields in vivo. Consequently, this necessitates the adoption of a descriptive framework that aligns with histopathologic classifications. In light of this, we propose the utilization of an MR HS classification template that effectively harmonizes radiologic findings with the ILAE HS histopathologic categories. Such classification is necessary as a framework for future studies examining the relationship of MRI findings in TLE diagnosis and outcomes.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received January 17, 2024.
- Accepted after revision February 14, 2024.
- © 2024 by American Journal of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- SUMMARY:
- ABBREVIATIONS:
- OVERVIEW OF HIPPOCAMPAL ANATOMY
- PATHOPHYSIOLOGY OF HS IN EPILEPSY
- ILAE CLASSIFICATION OF HS IN EPILEPSY
- CLINICAL IMPLICATIONS OF THE ILAE CLASSIFICATION OF HS
- PROPOSED RADIOLOGIC TYPES CORRELATING WITH ILAE PATHOLOGY CLASSIFICATION
- QUALITATIVE ASSESSMENT OF HS
- QUANTITATIVE ASSESSMENT OF HS
- DISCUSSION
- CONCLUSIONS
- Footnotes
- References
- Figures & Data
- Supplemental
- Info & Metrics
- Responses
- References
Related Articles
Cited By...
- No citing articles found.