
Abstract
SUMMARY: Laryngectomy and pharyngectomy are surgical options for advanced laryngeal or pharyngeal squamous cell carcinoma. Cervical osteomyelitis-diskitis, occurring when there is dehiscence of the posterior neopharyngeal wall, is an uncommon complication of laryngopharyngectomy. This case series describes imaging findings of pharyngoesophageal wall breakdown with subsequent cervical spine infection and demonstrates that most of these patients had undergone prior esophageal or neopharyngeal dilations for benign posttreatment stricture. Neck pain, fever, or serologic evidence of infection should prompt careful evaluation for osteomyelitis-diskitis and assessment for neopharyngeal breakdown and sinus tract formation, especially in the postdilation setting.
ABBREVIATION:
- SCCA
- squamous cell carcinoma
Treatment of advanced or recurrent head and neck cancer usually involves multiple modalities, including surgical resection, radiation therapy, and/or chemotherapy. For advanced laryngeal and pharyngeal squamous cell carcinoma (SCCA), the surgical options are generally laryngectomy or pharyngectomy, which create defects that are managed by primary closure or flap reconstruction.1 In addition to defect closure, a neopharynx is constructed to restore swallowing. A cutaneous fistula between the neopharynx and skin is a complication that is readily recognized by clinical examination of the treated neck. Neopharyngeal or pharyngoesophageal ulceration and anastomotic breakdown of the posterior wall, with subsequent sinus tract formation, are, however, uncommon and underrecognized complications.2 Risk factors for perforation are those resulting in poor soft-tissue healing, including prior chemo-/radiation therapy, poor nutritional status, and continued tobacco and alcohol use.3,4 Ulceration and perforation most commonly occur on the posterior neopharyngeal wall.5 Such perforations or microperforations establish conditions under which cervical osteomyelitis and diskitis can result.
The purpose of this retrospective, multisite clinical series is to describe 11 patients who developed osteomyelitis-diskitis following laryngopharyngectomy for tumor resection, pharyngeal reconstruction, and adjuvant radiation.6
Case Series
Institutional review board approval from each institution (Mayo Clinic Jacksonville, Emory University, University of Kentucky) was obtained. A total of 11 patients comprised the study population. Seven of 11 patients were identified at the time of imaging performed for “neck pain” or possible infection. Additional cases were identified retrospectively; databases were searched for “laryngectomy,” “pharyngectomy,” “diskitis” or “osteomyelitis.” Electronic medical records were reviewed to confirm cervical osteomyelitis-diskitis after laryngectomy or pharyngectomy. Imaging was reviewed by group consensus.
There were 9 male and 2 female patients (age range, 60–78 years, with an average age of 65.5 years). All patients had undergone surgical resection for SCCA of the larynx (10/11) or hypopharynx (1/11). All were also treated with adjuvant radiation. All patients had flap reconstruction after laryngopharyngectomy, either as the initial surgery or after recurrent tumor. The average time between initial treatment and the diagnosis of osteomyelitis-diskitis was 7 years; range, 3–12 years. Patients presented years after the operation with new pathologic compression fractures, neck pain, or arm pain. All had serologic evidence (elevated white blood cell count, C-reactive protein, and/or erythrocyte sedimentation rate) of infection. The time between symptom onset and diagnosis was not available for all, but the delay in diagnosis was as long as 18 months.
A barium swallow in our series was used when patients had new or worsening dysphagia to evaluate stenosis or aspiration; only 1 examination showed a leak. Nine patients had ≥1 posttreatment esophageal or neopharyngeal stricture dilation for dysphagia, obstruction, and an inability to take oral nutrition. Two had no history available regarding dilation. The onset of symptoms after dilation was not immediate and ranged from several weeks to months.
Cross-sectional imaging was performed for routine surveillance or because of neck pain, dysphagia, or concern for infection. Both CT and MR imaging were performed in 9 patients; CT only in 1 patient; and MR imaging only in 1 patient. Both CT and MR imaging showed edema and phlegmonous changes around the neopharynx. An incomplete air column from the oropharynx to the cervical esophagus was present in all cases. Extraluminal air was frequently misinterpreted as neopharyngeal air. Extraluminal air was either a relatively large, isolated pocket of air or small bubbles around the reconstruction (Fig 1) and was seen in 4 of 11 patients. A defect in the posterior neopharynx with a fluid- and/or air-filled fistulous tract extending to the cervical spine was visible in 10 of 11 patients (Figs 2 and 3A). Multiplanar reformations performed at the workstation in oblique planes facilitated recognizing that air or gas was not in the lumen and the presence of a fistulous tract.

A 51-year-old man with a history of laryngeal SCCA, treated with total laryngectomy and myocutaneous flap reconstruction. Sagittal contrast-enhanced CT demonstrates marked prevertebral soft-tissue thickening from C4 to T1 and chronic fracture/dislocation at C6–C7. A bulky myocutaneous flap reconstructs the anterior pharyngeal wall; note how lumen tapers, terminating at C7. A tiny locule of extraluminal air is present in the prevertebral soft tissues just anterior to the T1 superior endplate (arrow).

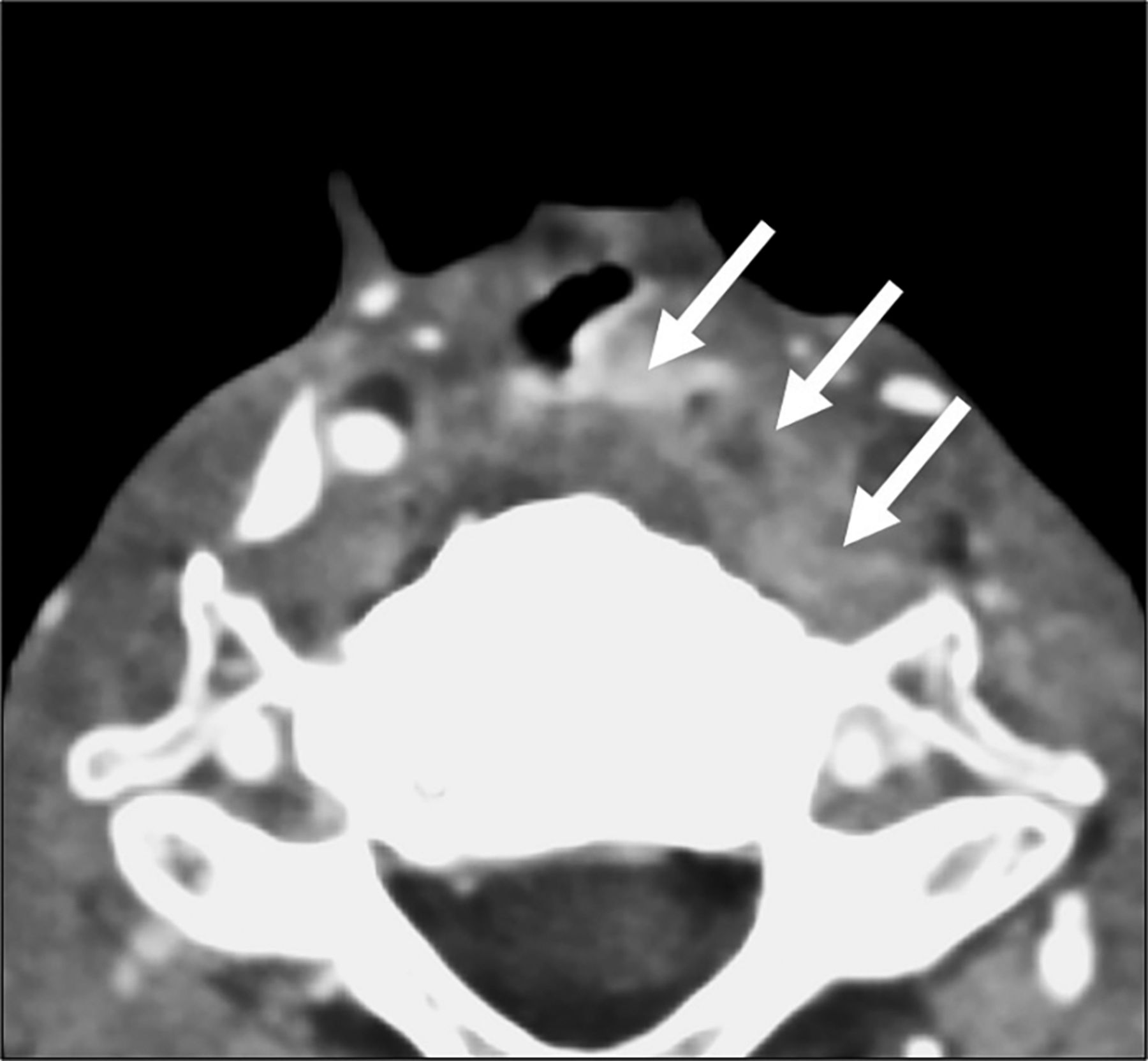
A 67-year-old man with a history of laryngeal SCCA, status post laryngectomy and radiation, and dilation of multiple sites of neopharyngeal and esophageal stenosis presented with obstruction and severe neck pain. An axial contrast-enhanced image demonstrates a fluid-filled sinus tract from the neopharyngeal posterior wall, extending to thickened prevertebral soft tissues (arrows). MR imaging of the cervical spine revealed characteristic cervical diskitis/osteomyelitis at multiple levels (not shown).
Characteristic CT and MR imaging findings of osteomyelitis and diskitis were present in all cases (Fig 3B). Diskitis was at C5–6 in 4/11, C6–7 in 2/11, and 1 each at C2–3, C3–4, and C4–5. Two patients had multilevel diskitis from C4 to C7.

A 74-year-old woman with a history of laryngeal carcinoma, status post total laryngectomy and radiation, and recent esophageal dilation presented with neck pain and fever. A, An axial postcontrast CT image demonstrates a sinus tract extending to the vertebral body (arrows). B, Sagittal T1 postcontrast fat-saturated MR image demonstrates thickening of the prevertebral soft tissue with a focal defect (arrow) and enhancement of the C5 and C6 vertebral bodies (arrowheads) and loss of disk height with enhancement, consistent with diskitis/osteomyelitis.
DISCUSSION
Dysphagia reportedly occurs in up to 70%–75% of patients in the posttreatment setting of head and neck cancer with a negative impact on the quality of life.7 Neopharyngeal or esophagopharyngeal strictures are common causes of dysphagia. In this patient population, strictures may be due to recurrent tumor, but, more commonly, are benign.8,9 Multimodality treatment—surgery, radiation, and chemotherapy—increases the risk of pharyngeal or neopharyngeal benign strictures, reportedly occurring as frequently as 33% of the time.8
After chemoradiation, soft-tissue chronic inflammation causes collagen deposition and fibrin production, resulting in fibrosis and stricture. Patients may undergo endoscopy with dilation to relieve such strictures. Endoscopic dilation of a neopharyngeal or pharyngoesophageal stricture is a safe and effective treatment for stricture-related dysphagia. Complications of this procedure include bleeding and perforation.9 In this setting, infectious organisms can gain access to the vertebral bodies by either perforation or microtrauma.5
In patients who have not undergone laryngopharyngectomy, perforation in the cervical region most commonly occurs at the triangular area in the posterior wall of the pharynx between the transverse and oblique bundles of the inferior pharyngeal constrictor muscles, termed the Killian triangle.4 This area is adjacent to the C4–C6 vertebral bodies, separated by only a thin layer of fascia. In patients undergoing laryngectomy or pharyngectomy, the Killian triangle does not exist and is replaced by a neopharyngeal anastomosis, an anatomic site of weakness but also, commonly, the site of stricture.8
All patients in this series had flap reconstruction of the defect, either as part of the initial treatment or after failure and tumor recurrence. Flap failure is a serious complication for the patient with treated head and neck malignancy. MR imaging or CT perfusion may help predict free flap failure from vascular compromise.10 Evaluation for stricture and possible leak following dilation may be diagnosed by fluoroscopic barium swallow examination.11 Our series showed esophageal or neopharyngeal stenosis, and subsequent dilation should prompt attention to the cervical spine, looking for infection if a patient presents with neck pain. In the absence of cord compromise or spine instability, surgical management of diskitis/osteomyelitis with debridement and spine stabilization and repair of the neopharyngeal defect should be considered after failure of medical therapy.12
In conclusion, diskitis/osteomyelitis should be a consideration in a patient previously treated for laryngeal or hypopharyngeal carcinoma who presents with neck pain or signs of infection, especially if imaging reveals posterior neopharyngeal breakdown and sinus tract formation. While CT is often the first imaging performed in this setting, MR imaging of the cervical spine is more sensitive for spine infection. In our series, most patients with neopharyngeal perforation and spinal infection had undergone prior esophageal or neopharyngeal dilations for benign posttreatment stricture.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received August 9, 2023.
- Accepted after revision September 27, 2023.
- © 2023 by American Journal of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.