
Abstract
BACKGROUND AND PURPOSE: Surgical clipping and endovascular treatment are commonly used in patients with unruptured intracranial aneurysms. We compared the safety and efficacy of the 2 treatments in a randomized trial.
MATERIALS AND METHODS: Clipping or endovascular treatments were randomly allocated to patients with one or more 3- to 25-mm unruptured intracranial aneurysms judged treatable both ways by participating physicians. The study hypothesized that clipping would decrease the incidence of treatment failure from 13% to 4%, a composite primary outcome defined as failure of aneurysm occlusion, intracranial hemorrhage during follow-up, or residual aneurysms at 1 year, as adjudicated by a core lab. Safety outcomes included new neurologic deficits following treatment, hospitalization of >5 days, and overall morbidity and mortality (mRS > 2) at 1 year. There was no blinding.
RESULTS: Two hundred ninety-one patients were enrolled from 2010 to 2020 in 7 centers. The 1-year primary outcome, ascertainable in 290/291 (99%) patients, was reached in 13/142 (9%; 95% CI, 5%–15%) patients allocated to surgery and in 28/148 (19%; 95% CI, 13%–26%) patients allocated to endovascular treatments (relative risk: 2.07; 95% CI, 1.12–3.83; P = .021). Morbidity and mortality (mRS >2) at 1 year occurred in 3/143 and 3/148 (2%; 95% CI, 1%–6%) patients allocated to surgery and endovascular treatments, respectively. Neurologic deficits (32/143, 22%; 95% CI, 16%–30% versus 19/148, 12%; 95% CI, 8%–19%; relative risk: 1.74; 95% CI, 1.04–2.92; P = .04) and hospitalizations beyond 5 days (69/143, 48%; 95% CI, 40%–56% versus 12/148, 8%; 95% CI, 5%–14%; relative risk: 0.18; 95% CI, 0.11–0.31; P < .001) were more frequent after surgery.
CONCLUSIONS: Surgical clipping is more effective than endovascular treatment of unruptured intracranial aneurysms in terms of the frequency of the primary outcome of treatment failure. Results were mainly driven by angiographic results at 1 year.
ABBREVIATIONS:
- EVT
- endovascular treatment
- RR
- relative risk
- UIA
- unruptured intracranial aneurysm
Unruptured intracranial aneurysms (UIAs) are increasingly discovered as incidental imaging findings, with an estimated prevalence of 2%–5% of the adult population, but most remain asymptomatic.1⇓-3 Ruptures are infrequent, on the order of 1% per year.4⇓-6 The best management of patients with UIAs is uncertain, with significant variability and disagreement among clinicians.7 Despite the lack of level 1 evidence of benefit, preventive endovascular or surgical treatments are commonly used.6 Endovascular treatment (EVT) has progressively supplanted surgical clipping after coiling was shown to be superior for ruptured aneurysms in 2002.8 However, for unruptured aneurysms, the safety and efficacy of the 2 treatments have never been previously compared in a randomized trial.9
It remains unclear whether UIAs should be repaired, and if so, which treatment is best. A proper answer to these questions would require nearly a thousand patients to be followed for many years, using a hard clinical outcome such as disabling stroke or death as a primary end point. An attempt to address the question of whether UIAs should be treated was interrupted in 2009 due to insufficient recruitment.10 Surgical clipping, though more invasive, is reputed to be more effective than endovascular treatment, but this possibility has never been proved.11 The Collaborative UnRuptured Endovascular versus Surgery (CURES) trial was designed to test the hypothesis that surgical clipping of intradural, saccular UIAs was superior to endovascular management in decreasing the proportion of patients experiencing treatment failure, a composite primary outcome defined as failure of the allocated treatment technique to occlude the aneurysm, aneurysmal rupture during follow-up, or a residual aneurysm on angiography at 1 year, decreasing from 14% to 3%.12 We here report the final results of the CURES trial.
MATERIALS AND METHODS
This report follows the CONsolidated Standards Of Reporting Trials (CONSORT) guidelines. CURES was an investigator-led, pragmatic, multicenter, randomized (1:1) parallel-group trial conducted in 5 Canadian and 2 European centers (Montreal, Edmonton, Ottawa, Trois-Rivières, and Calgary in Canada; and Liège, Belgium, and Lille, France). The trial, conceived as a pilot before a larger pivotal effort, was initially funded by the Canadian Institutes of Health Research (MOP 119554). The protocol, published in 2011,12 was approved by the local institutional review boards of all participating centers, and all patients provided written informed consent. Data capture and management were through secure servers in compliance with Good Clinical Practice requirements. The trial was monitored in Montreal, Canada. Electronic case report forms were simple, and data collection was kept to a minimum to facilitate completion by ordinary care personnel. Neuropsychological tests were not required by protocol. There were no preplanned interim efficacy analyses or stopping rules for safety or futility because both treatments were in common clinical use. The number of patients to be recruited was estimated to be 118 per group (with a statistical power of 0.80 and a 2-sided α of .05), or 260 patients (to account for losses and cross-overs). The trial was launched in September 2010, but participation was below expectations. The Steering Committee decided to publish interim results in 2016 to encourage center participation and before re-submission for financial support.13 Further funding was declined in 2016, but the Steering Committee opted for trial continuation until the initiation of the Comprehensive Aneurysm Management (CAM) study on UIAs in 2020.14 The last patient was recruited in May 2020. In May 2021, after examination of the blinded 1-year outcome data, the Data Safety Monitoring Committee recommended trial continuation, but the Steering Committee decided to report the CURES trial.
Patients
CURES was designed to address the question of the best treatment for patients with UIAs eligible for both surgical or endovascular options. Patients were recruited from outpatient neurosurgery or neuroradiology clinics by participating physicians at each study site, which all offer specialized neurovascular care. Independent (mRS of <3) patients 18 years of age and older with any intradural, saccular, nonbasilar UIA, 3–25 mm (in maximal cross-sectional diameter), were offered participation if they had at least 10 years of life expectancy. Patients were excluded if their aneurysms were thought to require endovascular flow diversion or parent vessel occlusion, with or without surgical bypass. Patients with multiple aneurysms were not excluded, but 1 index aneurysm was to be chosen as the main target. The protocol was modified on October 22, 2014, to include patients with recurrent but previously treated aneurysms (n = 10); on May 9, 2016, to allow prerandomization when approved by the local institutional review board;15 and on June 25, 2019, to include patients considered for endovascular flow diversion (n = 9). A prospective screening log of potential participants was not required.
Interventions
Patients were treated with surgical clipping or endovascular methods as per local practices, with technical details left to the individual operators.
Outcome Measures
The composite primary outcome measure, “treatment failure,” occurred under the following circumstances: 1) failure of aneurysm occlusion using the allocated treatment technique, 2) intracranial hemorrhage during follow-up, or 3) when a residual or recurrent index aneurysm was found using CTA, MRA, or conventional angiography at 1 year. Cross-overs to the other treatment arm, with no attempt to occlude the aneurysm, were not considered treatment failures. Additional procedures directed against the index aneurysm performed during the follow-up period were considered treatment failures. One primary poor efficacy outcome was allocated per patient; when a patient reached >1 outcome, the following hierarchical order was used to classify each patient: intracranial hemorrhage during follow-up > initial treatment failure > residual aneurysm at 12-month imaging follow-up.
Secondary end points included the individual components of the composite primary outcome, as well as treatment safety outcomes: overall morbidity (mRS > 2) and mortality at 1 year, new perioperative (30 days) neurologic deficits (defined as any new weakness, sensory abnormality, decreased level of consciousness, or cranial nerve deficit), perioperative morbidity (mRS >2) measured at discharge, peritreatment hospitalization lasting >5 days, and discharge to a location other than home.
Follow-up tests and visits were standard per local practices, including neurologic examinations, brain imaging studies, and a functional assessment according to the mRS at discharge, 6 weeks, and 1 year using a standardized questionnaire.16
A vascular imaging study (conventional angiography, CTA, or MRA) at a mean of 12 (± 2) months to verify aneurysm occlusion was expected as standard care, to be centrally adjudicated by an independent core lab according to a previously validated classification system.17,18 The protocol did not impose a common follow-up imaging technique to be used in all patients because surgical patients are typically followed by CTA, while patients undergoing EVT are followed by MRA. Blinding of the core lab assessors for the presence of surgical clips or endovascular devices was not possible.
Randomization
Parallel-group randomization (1:1) was concealed, generated through a web-based platform (https://www.medscinet.com/cures), and minimized for age older than 60 years, aneurysm size of ≥15 mm, and posterior circulation location (posterior communicating artery aneurysms were considered to be in the anterior circulation). Blinding to treatment assignment of patients, physicians, and outcome assessors was not done.
Statistical Analyses
All data were analyzed by statisticians (J.Z., M.C.). Patient and aneurysm characteristics and primary and secondary outcomes are described by group using mean and SD for continuous variables and percentages for categoric variables. Analyses were intent-to-treat, but as-treated analyses were also performed. The impact of missing data on the primary outcome results was studied using a worst-case-scenario sensitivity analysis, in which the missing data (n = 1) were replaced by a bad outcome. Relative risk (RR) was estimated using a generalized estimating equation with a binomial distribution and a log-link function reporting 95% confidence intervals. No adjustments for residual confounding factors were made. The analyses of interactions between prespecified subgroups of interest and treatment were made by adding subgroup variables and interaction in the generalized estimating equation models. Subgroups predefined according to minimization criteria (age, aneurysm size, and location) were examined, regardless of the results of tests for interactions. There were no corrections for multiplicity of analyses. Analyses were performed using SAS software, Version 9.4 (SAS Institute) and SPSS, Version 26 (IBM) with a significance level of 5%.
Roles of the Funding Source and Data Integrity
Neither the funding agency (Canadian Institutes of Health Research) nor the sponsor (Université de Montréal) had any part in the study design, data collection, analysis, or reporting and had no access to the data or source documents.
RESULTS
From September 2010 to May 2020, two hundred ninety-one patients with 376 UIAs (291 index aneurysms and 85 additional aneurysms) were recruited. Patients who registered and had treatment randomly allocated are presented in the flow chart (Fig 1). Baseline patient and aneurysm characteristics were similar (Table 1). Of 291 patients, 138/143 patients randomly allocated to surgery underwent clipping; 5 were treated with EVT. Of the 148 patients randomly allocated EVT, 142 underwent EVT and 6 were treated by surgery.

Study flowchart.
Patient and index aneurysm characteristics
The 1-year primary outcome data are available for 290/291 patients (99%; Table 2): 13/142 patients (9%; 95% CI, 5%–15%) in the surgical group and 28/148 (19%; 95% CI, 13%–26%) in the EVT group reached the primary outcome (RR: 2.07; 95% CI, 1.12–3.83; P = .021). No primary outcomes occurred in patients who crossed over, and the as-treated analysis of the primary end point gave similar results (RR: 2.10; 95% CI, 1.13–3.88; P = .019). A worst-case-scenario analysis in which a poor outcome was imputed for the 1 missing surgical primary outcome did not significantly change the results. In the endovascular group, the “treatment failure” primary outcome was assigned because of immediate failure in 5 patients, a fatal treatment-related subarachnoid hemorrhage in 1, and saccular aneurysmal recurrences at 1 year in 22 patients (2 retreated by EVT; 6, by clipping; or 14 left untreated). In the surgical group, treatment failure was assigned as follows: 1 patient who awoke hemiparetic from the operation and was immediately returned to the operating room for clip removal, 1 surgical patient who died from aneurysmal rupture the day before scheduled treatment, 1 patient who died 2.5 years after treatment due to rupture of a contralateral coiled aneurysm (the clipped aneurysm remained occluded), and 10 patients who had residual saccular aneurysms at 1 year. These recurrences were treated with stent-assisted coiling (n = 3) or left untreated at the time of reporting (n = 7).
Primary and secondary outcomes
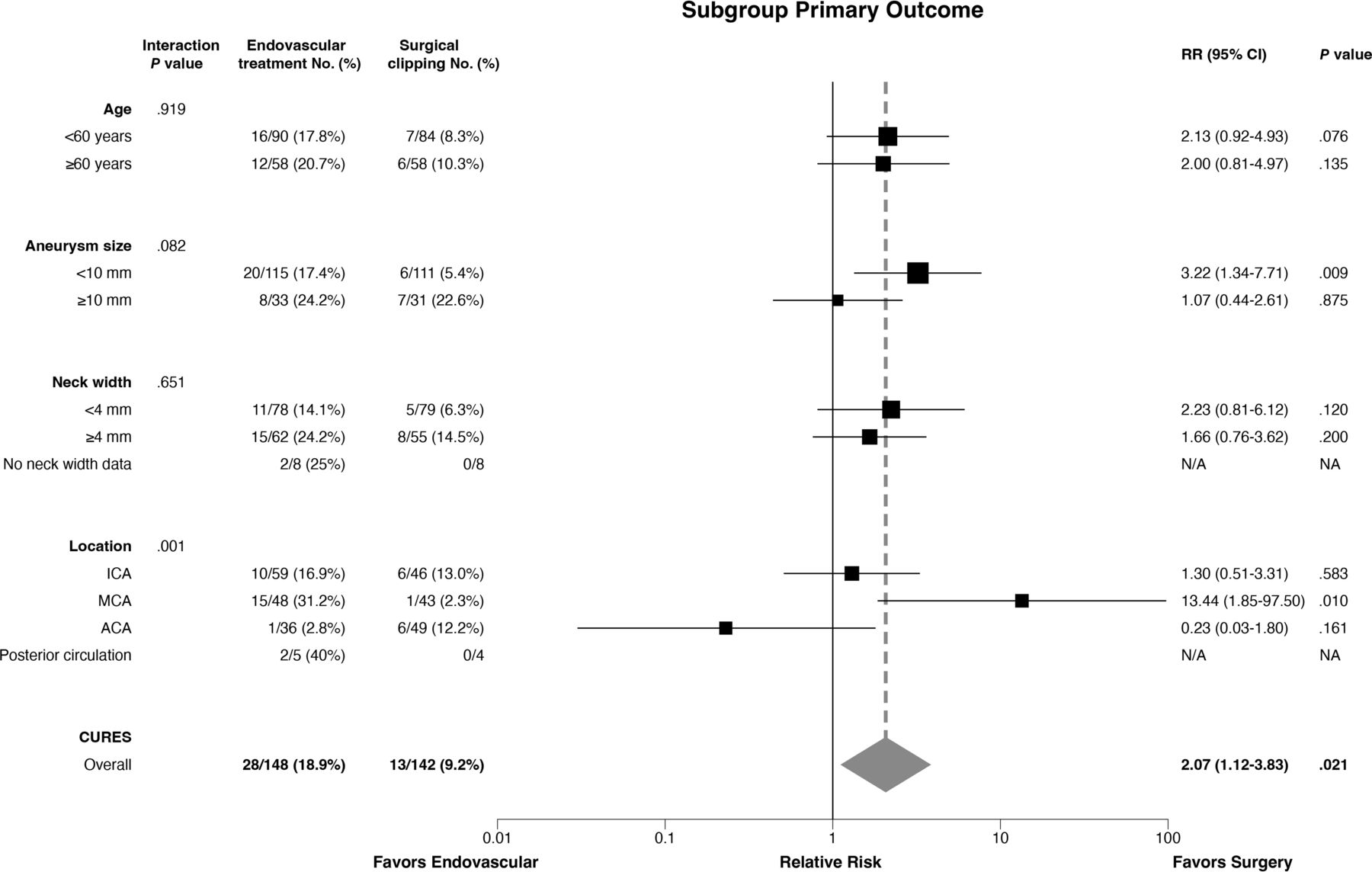
Intent-to-treat exploratory subgroup analyses are detailed and illustrated in the forest plot (Fig 2). The interaction test was not significant for age, size, or neck width. There was a significant interaction with location (P = .001), with treatment failures more frequent in patients with MCA aneurysms in the EVT group (RR: 13.44; 95% CI, 1.85–97.5).

Subgroup analyses of primary outcome. NA indicates not applicable.
Secondary outcomes, including the individual components of the primary outcome and safety outcomes, as well as pretreatment, discharge, and 1-year follow-up mRS scores are presented in Table 2 and Fig 3. Perioperative safety outcomes were in favor of EVT: New neurologic deficits occurred in 32/143 surgical patients (22%; 95% CI, 16%–30%) compared with 19/148 (12%; 95% CI, 8%–19%) patients allocated to EVT (P = .04). Hospitalization for > 5 days occurred in 69/143 (48%; 95% CI, 40%–56%) surgical patients, compared with 12/148 (8%; 95% CI, 5%–14%) patients treated endovascularly (RR: 0.18; 95% CI, 0.11–0.31; P < .001). Perioperative safety outcomes, such as death or dependency at discharge or discharge to a location other than home, were similar. Patients with a discharge mRS of 0 were more frequent in the endovascular group (Fig 3). All 291 patients had clinical follow-up data: By 1 year, 1 surgical patient had died and 2 were disabled (mRS >2), 1 patient allocated to EVT had died, and 2 were disabled.

Clinical status at baseline, hospital discharge, and 1-year follow-up.
Serious adverse events occurred in 31/143 (22%; 95% CI, 16%–29%) surgical patients and 15/148 (10%; 95% CI, 6%–16%) patients treated endovascularly (P = .01) (details in the Online Supplemental Data). One-year follow-up imaging is available for 288 patients: Complete occlusions were more frequent in patients allocated to surgical management, while saccular aneurysms and residual necks were more frequent in patients allocated to EVT (Table 2).
DISCUSSION
CURES provides randomized evidence that clipping is more effective than EVT in terms of angiographic results at 1 year. This benefit comes at the cost of a more invasive intervention, associated with a longer hospitalization and a greater risk of posttreatment neurologic deficits. However, death and dependency at discharge and 1 year were similarly infrequent in both groups.
The primary end point of the trial was a composite that attempted to capture in 1 judgment the efficacy of treatment. This outcome combined immediate results (failure of the allocated treatment technique) and aneurysm rupture during follow-up and, to account for the short follow-up, an angiographic outcome of “residual aneurysm” at 1 year. Angiographic outcomes are necessary in practice because clinicians cannot wait until aneurysms rupture to judge the results of each procedure.19 Angiography is the most common primary outcome of aneurysm trials.18,20⇓⇓-23 Residual aneurysm was used to judge treatment failure because this angiographic category has been shown to be reliable and its clinical significance has been constant across raters, imaging modalities, and treatments.17,18 This reliability is important because different angiographic imaging modalities are routinely used to follow surgically clipped (mostly CTA) versus endovascularly treated aneurysms (mostly MRA). Had we used “complete occlusion” as the angiographic measure of efficacy, the conclusion would not have been different.
The 1-year timeframe was selected to be long enough for patients to recover from transient morbidity and to allow postcoiling aneurysm recurrences to occur.24,25
The clinical significance of angiographic recurrences in terms of aneurysm rupture is unclear, but recurrences are potentially concerning. There were no posttreatment ruptures of index aneurysms during the course of this study. Case series and meta-analyses have reported hemorrhages after endovascular coiling in <1% of patients, but retreatments were performed in 10%–22% of patients.26,27 The better angiographic outcomes of surgery may translate into clinical benefits if, with time, delayed recurrent aneurysms rupture or if there are complications from retreatment of recurrent aneurysms.
CURES was fully integrated into clinical practice, with no extra risks, tests, or costs, and data were collected by ordinary care personnel at the time of routine follow-up visits.28 The main drawback of the approach is the lack of blinding. To decrease the risk of bias, we used death or dependency (mRS > 2) as the clinical outcome at 1 year, a choice that has been shown to be reliable.29
Subgroup exploratory findings suggest that surgery is particularly more effective than EVT in MCA aneurysms. A trial dedicated to MCA aneurysms has recently been proposed.30
The use of surgical clipping for aneurysms is declining, and concerns have been raised that this trend may lead to a decrease in open surgical expertise.31⇓-33 The surgical angiographic results presented here are promising, but they come with added initial morbidity. It would be ill-advised to prematurely abandon a treatment that could provide better long-term clinical outcomes, but this remains to be shown. Whether patients with UIAs should be treated at all also remains a dilemma. These questions are now being addressed by the CAM study.14,34
The limitations to this study include the relatively small number of patients, slowly accrued during >10 years. Indications, techniques, and treatments may have substantially changed across time. In particular, relatively few patients were treated with newer stents, flow diverters, or intrasaccular flow disruptors. The noninvasive imaging technique most commonly used to assess angiographic results at 1 year differed between groups. There were a few patients with posterior circulation aneurysms to whom the results of this trial may not apply. Other limitations are the absence of blinding of outcome assessors and the lack of adjustment for a multiplicity of analyses. The follow-up period may have been insufficient to capture all recurrences that can occur after 1 year, and it was too short to assess efficacy in the prevention of long-term aneurysm rupture.26
Only 7 centers actively participated. Despite the limitations, results are expected to apply to a variety of patients, operators, and settings.
CONCLUSIONS
Surgical clipping is more effective than endovascular treatment of UIAs in terms of the frequency of the primary outcome measure, treatment failure. Results were mainly driven by angiographic results at 1 year. Additional trials are required to assess long-term clinical outcome results of the preventive treatment of UIAs.
Acknowledgment
We thank Dr Bryce Weir for his contributions to an early version of this manuscript.
Footnotes
This work was funded by Canadian Institutes of Health Research (MOP119554).
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received February 27, 2023.
- Accepted after revision April 10, 2023.
- © 2023 by American Journal of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Optimizing Photon-Counting Detector CT for Imaging Intracranial Aneurysms
- Management of wide-neck aneurysms in 2024: how does one make the best treatment decision when there are so many good options?
- Response to: Correspondence on "Cerebral aneurysms: Germany-wide real-world outcome data of endovascular or neurosurgical treatment from 2007 to 2019" by Cole
- Reply:
- Appreciation and Concerns Regarding the Published Study "CURES"