
Abstract
BACKGROUND AND PURPOSE: Combination radiofrequency ablation and vertebral augmentation is an emerging minimally invasive therapy for patients with metastatic spine disease who have not responded to or have contraindications to radiation therapy. The purpose of this study was to evaluate the rate of radiographic local control of spinal metastases treated with combination radiofrequency ablation and vertebral augmentation.
MATERIALS AND METHODS: We retrospectively reviewed our tumor ablation database for all patients who underwent radiofrequency ablation and vertebral augmentation of spinal metastases between April 2012 and July 2014. Tumors treated in conjunction with radiation therapy were excluded. Tumor characteristics, procedural details, and complications were recorded. Posttreatment imaging was reviewed for radiographic evidence of tumor progression.
RESULTS: Fifty-five tumors met study inclusion criteria. Radiographic local tumor control rates were 89% (41/46) at 3 months, 74% (26/35) at 6 months, and 70% (21/30) at 1 year after treatment. Clinical follow-up was available in 93% (51/55) of cases. The median duration of clinical follow-up was 34 weeks (interquartile range, 15–89 weeks), during which no complications were reported and no patients had clinical evidence of metastatic spinal cord compression at the treated levels.
CONCLUSIONS: Combination radiofrequency ablation and vertebral augmentation appears to be an effective treatment for achieving local control of spinal metastases. A prospective clinical trial is now needed to replicate these results.
ABBREVIATION:
- RFA
- radiofrequency ablation
Metastatic spine disease affects 5%–10% of patients with cancer.1 Approximately 90% of symptomatic patients present with pain, which is most commonly due to biochemical stimulation of endosteal nociceptors, tumor mass effect, and/or associated pathologic fracture.2 These patients are also at risk for metastatic spinal cord compression, which occurs in 10%–20% of patients and is most often due to posterior extension of vertebral body tumor.3,4 The resulting pain and neurologic deficits are associated with decreased quality of life and shortened life expectancy.5 Therefore, the goals of treatment are both pain palliation and local tumor control.
Radiation therapy is the standard of care for pain palliation and local control of spinal metastases, but it has several important limitations. First, certain tumor histologies respond less favorably to radiation therapy, particularly non-small cell lung cancer, renal cell carcinoma, melanoma, and sarcoma.6 Second, radiation therapy of spinal metastases is limited by the cumulative tolerance of the spinal cord, which often precludes retreatment of recurrent disease or progressive disease at adjacent vertebral levels.7 Third, radiation therapy excludes patients from certain systemic chemotherapy clinical trials.
Combination radiofrequency ablation (RFA) and vertebral augmentation is an emerging minimally invasive therapy for patients with metastatic spine disease who have not responded to or have contraindications to radiation therapy. An ablation probe is percutaneously placed into the tumor, and high-frequency alternating current is passed through an electrode at the probe tip, generating frictional heating and necrosis of adjacent tissue.8 Cement is then instilled through the same percutaneous cannula to stabilize or prevent associated pathologic fracture.9,10 The tandem procedure can be performed in an outpatient setting with the patient under conscious sedation, requires minimal recovery, and does not hinder or delay adjuvant therapies such as radiation or systemic chemotherapy. Multiple case series have shown decreased pain scores after RFA and vertebral augmentation of spinal metastases,11⇓⇓⇓–15 but evidence that percutaneous therapy achieves local tumor control is limited to case reports and small case series without internal controls.13,14 The purpose of this study was to retrospectively evaluate the rate of radiographic local control of spinal metastases treated with combination RFA and vertebral augmentation at a National Cancer Institute–Designated Cancer Center.
Materials and Methods
Institutional review board approval was obtained to retrospectively review our institutional database for all patients who underwent RFA and vertebral augmentation of osseous metastases between April 2012 and July 2014. Informed consent was waived for retrospective study participation. Tumors also treated with radiation therapy were excluded. Recorded data included patient demographics, primary tumor histology, and vertebrae treated. All available preprocedural imaging of each treated vertebra, including MR imaging, CT, and/or [18F] fluorodeoxyglucose (FDG) PET/CT, was reviewed to determine whether the tumor involved the posterior vertebral body and/or pedicles, had eroded the posterior vertebral body cortex, and/or was associated with pathologic vertebral compression fracture. Preprocedural tumor volumes were also estimated by measuring the greatest length of tumor in each dimension. We preferred to measure the dimensions of T2-hyperintense marrow replacement on MR imaging. If MR imaging was not available, the dimensions of osteolysis on CT were measured, though this measurement likely underestimated tumor size.
Procedure notes were reviewed to determine the percutaneous approach (ie, uni- versus bipedicular), number of ablations performed, and total ablation time at each vertebral level. Procedural complications were documented according to the Society of Interventional Radiology classification.16 Patients were clinically evaluated 1 hour after each procedure for evidence of acute complications, such as hematoma formation or neurologic injury. The duration of clinical follow-up was recorded for each patient, and electronic medical records were reviewed for evidence of delayed complications, such as infection.
Patient Selection for Radiofrequency Ablation and Vertebral Augmentation
Patients were selected for RFA and vertebral augmentation by a multidisciplinary team of radiation and medical oncologists, interventional radiologists, and spine surgeons. Treatments were performed to achieve local tumor control and, in most cases, pain relief. Treated patients could not receive radiation therapy or had radiographic tumor progression at other sites of disease treated with radiation therapy. Exclusion criteria for RFA and vertebral augmentation included metastases that were entirely osteoblastic, associated with pathologic compression fracture with spinal instability, or causing spinal cord compression. Tumor within 1 cm of the spinal cord or nerves was not a contraindication for treatment.
Radiofrequency Ablation and Vertebral Augmentation Procedure
Written informed consent was obtained before all treatments. All procedures were performed under fluoroscopic or CT guidance with the patient consciously sedated. The skin, soft tissues, and periosteum overlying the target vertebra were anesthetized with a 50/50 mixture of 1% lidocaine and 0.25% bupivacaine. The vertebral body was accessed from a transpedicular approach with a 10-ga introducer cannula, and a navigational osteotome was used to create channels in the marrow cavity corresponding to the planned placements of the ablation probe. In each case, the goal was to perform overlapping ablations that encompassed the entire volume of tumor on cross-sectional imaging and an additional 3-mm margin to account for microscopic tumor spread.9 A bipedicular approach was used when tumor extended across the sagittal vertebral body midline and could not be entirely ablated with an adequate margin from a unipedicular approach (Fig 1).

A 29-year-old woman with stage IV (T1b, N1, M1) cardiac angiosarcoma who presented with low back pain. Sagittal T1-weighted (A) and STIR (B) MR imaging show diffuse T1 hypointensity and heterogeneous T2 hyperintensity of the lumbar vertebral body marrow, consistent with marrow-replacing tumor. She was treated with conventional external-beam radiation therapy (30 Gy in 10 fractions); however, her back pain persisted. Sagittal STIR (C) and T1-weighted, fat-suppressed, postcontrast (D) MR imaging performed 5 months later show interval progression of multiple spinal metastases with new epidural extension of tumor at T11, L1, L2, and L3 (black block arrows) and pathologic fractures of the L2 and L3 vertebral bodies. She could not receive additional radiation therapy due to the cumulative dose to the spinal cord. Consequently, she underwent radiofrequency ablation and vertebral augmentation of T11, L1, L2, and L3. Anteroposterior (E) and lateral (F) fluoroscopic images show percutaneous cannulae in both pedicles of T11 and the ablation probe curving into the left posteroinferior vertebral body (black arrowheads). Sagittal STIR (G) and T1-weighted, fat-suppressed, postcontrast (H) MR imaging performed 6 months later show interval retraction of the epidural tumor at T11, L1, L2, and L3. Signal void corresponding to cement (white asterisks) with surrounding T2-hyperintense, enhancing granulation tissue is noted at the treated levels (white block arrows).
Ablations were performed with the STAR Tumor Ablation System (DFINE, San Jose, California). This system includes an ablation probe with an articulated distal segment that is essential for accessing tumor in the posterior central vertebral body (Fig 1).14 The probe also contains 2 thermocouples located 10 and 15 mm from the electrode, which permit real-time monitoring of the volume of the ablation zone. Each individual ablation was performed until the thermocouple located 15 mm from the electrode reached 50°C. Based on the manufacturer's thermal distribution curves, the dimensions of the ellipsoid ablation volume are 30 × 20 × 20 mm when the thermocouple located 15 mm from the electrode reaches 50°C.14 The electrode was placed no closer than 10 mm from the posterior vertebral body cortex, which is the maximum radius of the minor axis of the ellipsoid ablation volume. When ablation was performed near this threshold, a coaxial needle was placed through the neural foramen into the ventral epidural space, the inner cannula of which contained an additional thermocouple. If the temperature in the ventral epidural space exceeded 45°C, carbon dioxide and cooled 5% dextrose in water were injected through the outer cannula of the needle for thermal protection.8,17 Vertebral augmentation was performed by using the StabiliT Vertebral Augmentation System (DFINE). In all cases, cement was injected through the same percutaneous cannula used for ablation.
Local Control Assessment and Analysis
All available postprocedural imaging was reviewed, including MR imaging, CT, and/or FDG PET/CT. All follow-up imaging was performed for clinical reasons at the request of the referring oncologist. In general, CT and PET/CT were performed to assess the systemic chemotherapy response, and spinal MR imaging was performed when patients reported new or increasing spine-related pain. Local control failure was defined as the following: 1) increased osteolysis or paravertebral tumor extension on CT; 2) new or persistent enhancing soft tissue extending into the epidural space, neural foramina, or paravertebral space on MR imaging; or 3) persistent FDG uptake on PET/CT (Fig 2). Additionally, T1-hypointense, T2-hyperintense signal and/or enhancement at the margin of the ablation cavity on follow-up MR imaging were categorized as local control failure unless these findings remained stable on subsequent imaging, retraction of epidural tumor was seen, or a PET/CT scan was available demonstrating absence of associated FDG uptake (Fig 1).9 To serve as an internal control, posttreatment cross-sectional imaging was also reviewed for evidence of systemic disease progression, including enlargement of visceral or intracranial metastases or osseous metastases that were not ablated.

Examples of ablation failure. A, Axial CT image shows a T12 lytic squamous cell carcinoma metastasis. B, CT scan obtained 4 months after radiofrequency ablation and vertebral augmentation shows new osteolysis medial to the cement and extending across the midline (white arrow), consistent with progression of residual tumor. C, Axial postcontrast, T1-weighted, fat-suppressed MR imaging performed 6 months after radiofrequency ablation and vertebral augmentation of an L3 non-small cell carcinoma metastasis shows signal void corresponding to cement in the ablation cavity (white asterisk), with residual enhancing tumor in the right lateral and posterior vertebral body that extends into the epidural space (black asterisks). D, Axial [18F] fluorodeoxyglucose PET/CT scan obtained 1 month after radiofrequency ablation and vertebral augmentation of an L5 liposarcoma metastasis shows residual hypermetabolic tumor along the right anterolateral aspect of the vertebral body (white dashed arrow).
Results
Fifty-five spinal metastases treated with RFA and vertebral augmentation were included in the study. Radiation-resistant histologies comprised 62% (34/55) of treated tumors, including sarcomas (27%, 15/55), non-small cell lung cancer (16%, 9/55), renal cell carcinoma (11%, 6/55), and melanoma (7.3%, 4/55). Other histologies included breast adenocarcinoma (13%, 7/55), papillary thyroid cancer (9.1%, 5/55), hepatocellular carcinoma (3.6%, 2/55), head and neck squamous cell carcinoma (3.6%, 2/55), multiple myeloma (3.6%, 2/55), malignant peripheral nerve sheath tumor (3.6%, 2/55), and gastrointestinal adenocarcinoma (1.8%, 1/55). Median tumor volume was 10.0 mL (interquartile range, 4.9–15.3 mL). Forty-seven percent (26/55) of tumors involved thoracic and 53% (29/55) involved lumbar vertebrae. Seventy-three percent (40/55) of metastases involved the posterior vertebral body, 31% (17/55) were associated with erosion of the posterior vertebral body cortex, and 47% (26/55) involved the pedicles. Associated pathologic compression fractures were present in 62% (34/55) of treated vertebrae.
Sixty-nine percent (38/55) of ablations were performed from a unipedicular approach, and 31% (17/55) were performed from a bipedicular approach. Within each vertebra, the median number of ablations performed was 4 (range, 1–12) and the median cumulative ablation time was 5 minutes 5 seconds (range, 51 seconds to 19 minutes 13 seconds). According to the Society of Interventional Radiology classification, there were no acute or delayed procedure-related complications during the median clinical follow-up of 34 weeks (interquartile range, 15–89 weeks).
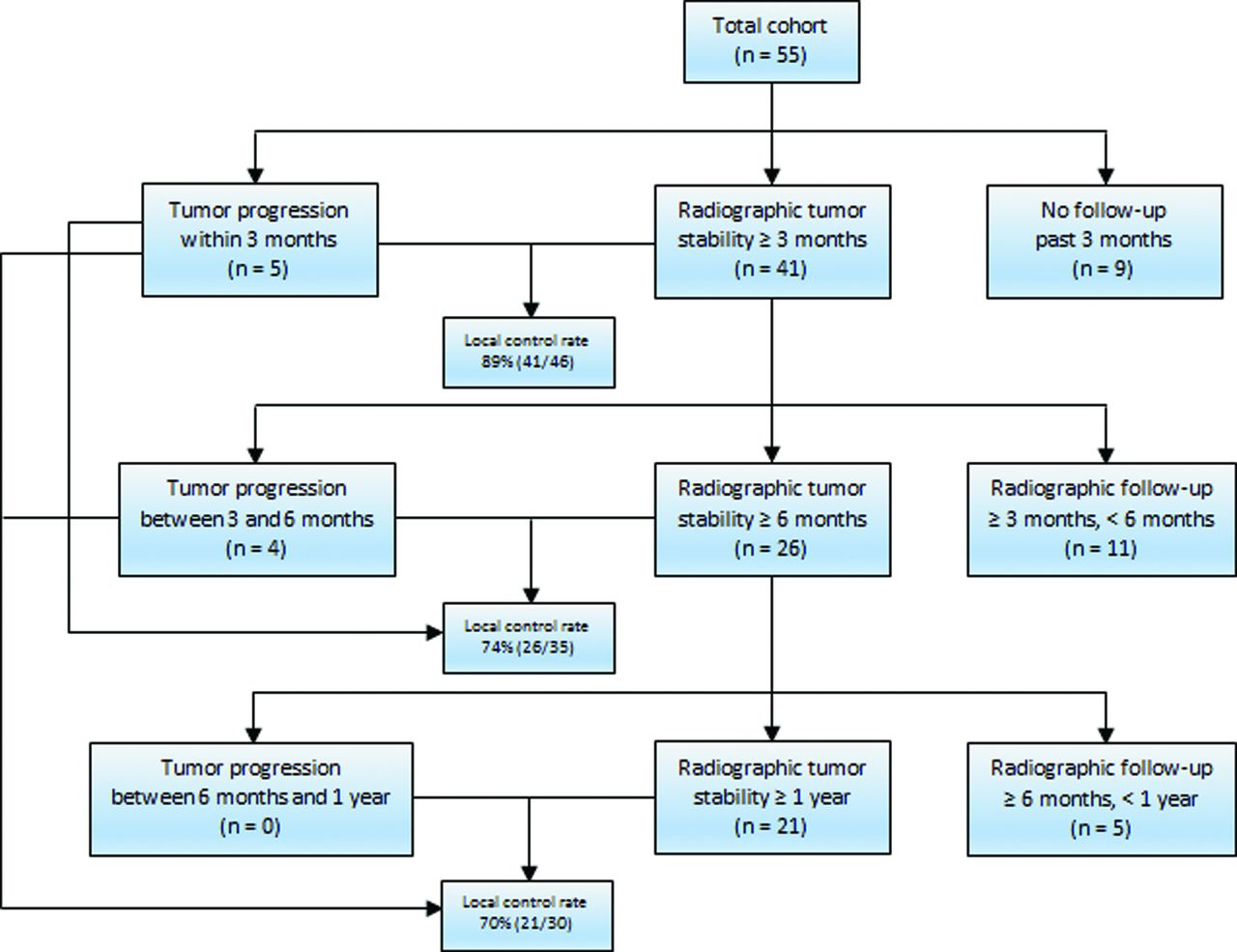
Radiographic follow-up results are summarized in Fig 3. Follow-up imaging included CT in 69% (38/55), MR imaging in 56% (31/55), and PET/CT in 40% (22/55) of cases. Five cases of residual or recurrent tumor were documented within 3 months of treatment. In all 5 of these cases, there was also evidence of systemic metastatic disease progression. Follow-up imaging demonstrating local tumor control at least 3 months after treatment was available for an additional 41 tumors. Thus, the radiographic local tumor control rate at 3 months was 89% (41/46). Imaging also demonstrated progression of systemic metastatic disease in 80% (37/46) of these cases. Thus, the 3-month radiographic local tumor control rate was 86% (32/37) in the setting of systemic metastatic disease progression. Nine tumors (16%; 9/55) did not have imaging demonstrating progression within 3 months of treatment or stability at least 3 months after treatment. These tumors were not reimaged because the patients entered hospice care due to progression of visceral or intracranial metastatic disease. None of the patients without follow-up imaging at least 3 months after treatment died with symptoms of metastatic spinal cord compression.

Flowchart summarizing overall radiographic local tumor control results at 3-month, 6-month, and 1-year follow-ups.
Four additional cases of tumor progression were documented between 3 and 6 months after treatment; thus, 9 total cases of tumor progression were documented within 6 months of treatment. Follow-up imaging demonstrating local tumor control at least 6 months after treatment was available for an additional 26 tumors. Thus, the radiographic local tumor control rate 6 months after treatment was 74% (26/35). Imaging also demonstrated progression of systemic metastatic disease in 89% (31/35) of these cases. Thus, the 6-month radiographic local tumor control rate was 71% (22/31) in the setting of systemic metastatic disease progression. Eleven tumors (27%; 11/41) with documented stability at least 3 months after treatment were not imaged again after 6 months. In 7 of these cases (64%; 7/11), posttreatment imaging was not performed because the patient was doing well clinically at the end of the study period with no back pain or neurologic deficits. One patient (9.1%; 1/11) died with metastatic spinal cord compression due to progression of an upper thoracic spinal metastasis that was not previously treated with RFA and vertebral augmentation. This patient had a lumbar spinal metastasis that was treated with RFA and vertebral augmentation that was stable on CT performed 3 months after treatment. Three patients (27%; 3/11) were lost to follow-up between 3 and 6 months after treatment.
No additional cases of tumor progression were documented between 6 months and 1 year after treatment. Follow-up imaging demonstrating local tumor control at least 1 year after treatment was available for an additional 21 tumors. Thus, the radiographic local tumor control rate 1 year after treatment was 70% (21/30). Imaging also demonstrated progression of systemic metastatic disease in 90% (27/30) of these cases. Thus, the 1-year radiographic local tumor control rate was 67% (18/27) in the setting of systemic metastatic disease progression. Five tumors (19%; 5/26) with at least 6 months of documented posttreatment stability were not imaged again after 1 year. In 3 of these cases (60%; 3/5), posttreatment imaging was not performed because the patient was doing well clinically at the end of the study period with no back pain or neurologic deficits. One patient (20%, 1/5) entered hospice care due to progression of visceral metastatic disease, and 1 patient (20%, 1/5) was lost to follow-up.
Of the 9 cases in which radiographic local tumor control was not achieved, the median time to documented tumor progression was 12.1 weeks (range, 3–20 weeks). Residual or recurrent tumor was present in the posterior vertebral body and/or epidural space in 89% (8/9) of cases, and in the anterolateral vertebral body in 1 case (11%; 1/9). In 89% (8/9) of cases, the ablation was performed from a bipedicular approach. In the one case in which failure occurred after a unipedicular approach, tumor recurrence occurred in the contralateral hemivertebral body (Fig 2).
Discussion
In the present study, combination RFA and vertebral augmentation achieved 1-year radiographic local control rates of 70% (21/30) overall and 67% (18/27) in the setting of systemic metastatic disease progression. These results suggest the possibility of a new, multidisciplinary paradigm for managing metastatic spine disease that incorporates RFA and vertebral augmentation for local tumor control.18 Although radiation therapy is the standard of care for palliation and local control of osseous metastatic disease, RFA and vertebral augmentation may be an effective alternative for patients who cannot be offered or cannot tolerate radiation therapy or have radiation-resistant tumors (Fig 1). A prospective clinical trial is now needed to replicate these results.
In the 9 cases in which RFA and vertebral augmentation did not achieve local tumor control, residual or recurrent tumor was most commonly present in the posterior vertebral body and/or epidural space (89%, 8/9). These results are expected, because it can be difficult to ablate tumor in these areas without also heating adjacent spinal nerves. We perform RFA with the patient under conscious sedation, in part, so that patients can react to and express new radicular pain indicating that the spinal nerves are being heated to dangerous temperatures. When this happens, ablation is terminated to avoid thermal nerve injury, though the result is often less thorough tumor ablation. The efficacy of radiation therapy similarly declines with decreasing distance between the tumor and the spinal cord, because of the risk of radiation-induced myelopathy.7 In several such cases, our multidisciplinary team has used radiation therapy in combination with RFA and vertebral augmentation. Greenwood et al19 recently reported our initial experience with this strategy, which achieved radiographic local tumor control rates of 92% (12/13) and 100% (10/10) at 3- and 6-month follow-ups, respectively, despite systemic metastatic disease progression. A prospective trial is needed to determine if combination radiation therapy, RFA, and vertebral augmentation achieves better results than radiation or percutaneous therapy alone.
One case of ablation failure occurred in the hemivertebral body contralateral to where ablation was performed (Fig 2). Although the entirety of osteolysis on pretreatment CT was confined to the right hemivertebral body and was accessible from a right unipedicular approach, microscopic tumor infiltration into the left hemivertebral body was presumably beyond the margin of the ablation zone. As a result of this case, our current practice is to ablate the entire volume of T2-hyperintense marrow signal and enhancement on MR imaging, or the entire volume of FDG avidity within the vertebral body on PET/CT, as well as an additional 3-mm margin to account for microscopic tumor infiltration.16
In addition to being a retrospective study with a heterogeneous cohort of tumor histologies, the most important limitation of this study is the number of patients without 3-month, 6-month, or 1-year imaging follow-up. Three factors account for this limitation: First, there was no routine follow-up imaging protocol. This introduced selection bias that may have resulted in underestimation of local control rates, because oncologists are less likely to obtain imaging in patients with clinically stable disease. Second, patients died or entered hospice care. These results are expected in a cohort of patients with metastatic disease, and chart review revealed that these outcomes were not due to metastatic spinal cord compression at the levels treated with RFA and vertebral augmentation. Third, patients were lost to follow-up entirely. As in all outcome-based studies, this group has the greatest potential to bias the results. However, these patients only accounted for 7.3% (4/55) of the original cohort.
Another limitation is the lack of established criteria for the radiographic diagnosis of recurrent or residual tumor. Ideally, radiographic differentiation of tumor from postablation changes would be based on histopathologic–MR imaging correlation, as has been done with soft-tissue tumors.20⇓–22 However, vertebral augmentation prevents re-access to the vertebral body for biopsy. Increased osteolysis on CT is a reasonable criterion for tumor progression, because animal studies have shown that the lamellar structure of bone is preserved after RFA.23 The MR imaging criteria of T2 hyperintensity and enhancement adjacent to the ablation cavity are nonspecific, because ablation produces a rim of granulation tissue around the ablation cavity that, like tumor, is T1 hypointense, T2 hyperintense, and enhances.9 Furthermore, granulation tissue can evolve with time, thus mimicking tumor progression.20 To avoid overestimating the rate of local tumor control, we assumed that residual T1-hypointense, T2-hyperintense signal and enhancement at the margin of the ablation cavity represented residual tumor unless follow-up MR imaging showed stable findings or retraction of epidural tumor (Fig 1), or a PET/CT was available demonstrating absence of associated FDG uptake.
Conclusions
Radiofrequency ablation and vertebral augmentation appears in this retrospective study to be an effective treatment for achieving local control of spinal metastases. A prospective clinical trial is now needed to replicate these results.
Footnotes
Disclosures: Adam N. Wallace—UNRELATED: Grants/Grants Pending: DFINE is donating ablation probes for an animal research study; OTHER RELATIONSHIPS: DFINE paid for travel expenses for the Metastatic Spine Disease Multidisciplinary Working Group meeting in January 2014. Jack W. Jennings—UNRELATED: Consultancy: DFINE; Payment for Lectures (including service on Speakers Bureaus): DFINE speaker panel.
REFERENCES
- Received July 27, 2015.
- Accepted after revision August 18, 2015.
- © 2016 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Photodynamic Therapy for the Treatment of Vertebral Metastases: A Phase I Clinical Trial
- Percutaneous Radiofrequency Ablation of Spinal Osteoid Osteomas Using a Targeted Navigational Bipolar Electrode System
- Simultaneous Bipedicular Radiofrequency Ablation Combined with Vertebral Augmentation for Local Tumor Control of Spinal Metastases
- Republished: Renal cell carcinoma metastasis involving vertebral hemangioma: dual percutaneous treatment by navigational bipolar radiofrequency ablation and high viscosity cement vertebroplasty
- Percutaneous Spinal Ablation in a Sheep Model: Protective Capacity of an Intact Cortex, Correlation of Ablation Parameters with Ablation Zone Size, and Correlation of Postablation MRI and Pathologic Findings
- Is an Intact Posterior Vertebral Body Cortex Protective for Percutaneous Ablation?
- Renal cell carcinoma metastasis involving vertebral hemangioma: dual percutaneous treatment by navigational bipolar radiofrequency ablation and high viscosity cement vertebroplasty