
Abstract
BACKGROUND AND PURPOSE: Standard selection criteria for revascularization therapy usually exclude patients with unclear-onset stroke. Our aim was to evaluate the efficacy and safety of revascularization therapy in patients with unclear-onset stroke in the anterior circulation and to identify the predictive factors for favorable clinical outcome.
MATERIALS AND METHODS: We retrospectively analyzed 41 consecutive patients presenting with acute stroke with unknown time of onset treated by intravenous thrombolysis and/or mechanical thrombectomy. Only patients without well-developed fluid-attenuated inversion recovery changes of acute diffusion lesions on MR imaging were enrolled. Twenty-one patients were treated by intravenous thrombolysis; 19 received, simultaneously, intravenous thrombolysis and mechanical thrombectomy (as a bridging therapy); and 1 patient, endovascular therapy alone. Clinical outcome was evaluated at 90 days by using the mRS. Mortality and symptomatic intracranial hemorrhage were also reported.
RESULTS: Median patient age was 72 years (range, 17–89 years). Mean initial NIHSS score was 14.5 ± 5.7. Successful recanalization (TICI 2b–3) was assessed in 61% of patients presenting with an arterial occlusion, symptomatic intracranial hemorrhage occurred in 2 patients (4.9%), and 3 (7.3%) patients died. After 90 days, favorable outcome (mRS 0–2) was observed in 25 (61%) patients. Following multivariate analysis, initial NIHSS score (OR, 1.43; 95% CI, 1.13–1.82; P = .003) and bridging therapy (OR, 37.92; 95% CI, 2.43–591.35; P = .009) were independently associated with a favorable outcome at 3 months.
CONCLUSIONS: The study demonstrates the safety and good clinical outcome of acute recanalization therapy in patients with acute stroke in the anterior circulation and an unknown time of onset and a DWI/FLAIR mismatch on imaging. Moreover, bridging therapy versus intravenous thrombolysis alone was independently associated with favorable outcome at 3 months.
ABBREVIATIONS:
- FAT
- first found abnormal time
- GRAPPA
- generalized autocalibrating partially parallel acquisition
- IVT
- intravenous thrombolysis
- sICH
- symptomatic intracranial hemorrhage
Acute ischemic strokes with an unknown time of symptom onset occur in approximately 25% of patients.1 Hence, these patients are usually excluded from intravenous thrombolysis (IVT).2 However, many patients with an unknown stroke onset could also benefit from this treatment. In a subset of these patients, it has been shown that the clinical features and imaging characteristics do not differ significantly from those in patients with a known time of onset.1 MR imaging could be helpful if it is used as a “clock” for stroke of unknown time onset; indeed, in a recent multicenter observational study of patients with stroke with known time of symptom onset, the DWI-FLAIR mismatch, defined by positive findings on DWI and negative findings on FLAIR, was effective in identifying patients within 4.5 hours of symptom onset.3
To date, limited studies have focused on the safety and effectiveness of IVT in patients with a stroke of unknown onset time, especially by using MR imaging–specific eligibility criteria.4⇓⇓⇓⇓–9 Only a few reports have evaluated the feasibility of endovascular therapies in patients with wake-up stroke.10⇓–12 Recently, randomized studies have demonstrated that mechanical thrombectomy is an alternative and synergistic method of treatment to IVT in acute ischemic stroke, with a higher recanalization rate (66%–100%) and a more favorable outcome (32.6%–71%).13⇓⇓⇓–17
The aim of this study was to describe the experience of our center with 41 patients presenting with a stroke of an unknown time of symptom onset in the anterior circulation, who were treated by using a coalescent stroke-management protocol with IVT, mechanical thrombectomy, or bridging therapy based on DWI/FLAIR mismatch. We also assessed predictive factors for favorable outcome at 3 months and evaluated the feasibility, safety, and efficacy of revascularization therapy in these patients.
Materials and Methods
All consecutive patients admitted in our stroke unit with a stroke of unknown time of onset and treated by reperfusion therapy between October 2010 and October 2013 were included in this study. The patient demographics, risk factors, and clinical and imaging data were prospectively registered in our stroke databank. The NIHSS score was systematically assessed by a stroke neurologist on admission. This study was approved by the local ethics committee. Consent for treatment was obtained from the patients or their family before the endovascular procedure.
The inclusion criteria were as follows: 1) patients with acute stroke without a known time of symptom onset, presenting to our emergency department within 4 hours after the first found abnormal time (FAT); 2) acute ischemic lesions within the anterior circulation on DWI; 3) an ASPECTS of ≥5; 4) the presence of a DWI/FLAIR mismatch according to Thomalla et al3; 5) the presence of a clinically relevant impairment in social, occupational, or other important areas of functioning following a physician evaluation; and 6) the presence of clinical-diffusion mismatch between stroke severity and volume of DWI lesions assessed by visual inspection. For mechanical thrombectomy, patients were selected if they had the following additional criteria: 1) the presence of a proximal intracranial artery occlusion in the stroke territory; 2) an NIHSS score of ≥8; 3) a premorbid mRS of <1; and 4) initiation of endovascular treatment within 6 hours of FAT.
In cases of anterior cerebral artery stroke, the MR imaging eligibility criterion was an infarct volume <50% of the arterial territory.
MR Imaging Protocol
Multimodal MR imaging was performed in all patients by using a 1.5T magnet (Gyroscan Intera, Release 10; Philips Healthcare, Best, the Netherlands; 33-mT/m hypergradients). The MR imaging protocol included the following sequences: T2 gradient echo (TR/TE = 900/27 ms; flip angle = 15°; 1 repetition; generalized autocalibrating partially parallel acquisition [GRAPPA] = 2; 5.0-mm section thickness with no intersection gap; voxel size = 1.3 × 0.9 × 5 mm); DWI (TR/TE = 3600/83 ms; b-values = 0 and 1000 s/mm2; 2 repetitions; GRAPPA = 2; 5.0-mm section thickness with no intersection gap; voxel size = 1.8 × 1.8 × 5 mm); an ADC map; FLAIR (TR/TE = 8000/94 ms; TI = 2500 ms; turbo factor = 15; GRAPPA = 2; 5.0-mm section thickness with no intersection gap; voxel size = 0.6 × 0.6 × 5 mm); and T1 contrast-enhanced MRA (3D coronal gradient echo: TR/TE = 3.45/1.28 ms; flip angle = 25°; GRAPPA = 2; 144 sections; voxel size = 0.7 × 0.7 × 0.7 mm; gadolinium contrast agent, 0.5 mmol/mL, 0.2 mL/kg; flow rate = 2 mL/sec) of the supra-aortic trunks and intracranial vessels.
The DWI/FLAIR mismatch was defined according to Thomalla et al.3 It was diagnosed when a visible acute ischemic lesion was present on DWI with no traceable parenchymal hyperintensity in the corresponding region on FLAIR imaging. Collateral blood flow in the distal cerebral artery territory was defined on FLAIR by linear or serpentine vascular hyperintensities relative to gray matter in the MCA territory subarachnoid space. It was graded as “present” if vascular hyperintensities in the sulci were seen on FLAIR images or as “absent” if they were not detectable.
Revascularization Protocol
IVT (0.9 mg/kg) was administered to patients within a maximum of 4.5 hours of FAT. Conventional clinical and laboratory inclusion and exclusion criteria for IVT were applied.2 In cases of bridging therapy, patients were transferred to the angiographic suite for thrombectomy as soon as possible. Among patients with contraindications to IVT, thrombectomy alone was performed.
Mechanical thrombectomy was performed via a femoral artery approach with the patient under general anesthesia with the Solitaire FR device (Covidien, Irvine, California). General anesthesia included urinary bladder catheterization and endotracheal intubation without neuromuscular blockade.
An 8F or 9F Merci balloon-guide catheter (Concentric Medical, Mountain View, California) was inserted through a sheath. A 0.21-inch-internal-diameter microcatheter (Prowler Select Plus; Codman & Shurtleff, Raynham, Massachusetts; or Vasco 21; Balt, Montmorency, France) was navigated distal to the occlusion over a 0.014-inch steerable guidewire, which was then exchanged with the thrombectomy device. During the retrieval, the balloon-guide catheter was inflated to interrupt anterograde flow. Manual aspiration with a 50-mL syringe was performed through the hemostatic valve during the retrieval, to reverse the flow and aspirate clot debris possibly lost in the guide catheter lumen. The number of attempts to retrieve the thrombus was limited to 5 passes by the occluded vessel. Neither IV heparin nor intra-arterial fibrinolytics were administered at any time during the procedure. Blood pressure was carefully monitored during anesthetic induction and during the procedure, with a minimal threshold set at 90 mm Hg (mean arterial pressure). Hypotension was rapidly corrected if needed. Following any complications, extubation was planned at the end of the procedure and the patient was transferred to the intensive care unit.
Follow-up CT or MR imaging was performed 24 hours after the acute therapy to assess the extent of the infarction and/or hemorrhagic complications. If no hemorrhage was present, antiplatelet drugs were administered.
Outcome Measures
Successful recanalization, defined as TICI 2b or 3, was assessed at the end of the procedure in patients treated with thrombectomy. In patients treated with IVT, recanalization at 1 day was considered successful if follow-up MRA or angio-CT demonstrated complete visualization of the occluded artery, without residual stenosis of >50%.
“Symptomatic intracranial hemorrhage” (sICH) was defined as a documented hemorrhage on CT or MR imaging with a decline of ≥4 points in the NIHSS score. Device-related complications were also reported. Clinical outcome was quantified by mRS and mortality at day 90. Favorable outcome at 90 days was defined as an mRS score of ≤2.
Statistical Analysis
Patients with a favorable or poor outcome were compared by using the Student t or Mann-Whitney test for continuous variables and the χ2 or Fisher test for categoric variables. Bivariate logistic regressions were used to identify predictors of favorable outcome. Potential independent predictors (P < .25 in bivariate logistic regressions) were included in a multivariate logistic regression, built by stepwise procedure. Adjusted odds ratios and their 95% confidence intervals were calculated. The statistical significance threshold was set at 5%. Statistical analyses were conducted by using SAS software 9.2 (SAS Institute, Cary, North Carolina).
Results
Population Data
Overall, 41 patients with unclear-onset stroke in the anterior circulation (median age, 72 years; range, 17–89 years; female/male ratio, 26:15) were included. Baseline clinical and radiologic features and main clinical outcomes at day 90 are presented in the Online Table.
The median time interval between last-seen-normal time and hospital admission was 490 minutes (interquartile range, 255–641 minutes). The mean NIHSS score was 14.5 ± 5.7. The median time interval from FAT to MR imaging was 135 minutes (interquartile range, 109–158 minutes) and 517 minutes (interquartile range, 314–678 minutes) from last-seen-normal time. The median DWI ASPECTS was 8 (range, 5–10). Thirty-six patients (88%) showed an arterial occlusion in the anterior circulation. Occlusion sites were the proximal MCA (M1) in 28 cases (68.3%), the distal MCA (M2, M3) in 5 cases (12.1%), and the anterior cerebral artery in 3 cases (7.3%). The internal carotid artery was occluded in 14 patients (34.1%), including 9 patients with tandem cervical ICA and intracranial occlusions and 5 carotid bifurcation occlusions.
Stroke-Management Protocol
Nineteen patients (46.3%) underwent bridging therapy, and 21 patients (51.2%), IVT alone. In these patients, the exclusion criteria for thrombectomy included the following: no occluded intracranial artery (5 patients), NIHSS score of <8 (4 patients), distal cerebral artery occlusion (5 patients), premorbid mRS of >1 (3 patients), fast recovery symptoms after IVT administration (1 patient), and delay beyond 6 hours after FAT (3 patients). The mean time from initial MR imaging to the start of IVT was 51 ± 24 minutes. One patient with uncontrolled hypertension was treated by mechanical thrombectomy alone.
For the 20 patients treated by mechanical thrombectomy, the median number of passes with the thrombectomy device was 2 (range, 1–5). The thrombectomy procedure failed in 2 cases because of an inability to advance the microcatheter in the proximal ICA. Immediate successful recanalization (TICI ≥2b) was achieved in 15 patients (75%), and TICI 3 was achieved in 40% (8/20). The mean time from MR imaging to groin puncture was 81 ± 38 minutes. The median time from groin puncture to maximum final TICI was 60 minutes (range, 21–248 minutes). The mean time from FAT to recanalization was 295 ± 75 minutes and 686 ± 196 minutes from last-seen-normal-time.
Outcome
Four device-related complications occurred without neurologic deterioration or clinical sequelae, including 1 vessel perforation, 1 cervical ICA dissection, and 2 distal asymptomatic embolizations. Two (4.9%) patients had sICH related to the acute therapy within the first 24 hours with a favorable outcome. Three (7.3%) patients died during their hospital stay. Favorable outcome (mRS ≤2) was observed in 25 (61%) patients, including 14 (70%) patients of the 20 treated by mechanical thrombectomy and 11 (52%) of the 21 treated by IVT alone. A representative case is shown in Fig 1.

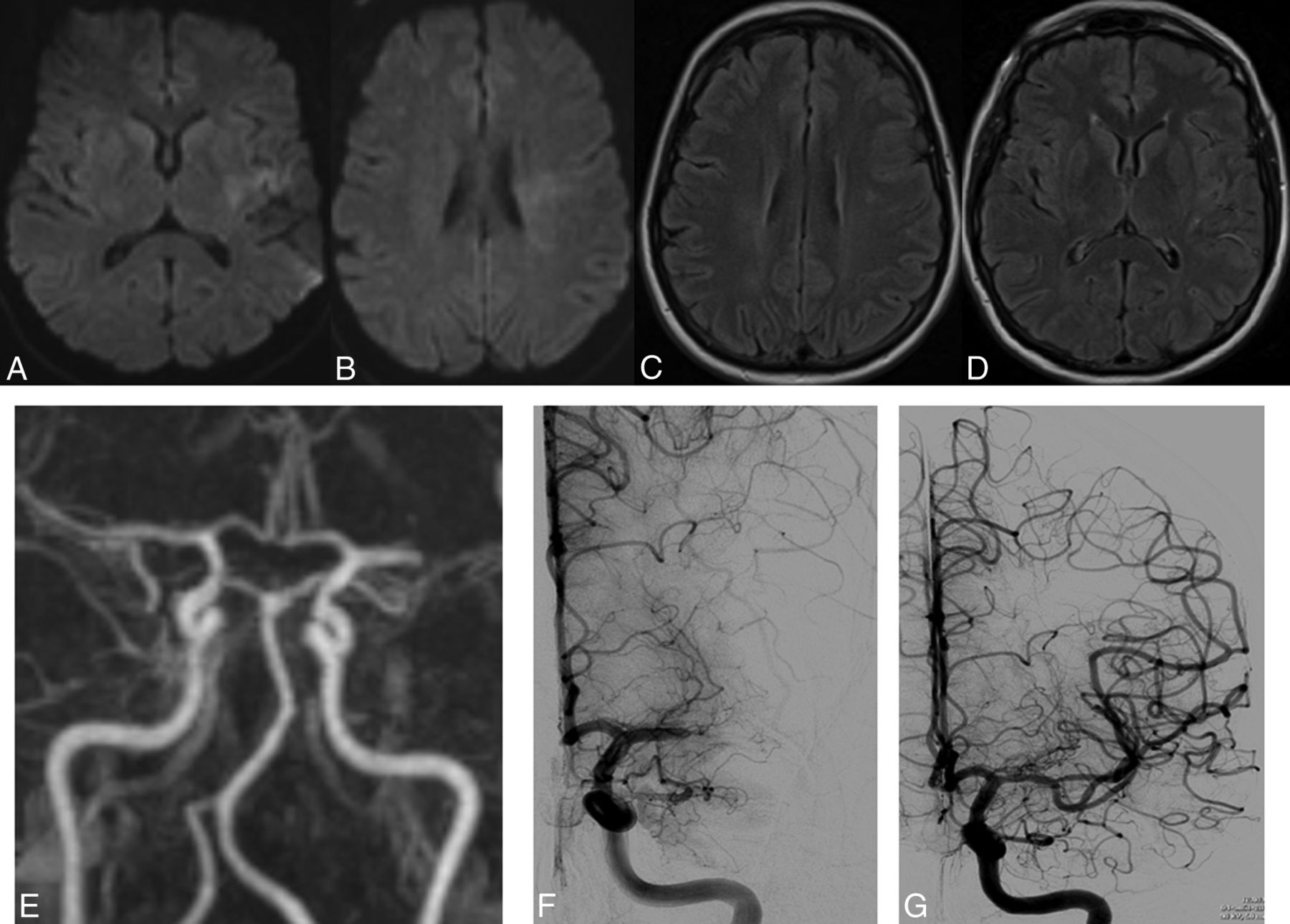
A 49-year-old woman presented with right hemiplegia and dysarthria (NIHSS score, 13). The patient arrived at the emergency department 72 minutes after symptom detection. MR imaging showed an acute ischemic lesion in the left MCA territory on DWI (A and B) without parenchymal signal changes on FLAIR (C and D) and occlusion of the left MCA (M1 segment) with collateral blood flow in the distal cerebral artery territory on MRA (E). Intravenous thrombolysis was started (0.9 mg/kg) 140 minutes after symptom detection. On DSA, the left MCA was still occluded on the M1 segment (F) and was recanalized after mechanical thrombectomy (TICI 3) (G). Time from symptom detection to recanalization was 189 minutes (3 hours 9 minutes). The mRS score at 3 months was zero.
Predictive Factors for Clinical Outcome
Compared with patients treated by IVT alone, patients treated with bridging therapy showed a statistically significant difference in a number of parameters. Patients were younger (P = .041) with a lower systolic blood pressure level at admission (P = .017), a higher NIHSS score (P = .007), and a lower ASPECTS (P = .022). Their recanalization rate (P = .023) was better (On-line Table).
The variables entered in the multivariate logistic regression analysis exploring predictive factors associated with a favorable outcome at day 90 (mRS ≤2) were age, initial systolic blood pressure, initial blood glucose level, initial NIHSS score, IVT versus bridging therapy, and time interval from FAT to treatment initiation. In the final adjusted model, each 1-point decrease of the initial NIHSS score was independently associated with a favorable outcome at day 90 (OR, 1.43; 95% CI, 1.13–1.82; P = .003) in patients with unclear-onset stroke and bridging therapy versus IV thrombolysis (OR, 37.92; 95% CI, 2.43–591.35; P = .009) (Table).
Predictive factors associated with favorable outcome at day 90 (mRS ≤2)
Discussion
Our study provided 2 important findings: 1) Reperfusion therapy based on DWI/FLAIR mismatch in patients with unclear-onset stroke seems to be efficient and safe, and 2) bridging therapy versus IVT alone is independently associated with favorable outcome at 3 months.
Our results are comparable with those of studies of IVT by using MR imaging variables (DWI/PWI, DWI/FLAIR mismatch) for patient selection, which showed favorable clinical outcome (40%–56.3% for mRS 0–2) and acceptable mortality (0%–10.3%) and sICH (0%–10.3%) rates.6⇓⇓–9 In contrast, CT-based thrombolysis in patients with wake-up stroke showed variable results. The only randomized controlled trial with thrombolytic treatment based on CT selection was stopped early because the rate of sICH was significantly higher in patients with wake-up stroke (13.6%) than in the other patients with stroke (4.0%).18 Barreto et al,4 by using noncontrast cranial CT, found, retrospectively, that 46 patients with intravenous thrombolysis and wake-up stroke had a significantly higher rate of favorable outcome (28% versus 13%; P = .006) but a higher mortality rate (15% versus 0%) than 34 patients with wake-up stroke treated without thrombolysis.
In the literature, there are only a few reports of patients with an acute stroke of unknown time of onset who underwent multimodal reperfusion therapy or endovascular therapy. In the Reperfusion Therapy in Unclear-Onset Stroke Based on MRI Evaluation trial, a prospective study using MR imaging criteria in 83 patients with an unknown time of onset,19 more than two-thirds of patients received endovascular treatment and approximately 10% received IVT alone. Favorable outcome (mRS 0–2) was achieved in 44.6%, and sICH was seen in 3.6%. Natarajan et al11 performed a retrospective review of 30 patients with significant salvageable brain tissue identified on CT perfusion who underwent endovascular recanalization (intra-arterial thrombolysis, mechanical thrombectomy, or angioplasty) ≥8 hours after last-seen-normal time, including those with wake-up stroke; partial/complete recanalization was achieved in 66.7% of patients, with 20% presenting with mRS 0–2 at 3 months. Overall mortality was 33.3%, and sICH was 10%.
Recently, Stampfl et al12 retrospectively analyzed clinical and angiographic data in 19 patients with wake-up stroke and diffusion/perfusion mismatch on MR or CT imaging treated with stent-retriever devices. Despite successful and rapid recanalization (94.7% of TICI ≥2), clinical outcome remained poor (10.5% of mRS 0–2; 36.8% died), and sICH occurred in 21.1% of patients. The authors underlined the difficulty of patient selection for endovascular therapy. Despite a lower recanalization rate, our results are better than those previously published for multimodal reperfusion therapy11,19 or endovascular treatment12 in terms of the frequency of good outcome (61% versus 10.5%–44.6%), mortality (7.3% versus 33.3%–36.8%), and sICH (4.9% versus 3.6%–21.1%) rates.
Recently 3 randomized studies13⇓⇓⇓–17 reported the superiority of rapid thrombectomy, compared with IVT alone, in patients with acute ischemic stroke with a proximal intracranial occlusion and improving reperfusion (66%–100% for intervention versus 31.2%–37% for controls) and functional outcome at 90 days (32.6%–71% for intervention versus 19.1%–40% for controls). There were no significant differences in mortality (9%–18.9% for intervention versus 12%–20% for controls) or the occurrence of symptomatic intracerebral hemorrhage (0%–7.7% for intervention versus 1.9%–6.4% for controls).
In our study, patients treated with bridging therapy had more favorable outcome compared with patients treated with IVT alone. These results were shown despite the conditions of patients treated with bridging being more severe (worst NIHSS and ASPECTS at admission). Indeed, after adjusting for the initial NIHSS score, bridging therapy versus IVT alone was independently associated with favorable outcome at 3 months in patients with unclear-onset stroke. Even if there is a statistically significant difference between these 2 groups of patients, our results suggest that IVT followed by endovascular therapy combines the advantages of a rapid start of treatment with IVT2 and a greater likelihood of early recanalization.
Recently, several trials emphasized the importance of patient selection for reperfusion therapy, with the tissue clock shown by multiparametric MR imaging techniques.6⇓⇓–9,12 We selected, in our study, patients using DWI/FLAIR mismatch and clinical-diffusion mismatch among MR imaging criteria. As reported by Thomalla et al,3 a patient with an acute ischemic lesion detected with DWI but not with FLAIR imaging is likely to be within 4.5 hours of symptom onset with high specificity (78%; 95% CI, 72%–84%) and high positive predict value (83%; 95% CI, 79%–88%). Moreover, clinical-diffusion mismatch, which predicts the presence of PWI-DWI mismatch, may be associated with neurologic improvement in patients treated with IVT as reported by Terasawa et al.20 Indeed, a number of studies have provided support for penumbral-imaging selection, by using the perfusion-diffusion mismatch criteria for the treatment of acute ischemic stroke7⇓–9,12 because salvage of the ischemic penumbra has formed the theoretic basis of recanalization therapies. This criterion may be particularly helpful in late time windows, when the proportion of patients with penumbral tissue steadily decreases. Last, the results of Diffusion and Perfusion Imaging Evaluation for Understanding Stroke Evolution Study 2 demonstrated that reperfusion was associated with increased good functional outcome at day 9 in a defined target mismatch profile.21
Obvious limitations of our monocentric observational study were the small number of patients, a retrospective analysis of our prospective dataset performed, and no control group. Using predefined imaging criteria, several ongoing prospective clinical trials are testing the safety and efficiency of thrombolytic treatment in patients with stroke with an unknown time of onset.22
Conclusions
Our preliminary results suggest that MR imaging–based reperfusion therapy can safely and efficiently be applied to patients with acute stroke with an unknown time of onset (based on DWI/FLAIR mismatch). Moreover, this study underlines the fact that IVT combined with endovascular mechanical thrombectomy seems to be associated with favorable clinical outcome when patients are carefully selected. Nevertheless, multicenter randomized trials are required to confirm these results and to determine the optimal multimodal MR imaging criteria for patient selection and the optimal treatment strategies.
Footnotes
A.B. and V.C. contributed equally to this work.
Disclosures: Alain Bonafé—UNRELATED: Consultancy: Covidien (consultant for ev3), Stryker; Grants/Grants Pending: Covidien.* Vincent Costalat—Consultancy: Balt, Codman Neuro-DePuy Synthes, Stryker, MicroVention; Payment for Lectures (including service on Speakers Bureaus): Stryker, Balt; Payment for Development of Educational Presentations: Covidien, Stryker. *Money paid to the institution.
References
- Received January 6, 2015.
- Accepted after revision June 2, 2015.
- © 2016 by American Journal of Neuroradiology





{kind=link}