
Article Figures & Data
Figures
- Fig 1.
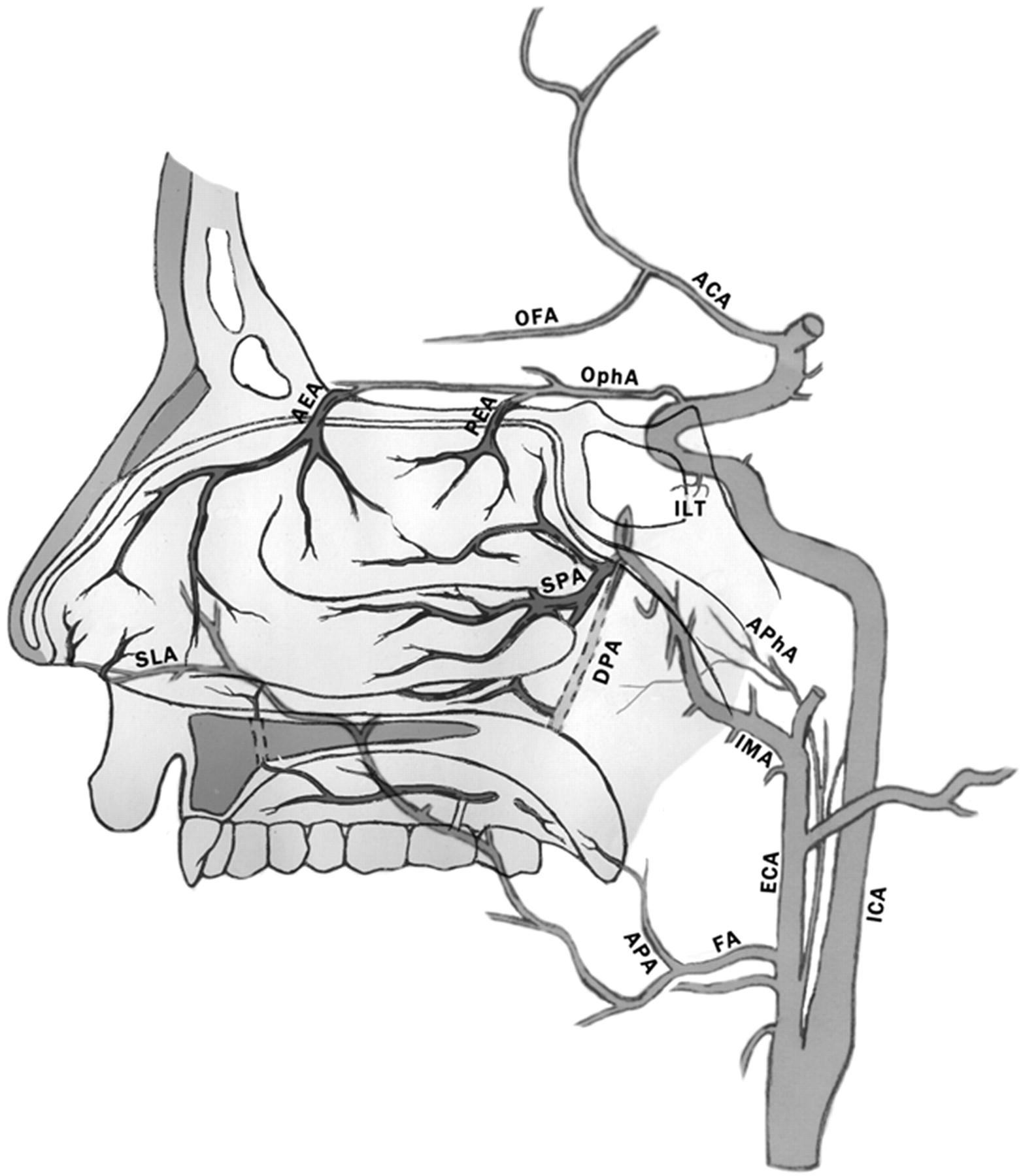
Schematic representation of normal arterial anatomy of the sinonasal region. ACA indicates anterior cerebral artery; AEA, anterior ethmoidal artery; APA, ascending palatine artery; APhA, ascending pharyngeal artery; DPA, descending palatine artery; ECA, external carotid artery; FA, facial artery; ICA, internal carotid artery; ILT, inferior lateral trunk; IMA, internal maxillary artery; OFA, orbitofrontal artery; OphA, ophthalmic artery; PEA, posterior ethmoidal artery; SLA, superior labial artery; SPA, sphenopalatine artery.
- Fig 2.
Oblique view of a right internal carotid arteriogram in a 19-year-old man, presenting with uncontrollable epistaxis 2 weeks after being struck in the face by a baseball bat, demonstrating a 5-mm pseudoaneurysm (arrow) arising from an AEA.
- Fig 3.
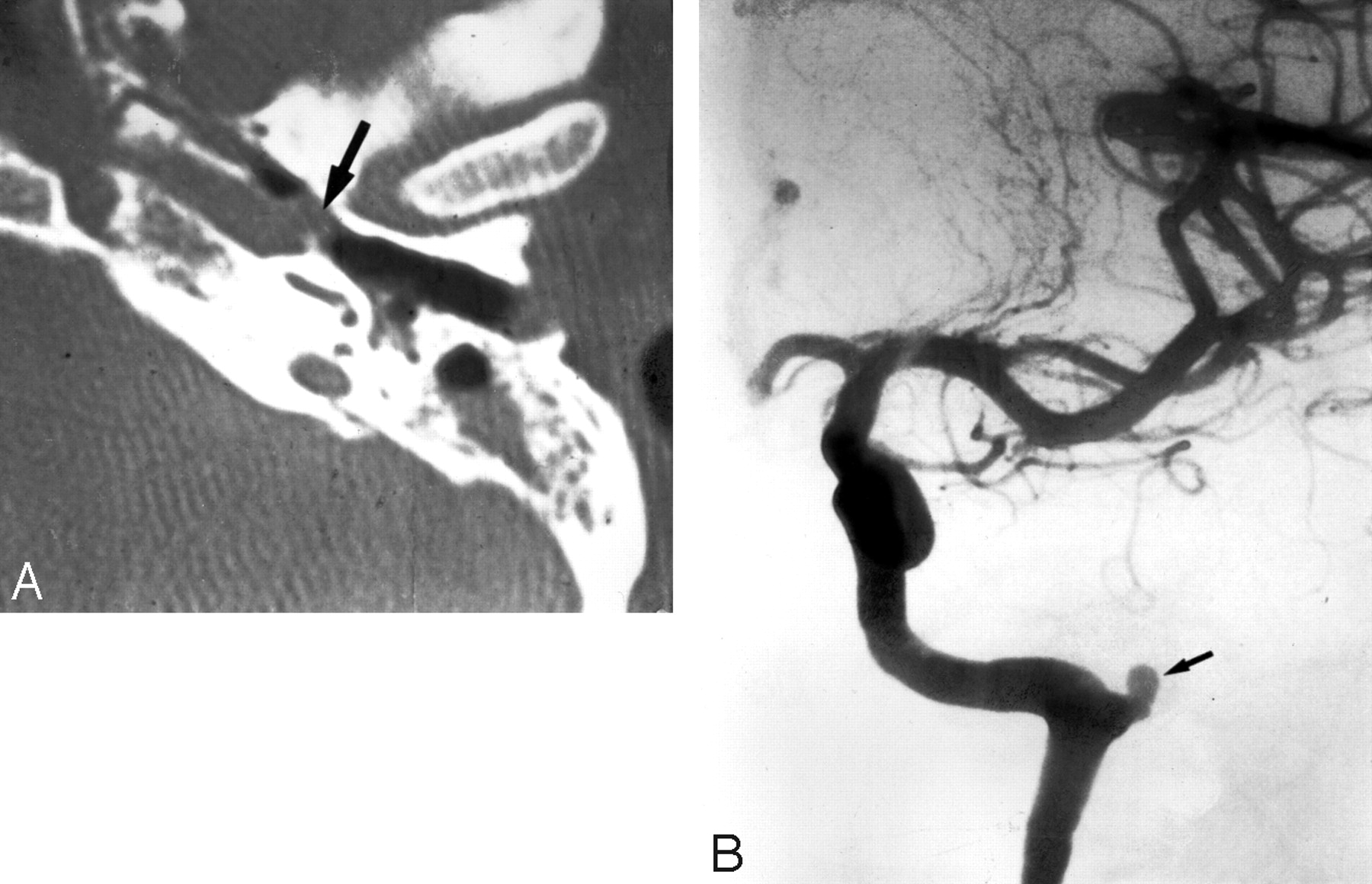
A 35-year-old woman, who presented with severe recurrent epistaxis. A, Nonenhanced axial CT scan shows a soft-tissue attenuation projecting from the carotid canal into the eustachian tube (arrow). B, AP view of a left internal carotid arteriogram, revealing a 6-mm aneurysm (arrow) projecting off the region of the petrous genu.
- Fig 4.
Oblique right internal carotid arteriogram of a 52-year-old woman with a 6-month history of severe recurrent epistaxis following a motor vehicle crash, revealing 2 large intracavernous traumatic pseudoaneurysms (curved arrows).
- Fig 5.
Left external carotid arteriography in a 26-year-old woman presenting with unrelenting epistaxis several hours after septorhinoplasty. Mid (A) and late (B) arterial phases demonstrate contrast extravasation (arrow), indicating the site of hemorrhage.
- Fig 6.
Angiographic imaging of a 35-year-old man with a history of recurrent epistaxis due to an AVM of the nose and upper lip. He had undergone previous surgical ligation of the proximal right ECA. A, Lateral view of a right internal carotid arteriogram demonstrates a large AVM (open arrows) with primary supply from the OphA (arrowheads). Collaterals to the SPA via the artery of the foramen rotundum (arrow) and the vidian artery (curved arrow) are seen. B, Lateral view of a right vertebral arteriogram demonstrating retrograde filling of the proximally occluded right ECA (curved arrow) via the occipital artery (arrows). The IMA is reconstituted to supply the AVM (open arrows).
- Fig 7.
Left internal carotid arteriogram of a 53-year-old woman, who presented with a 4-week history of recurrent epistaxis uncontrolled by AP packs and requiring multiple transfusions. The image reveals a small cerebral AVM with a nidus measuring <1 cm (curved arrow). The AVM is fed by an orbitofrontal branch (straight arrow) of the right anterior cerebral artery. Two early draining cortical veins are seen (arrowheads) as well as a small venous aneurysm distal to the nidus (open arrow). A small venous network is opacified in the nasal fossa (double arrow).
- Fig 8.
Imaging of a patient with HHT, for whom embolization was requested to treat recurrent epistaxis. A, Right external carotid arteriogram shows typical vascular changes in HHT along the hard palate (arrow) and the premaxilla (double arrow). B, Right internal carotid arteriogram of the same patient shows a small incidental AVM fed by small branches of the pericallosal artery (arrow).
- Fig 9.
Right external carotid arteriogram in a 12-year-old boy with a juvenile nasopharyngeal angiofibroma, who presented with nasal obstruction and recurrent epistaxis. A hypervascular mass arises from the pterygopalatine portion of the IMA (arrows).
- Fig 10.
Imaging of a 65-year-old man who presented with intractable epistaxis and whose history included right nephrectomy for renal cell carcinoma 5 years earlier. A, Axial CT scan at the level of the ethmoid sinuses shows a soft-tissue mass in the posterior ethmoidal air cells (arrows). B, Left external carotid arteriogram demonstrates the neovascularity (arrow) supplied by the terminal IMA.
- Fig 11.
Angiography in a 62-year-old man with right-sided epistaxis, demonstrating a meningo-ophthalmic artery (ie, the OphA arises from the MMA). Selective catheterization of the IMA distal to the origin of the MMA was necessary to perform embolization safely. A, Right internal carotid arteriogram demonstrates the absence of the OphA arising from the internal carotid system. B, Right external carotid arteriogram, early arterial phase, reveals the meningo-ophthalmic artery (arrows). C, The same image as in B, late arterial phase, confirms the choroidal blush (arrows) arising from the external carotid system.
- Fig 12.
Angiography in a 72-year-old woman with intractable idiopathic epistaxis, who was referred to surgery because an ECA origin of the OphA rendered embolization unsafe. A, Left common carotid arteriogram demonstrates ICA occlusion (arrow). B, The same image as A shows no antegrade or retrograde opacification of the OphA. C, Selective left IMA injection, early arterial phase, demonstrates collaterals from the SPA to the OphA (arrow) via an ethmoidal branch (double arrows). D, The same image as in C but in the late arterial phase shows the OphA (arrow) and choroidal blush (arrowheads).












Tables
Treatment protocol used at our institution for the embolization of idiopathic posterior epistaxis
Step Action Clarification 1 Angiogram of il* ICA Verify supply to the OphA and choroidal blush from the ICA; rule out an ICA source of bleeding; check for extensive supply to nasal mucosa from the EAs 2 Angiogram of il ECA Rule out vascular anomalies; check for dangerous anastomoses between ECA and ICA; rule out nonidiopathic causes of epistaxis 3 Embolization of il IMA Selective catheterization of IMA, distal to MDTA, and embolization with suspension of PVA particles (250–350 μm) in contrast medium; sometimes followed by 1 or 2 Gelfoam pledgets 4 Embolization of il FA Performed if significant supply to nasal mucosa from FA; selective catheterization of FA, distal to SMA, and embolization with suspension of PVA particles (250–350 μm) in contrast medium 5 Repeat 1–4 on cl* side Due to collaterals between il and cl vasculature, we routinely include the cl side in our protocol 6 Transfer to ENT department The packs are usually removed the following day by the ENT department Note:—il indicates ipsilateral; cl, contralateral; ENT, ear-nose-throat; EAs: ethmoidal arteries (anterior and posterior); ICA, internal carotid artery; OphA, ophthalmic artery; ECA, external carotid artery; IMA, internal maxillary artery; MDTA, middle deep temporal artery; PVA, polyvinyl alcohol; FA, facial artery; SMA, submandibular artery.
* il and cl indicate the side of bleeding or, if the patient bleeds from both nostrils, the side where bleeding started.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Endovascular arterial embolization versus conservative management with nasal packing alone for severe epistaxis: a nationwide cohort study
- Endovascular intervention for the treatment of epistaxis: cone beam CT review of anatomy, collateral, and treatment implications/efficacy
- Endovascular intervention for the treatment of epistaxis: cone beam CT review of anatomy, collateral, and treatment implications/efficacy
- Endovascular Management of Intracranial Dural Arteriovenous Fistulas: Transarterial Approach
- Last resort: case of clot translocation in intra-arterial stroke therapy
- Last resort: case of clot translocation in intra-arterial stroke therapy
- Off-Label Use of Drugs and Devices in the Neuroendovascular Suite
- Current treatment strategies for epistaxis: a multidisciplinary approach
- Severe epistaxis after nasogastric tube insertion requiring arterial embolisation