
Article Figures & Data
Figures
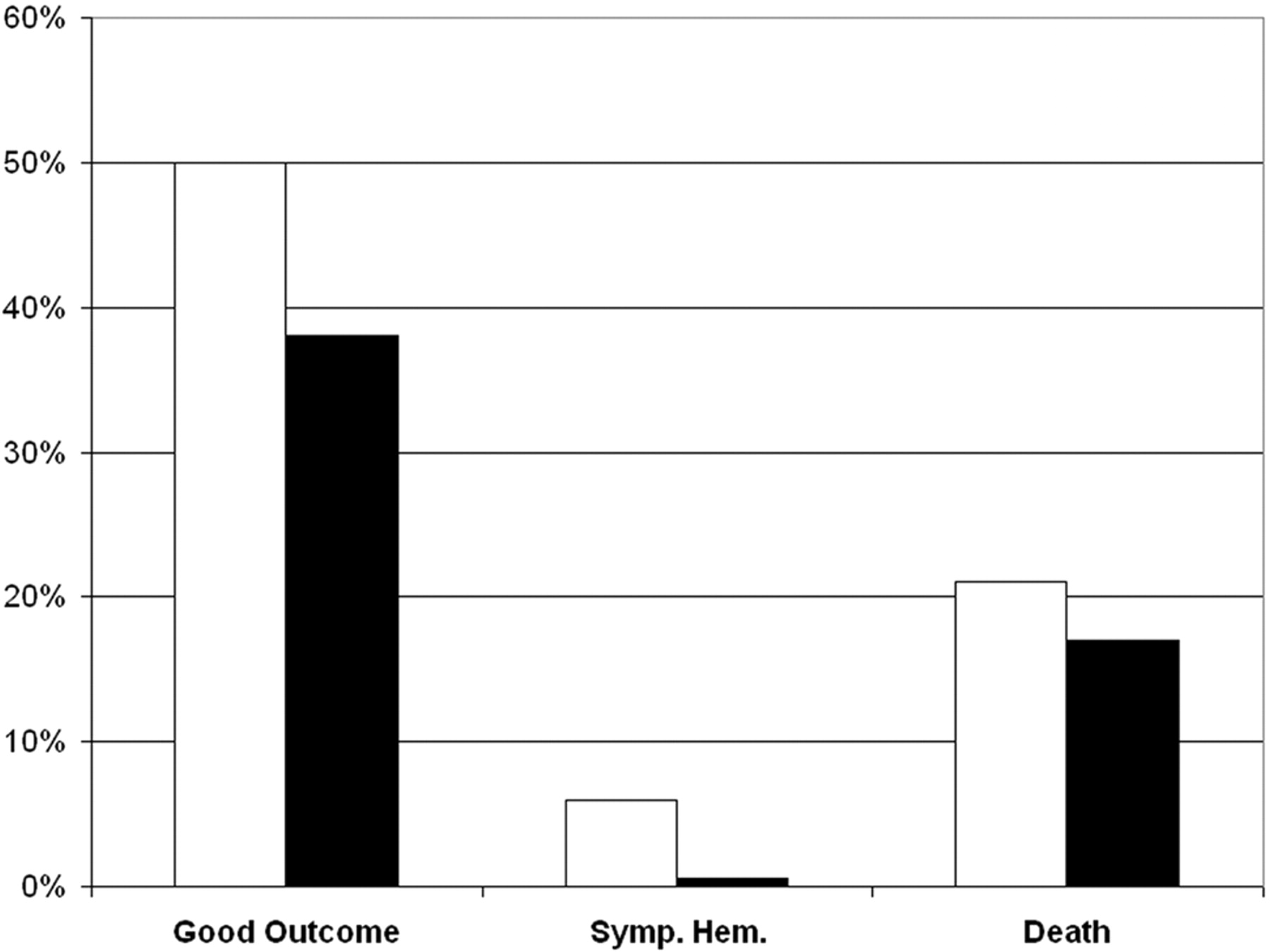
- Fig 1.
Three outcome measures from the NINDS tPA trial.1 In a study population of 624 patients, recombinant tPA (white bar) or placebo (black bar) was administered intravenously in patients within 3 hours of stroke symptom onset and negative findings on head CT. Displayed here are percentages of patients who had good clinical outcomes at 3 months (modified Rankin Score of 0–2), symptomatic hemorrhage, and death. The long-term clinical benefit of tPA was significant (global odds ratio for a favorable outcome, 1.7; 95% confidence interval, 1.2–2.6). Compared with patients given placebo, patients treated with tPA were more likely to have minimal or no disability at 3 months on the assessment scales (50% versus 38%). Symptomatic intracerebral hemorrhage within 36 hours after the onset of stroke occurred in 6.4% of patients given tPA but in only 0.6% of patients given a placebo (P < .001). Mortality rate at 3 months was 17% in the tPA group and 21% in the placebo group (nonsignificant, P = .30).
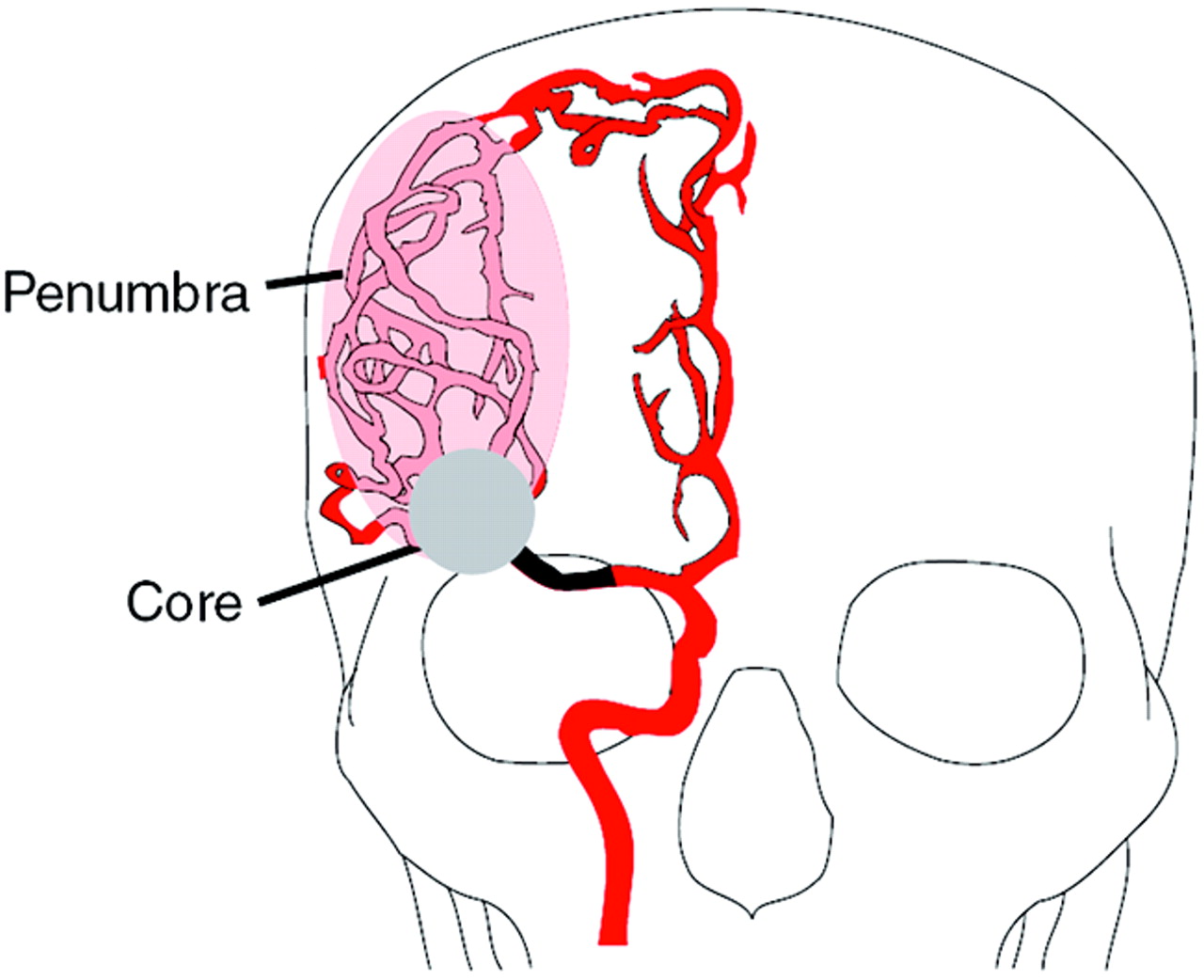
- Fig 2.
The ischemic penumbra. Occlusion of a major cerebral artery such as the proximal right MCA, illustrated here, results in changes in the hemodynamics of the brain that vary from patient to patient. With occlusion, collateral vascular channels can provide blood flow to ischemic regions. Here, collateral circulation from the right anterior cerebral artery distribution to the right MCA territory is depicted. The perfusion within the vascular territory of the occluded artery varies with some areas receiving little blood flow, whereas other areas receive near-normal amounts of blood flow. This results in 2 regions: an infarction core that represents irreversibly injured brain and an ischemic penumbra that may be clinically symptomatic but can be rescued if blood flow is restored.
- Fig 3.
Blood flow and infarction. Data from awake monkeys in which an MCA was occluded.44 The open circles represent local blood flow in normal tissue, the open triangles are measurements in the periphery of the infarct, and the closed rectangles depict blood flow within the infarct. The dashed line approximates the infarction threshold; when the local CBF crosses this line, there is irreversible injury. Local CBF outside this line, but below normal levels (∼20–25 mL/100 g per minute), represents the ischemic penumbra.
- Fig 4.
Outcomes and reperfusion rates in the Desmoteplase in Acute Stroke (DIAS) trial.80 Data from the dose escalation part of this phase II trial are depicted, including reperfusion percentage (open bars) and good clinical outcomes (black bars). Dosage on the horizontal axis is in units of micrograms per kilogram. At the optimal dose (125 μg/kg), the reperfusion percentage (∼70%) and good outcome percentage (∼60%) were much superior to those of a placebo. Remarkably, strong statistical significance was achieved (P = .009), despite small numbers of patients (n = 15 for desmoteplase at the optimal rate and n = 11 for the placebo).
- Fig 5.
Outcomes in extended time window for tPA trial.81 Patients within 0–3 hours from symptom onset (group A, n = 79) were treated according to standard CT criteria. Treatment within 3–6 hours (n = 43) was decided according to protocol criteria that included a diffusion- and perfusion-weighted image–generated TTP map; criteria for tPA treatment were defined as a diffusion/perfusion mismatch >50%. Clinical outcomes for the patients in the 2 groups were not significantly different. Interestingly, more than 75% of the 56 patients considered for inclusion into the 3- to 6-hour group B had a diffusion/perfusion mismatch >50%.
- Fig 6.
Using imaging-derived physiologic information to guide therapy. The patient is a 38-year-old man who was found with a severe left hemiparesis. The precise time of stroke onset was unknown. The noncontrast CT scan was remarkable for a hyperattenuated focus in the region of the right MCA (not shown). A, CT angiography demonstrates occlusion of the right MCA (arrow), but with reconstitution of distal branches likely due to collateral circulation. B, Diffusion MR imaging shows abnormal diffusion in the distribution of the right lenticulostriate arteries, but with sparing of the remainder of the MCA territory, including the cerebral cortex. C, Perfusion MR imaging displays abnormalities involving the entire right MCA territory. The time-to-minimum-perfusion map at the same level as the DWI image demonstrates a perfusion deficit that is much larger than the DWI abnormality. Because of the large diffusion/perfusion mismatch and the likely poor long-term outcome in the absence of treatment in this man with a young family, the decision was made to proceed to intra-arterial thrombolysis. D, Right common carotid angiogram demonstrates a cutoff of the right MCA, corresponding to the previously obtained CTA (arrow). E, After manipulation with a microguidewire and infusion of urokinase, right MCA flow was established (arrow). F, A follow-up head CT scan shows infarction in the region of the right corona radiata and a small portion of cerebral cortex. The patient made an excellent recovery with minor neurologic deficits at discharge.






In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Combined Multimodal Computed Tomography Score Correlates With Futile Recanalization After Thrombectomy in Patients With Acute Stroke
- Time and Diffusion Lesion Size in Major Anterior Circulation Ischemic Strokes
- Role of EPI-FLAIR in Patients with Acute Stroke: A Comparative Analysis with FLAIR
- Imaging-based selection for intra-arterial stroke therapies
- Prediction of Recanalization Trumps Prediction of Tissue Fate: The Penumbra: A Dual-edged Sword
- Computed Tomography Workup of Patients Suspected of Acute Ischemic Stroke: Perfusion Computed Tomography Adds Value Compared With Clinical Evaluation, Noncontrast Computed Tomography, and Computed Tomography Angiogram in Terms of Predicting Outcome
- Does perfusion imaging add value compared with plain parenchymal and vascular imaging?
- Reperfusion by Combined Thrombolysis and Mechanical Thrombectomy in Acute Stroke: Effect of Collateralization, Mismatch, and Time to and Grade of Recanalization on Clinical and Tissue Outcome
- Early Experience of Translating pH-Weighted MRI to Image Human Subjects at 3 Tesla
- Identification of Infarct Core and Penumbra in Acute Stroke Using CT Perfusion Source Images
- Poststroke neuronal rescue and synaptogenesis mediated in vivo by protein kinase C in adult brains