
Abstract
BACKGROUND AND PURPOSE: Pericallosal lipomas are rare tumors. Few reports have included their imaging characteristics. Furthermore, little is known about their evolutive course. Our purpose was to describe the imaging features of seven cases of pericallosal lipoma diagnosed in utero and followed up after birth.
METHODS: We reviewed seven cases of pericallosal lipoma diagnosed by obstetric sonography (n = 7) and examined by fetal MR imaging (n = 5). Analysis of the complementary findings provided by fetal MR imaging was conducted. All findings were correlated with the postnatal imaging and clinical findings.
RESULTS: Obstetric sonography easily showed the pericallosal lipoma in all seven patients. In one, however, it was misinterpreted as intracranial hemorrhage. The morphology and integrity of the underlying corpus callosum were less easy to assess by using sonography. Fetal MR imaging confirmed the fatty content and location of the lesion in all five cases. It showed the choroidal extension in two patients and the type of associated callosal anomaly in another patient better than did sonography. In two patients, the lipoma grew, as revealed by subsequent postnatal MR imaging. The results of the neurologic examinations remained normal for the five surviving patients at a mean follow-up of 3 years (1 month–9 years).
CONCLUSION: Obstetric sonography is able to easily show pericallosal lipoma. Fetal MR imaging may be useful to characterize the lipomatous nature and the extension of the lipoma and the status of the corpus callosum. Long-term follow-up is necessary to understand the clinical consequences of such lesions.
Pericallosal lipoma is a rare anomaly of the CNS found in one of 2500 to one of 25,000 autopsies. It presents with great clinical variability and is frequently associated with anomalies of the corpus callosum. It may be part of specific malformative syndromes (1). With the increasing use of obstetric sonography, a few cases have been detected in utero and reported in the recent literature (2–5). We herein report the sonographic characteristics of seven new cases, discuss the potential use of fetal MR imaging for prenatal evaluation, and stress the need for long-term follow-up to understand the natural history of the malformation.
Methods
Seven cases of fetal pericallosal lipoma were collected from three hospitals in France and Belgium during a 10-year period (1990–1999). The analysis of the cases included in utero and postnatal imaging and neurologic evaluation at birth and at follow-up.
All the sonography findings in utero were reviewed, including the gestational age at diagnosis, the size, morphologic type (as described by Truwit and Barkovitch [6]), and localization of the lipoma, and the associated anomalies. The specific sonographic characteristics of the lipomas (echogenicity, margins, and extensions) were also studied. Pre- and postnatal MR images were analyzed independently by two pediatric neuroradiologists (P.D., F.B.) to assess the lipoma, the degree of callosal anomaly, and any associated anomaly. The clinical and other imaging evaluations conducted at birth and at follow-up were also reviewed.
Obstetric sonography was performed using variable equipment with 3.5- to 5-MHz curvilinear transducers. Fetal MR imaging was performed using 1.5-T systems from two manufacturers (Philips Medical System, Best, The Netherlands; General Electric, Milwaukee, WI). Informed consent was obtained from the parents. The examination was performed after maternal premedication with 1 mg of flunitrazepam administered orally. T2-weighted turbo spin-echo imaging (4000/140 [TR/TE]) and T1-weighted gradient-echo imaging (400/140) were performed in sagittal, axial, and coronal planes.
Results
The data concerning the seven patients are detailed in Table 1. In six cases, the lipoma had a tubulo-nodular pattern (Figs 1A and 2A), and in the last case, case 7, the lipoma had a curvilinear pattern (Fig 3A). Six cases had been discovered during the third trimester (mean gestational age, 32 weeks). The most recent case (case 7) was diagnosed at 23 weeks after the last menstrual period. Lipoma was correctly diagnosed using obstetric sonography in six of the seven cases. In case 5, the anomaly was detected but the diagnosis that had been suggested was intracerebral hemorrhage. In six patients, the lipoma was associated with various anomalies of the corpus callosum (complete agenesis, four patients; partial agenesis, two patients). In case 7, the corpus callosum appeared normal (Fig 3). The extent of the callosal anomaly was correctly established by using sonography in six of seven cases. In case 4, the corpus callosum was not seen.
In utero and postpartum data of seven patients with pericallosal lipoma

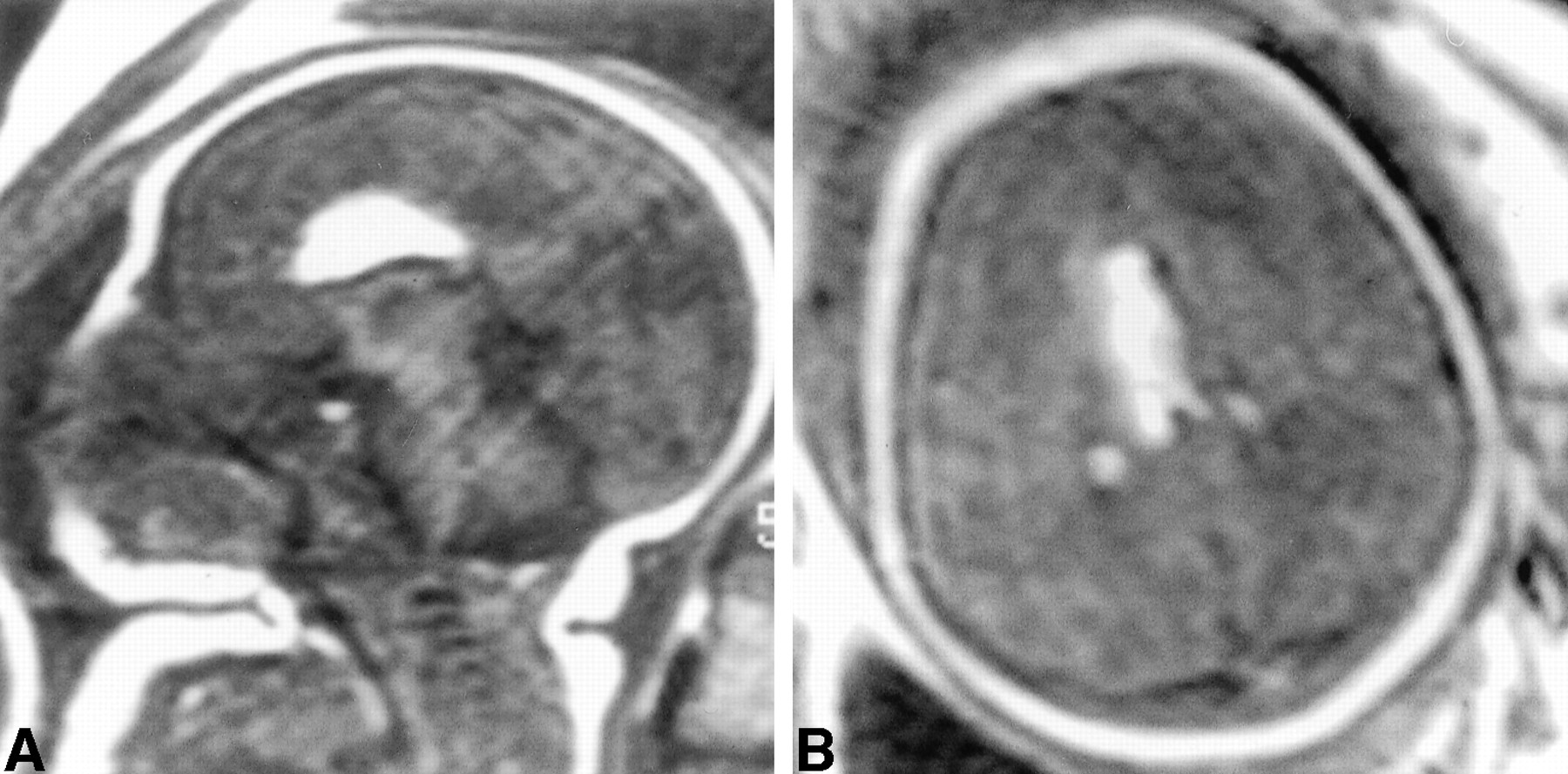
Tubulo-nodular type of pericallosal lipoma. In utero and postnatal follow-up images (case 3).
A, Sonogram obtained in utero at 35 weeks' gestation. A biparietal image is shown. A hyperechoic mass (M) can be seen within the anterior midline. The lipoma appears slightly less echogenic than the parietal bone; its margins are irregular. The mass is extending toward the frontal lobes (arrows).
B, MR image obtained at birth. Sagittal view turbo spin-echo T1-weighted image (350/16/1) confirms the presence of the lipoma and the agenesis of the corpus callosum.
C, MR image obtained at birth. Frontal view turbo spin-echo T1-weighted image (350/16/1) shows the lateral extend of the lipoma.
D, MR image obtained at age 3 years. Mid-sagittal view turbo spin-echo T1-weighted sequence (450/15/1) shows the growth of the lipoma.
E, MR image obtained at age 3 years. Similar findings are revealed by the frontal view turbo spin-echo T1-weighted sequence (450/15/1).

Tubulo-nodular type. Fetal MR images (case 4).
A, Mid-sagittal view turbo spin-echo T1-weighted sequence (400/17/1) shows typical lipoma and incomplete corpus callosum. Note that it was not possible to obtain this sagittal view image by using obstetric sonography.
B, Transverse turbo spin-echo T1-weighted sequence (400/17/1) shows the lipoma and the extension toward the plexus choroids.

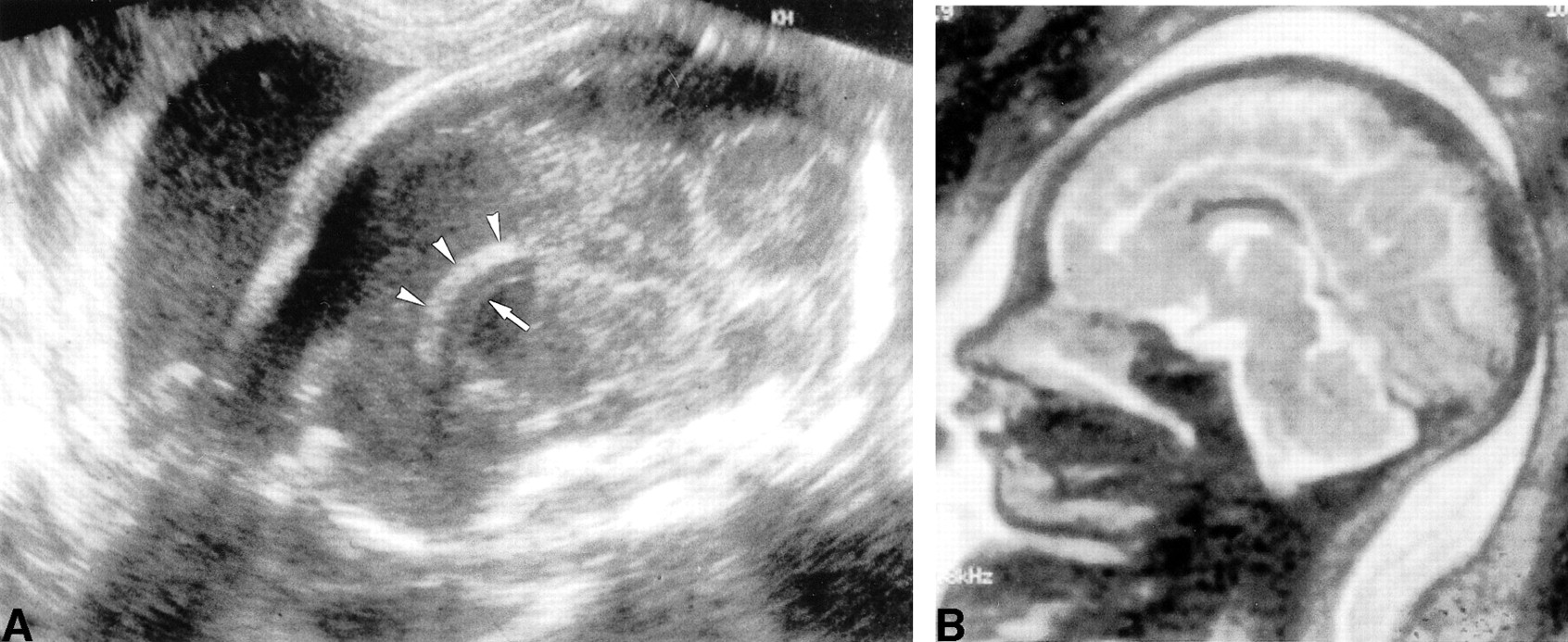
Curvilinear pattern. Sonograms and fetal MR images (case 7).
A, Obstetric sonograms obtained 26.5 weeks. Sagittal view image of the fetal head. The lipoma appears as a hyperechoic mass (arrowheads) with smooth margins parallel to the corpus callosum (arrow).
B, Fetal MR image. Mid-sagittal fast spin-echo T2-weighted sequence (8000/122/2) shows a curvilinear hyposignal lipoma and a normal corpus callosum.
Fetal MR imaging was performed in the five more recent cases. It confirmed the presence of the lipoma and characterized the corpus callosum in all five cases (Fig 3A and B); it showed, better than did sonography, the extension of the lipoma in two patients and the precise type of callosal anomaly in another. Patient 1 had multiple congenital anomalies and died at day 27. The five surviving patients had normal results of their neurologic evaluations at birth. They have been followed up for 1 month to 9 years (mean, 3 years). Their neurologic development remains normal.
Follow-up MR imaging was also performed in patients 2 and 3 at ages 9 and 3 years, respectively. In both cases, the lipoma had increased in volume and extension. In both, less sulci were visible adjacent to the lipoma and the cortical mantle appeared thickened. These features increased on subsequent control images (Fig 1B–E). There was a global agreement between the two reviewers of the MR imaging findings regarding the lipoma, the corpus callosum, and the associated anomalies.
Specific sonographic characteristics of the lipomas are detailed in Table 2. The echogenicity of the lipoma was similar to that of the parietal bone in five patients, less echogenic in one, and more echogenic in one. The margins were smooth in five patients and irregular in the two patients with the largest lipomas. Extension of the lipoma toward the frontal lobes in two patients and toward the choroid plexuses in another was visible.
Specific sonographic characteristics of the pericallosal lipomas
Discussion
The natural history of perinatally diagnosed pericallosal lipoma is unknown. The entity is rarely isolated, and the workup must be as complete as possible to detect all associated malformations. An antenatal diagnosis is very rare, and only a few cases have been reported (2–5). With this article, we add seven cases, including postnatal follow-up, and discuss the contribution of prenatal MR imaging.
The pathogenesis of a pericallosal lipoma is considered to be the result of an abnormal resorption of the meninx primitive. Usually, this resorption occurs between the eighth and the 10th week of development (6, 7). When the meninx primitive persists longer, instead of being resorbed, it differentiates into lipomatous tissue. Such lipoma may develop in all the cerebral cisternae, but they are much more frequent in the area of the corpus callosum where it interferes with its normal growth between the 11th and 20th weeks. Therefore, anomalies of the development of the corpus callosum (complete or partial agenesis, hypoplasia) almost always coexist. The degree of anomaly seems to be in relation with the size and location of the lipoma (6–8). Two morphologic types of pericallosal lipoma have been described on the basis of MR imaging findings in adults and children (1, 6, 7). One is a tubulo-nodular type, appearing round and measuring >2 cm. It is usually anterior and associated with extensive callosal and possibly fronto-facial anomalies. The second type is curvilinear: thin, elongated, measuring <1 cm in diameter and usually more posterior. The corpus callosum is only mildly hypoplastic. The tubulo-nodular type is much more common.
On obstetric sonograms, the lipoma is best visualized on an image obtained slightly above the image that is intended to measure the biparietal diameter. The aspect of a pericallosal lipoma is characteristic: a nodular or curvilinear mass within the interhemispheric fissure. A lipoma is always an echogenic mass. In our series, the echogenicity of the mass was most often similar to that of the parietal bone; it was more echogenic compared with the bone in one patient and less echogenic in another. Larger sized masses tend to have irregular and somewhat spiculated margins. Extension toward the frontal lobes or the choroid plexuses is also a characteristic feature; it was present in three of our patients (4). The differential diagnosis of a lipoma includes hemorrhagic or rare tumoral lesions (such as craniopharyngioma) (3–5). The diagnosis of the pericallosal lipoma is usually performed during the third trimester (at a mean of 32 weeks in our series and 36.5 weeks for the previously reported cases), probably when the mass has a significant volume. The tubulo-nodular type presented by Truwit and Barkovitch (6) is the type most commonly detected. Our last case was a curvilinear type and was detected much earlier, at 23.5 weeks. This is probably because of the growing experience of the sonographers and better equipment.
As noted above, the antenatal monographic diagnosis of callosal anomalies has been frequently reported. However, because of the lipoma, direct visualization of the callosal anomaly in utero may be difficult on sonograms. The indirect signs associated with callosal dysgenesis, such as colpocephaly, are easier to show (9, 10).
There has been a rapidly growing interest for the use of MR imaging for the evaluation of fetal CNS (11, 12). MR imaging completes the information provided by obstetric sonography. In cases of pericallosal lipoma, MR imaging easily confirms and further characterizes the lipoma (location, size, and extension) and the associated anomalies. On fetal MR images, the fatty content of the lipoma is easily seen. Furthermore, in our series, MR imaging more clearly revealed the extension of the lipoma. Another interesting feature of fetal MR imaging is that it accurately displays the associated callosal anomaly. Gyration anomalies may be present and are also better shown by MR imaging (4). In cases 2 and 3, fewer sulci were visible adjacent to the lipoma and the cortical mantle appeared thickened; these features increased on subsequent control images (Fig 1), and it is therefore difficult to determine whether these findings are related to the size of the lipoma or to gyration dysgenesis. No other gyration anomalies were found in our cases.
The neurologic status of patients presenting with pericallosal lipoma seems variable and related to the age of the patients, the type of lipoma, the associated callosal anomalies, and other system malformations (1, 13). Fifty percent of the interhemispheric lipomas are associated with seizures starting in the second decade of life. Mental retardation and psychological disorders may develop later. The tubulo-nodular type of lipoma is more often associated with clinical anomalies than is the curvilinear type. When other anomalies are present (neuronal migration, gyration anomalies), more symptoms are present. A few cases of lipoma have been found in association with Goldenhar syndrome and trisomy 13, 15, 18, and 21 (3, 14, 15). Therefore, chromosomal analysis is mandatory in utero.
The clinical evolution in our series was normal, with a follow-up of 1 month to 9 years (mean, 3 years). However, symptoms may occur later. One unusual finding at follow-up in our series was the relative increase in volume of the lipomas observed in two cases (cases 2 and 3). A similar discussion has occurred regarding intraspinal lipomas that, like intracranial lipomas, are composed of normal fat. Fat cells markedly increase in size during infancy. It has been shown that growth of intraspinal lipoma may parallel the postnatal fatty growth of the patients and that, conversely, a diet leading to a reduction of the body fat may determine a decrease in the size of the spinal lipoma (16, 17). Therefore, it is suggested that patients with intraspinal lipomas be followed up throughout childhood and that their weight be monitored. The same could likely apply to intracranial lipomas; however, this postnatal growth has not been reported until now and our two patients were not overweight. It may be that other growth factors must be implicated (proper to the tumor? genetically determined?) (1, 4). The follow-up of more cases may lead to clarification. The two patients remain asymptomatic, but a longer clinical follow-up will determine the importance of such findings.
Conclusion
Pericallosal lipoma has a typical sonographic pattern in utero. The diagnosis of the tubulo-nodular type is easier than the diagnosis of the curvilinear type. Fetal MR imaging may help for the evaluation of the associated anomalies, especially of the frequent callosal anomaly. The surviving patients in our series had normal results of their neurologic examinations, despite an increasing size in two cases. Longer follow-up is needed.
Footnotes
↵2 Address reprint requests to Fred E. Avni, MD, PhD, University Children's Hospital Queen Fabiola, Avenue J.J. Crocq, 15, B-1020 Brussels, Belgium.
References
- Received June 21, 2000.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.