
Graphical Abstract

SUMMARY:
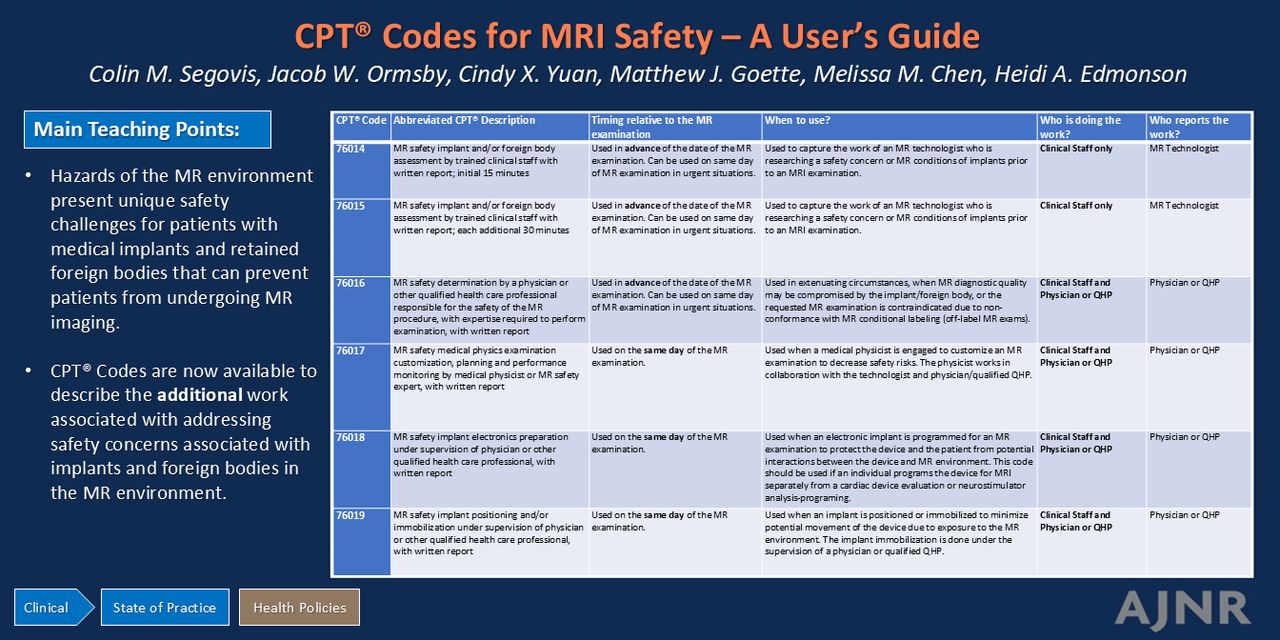
The magnetic fields of the MR environment present unique safety challenges. Medical implants and retained foreign bodies can prevent patients from undergoing MR imaging due to interactions between the magnetic fields of the MR environment and the implant or foreign body. These hazards can be addressed through careful MR safety screening and MR examination customization, often allowing these patients with implants to undergo management-altering MR imaging. However, mitigating these risks takes additional time, expertise, and effort. Effective in 2025, this additional work is formally acknowledged with a new series of Current Procedural Terminology codes to report the work of assessing and addressing safety concerns associated with implants and foreign bodies in the MR environment. This user guide provides guidance on how to report these codes so physician-led MR safety teams can be appropriately reimbursed for the additional work performed in preparing patients with implants or foreign bodies for MR imaging.
ABBREVIATIONS:
- ACR
- American College of Radiology
- ASTM
- American Society for Testing Materials
- CPT
- Current Procedural Terminology
- QHP
- qualified health care professional
MRI is the mainstay technique of neuroimaging. The MR environment, however, presents unique safety challenges because of high-strength magnetic fields. Further, patients with implants can be at increased risk for injury in the MR environment. The US Food and Drug Administration (FDA) recognizes the risks of classifying medical implants as MR safe, MR conditional, or MR unsafe, as designated by the American Society for Testing Materials (ASTM) International, ASTM F2503-23 Standard Practice for Marking Medical Devices and Other Items for Safety in the MR Environment.1⇓-3 The MR safety of implanted medical devices is established by the manufacturer, with validation by the FDA. By default, any device that has not been deemed MR conditional or MR safe is considered MR unsafe. To further complicate matters, the term “MR nonconditional” has also been used in the medical literature to describe cardiac devices that have been labeled “MR unsafe” but may not be completely unsafe in the MR environment.4,5 The labeling provided by the manufacturer is not an absolute contraindication to obtaining an MRI with the guidance of a team knowledgeable in MR safety. Additionally, the number of medical implant technologies and market penetration of active medical implants continues to increase. MR safety is evolving as the field gains experience with implants and foreign bodies. However, the increasing complexity of MR conditional devices along with the time required to assess patient implants, modify medical device settings to meet manufacturers’ MR conditions, and potentially modify MRI protocols to create a safe experience can require more time and effort than associated with the typical MRI, thus creating a challenge for the institution to offer MRI to patients with complex implants or foreign bodies.
Given the evolution of MR safety, the American College of Radiology (ACR) led the Current Procedural Terminology (CPT) code change application, along with the support of American Society of Neuroradiology and other radiology societies, which resulted in the creation of CPT codes that will be available for use in 2025.6,7 These codes allow for billing for the additional work required to perform complex safety assessments for patients at increased risk for harm in the MR environment due to the presence of a medical implant or foreign body. These codes allow for reporting the work required to modify imaging protocols or implants to safely perform MR examinations. These codes describe the work of technologists, medical physicists, physicians, and/or other qualified health care professionals (QHPs). This paper provides guidance on how to use these codes in a neuroradiology practice.
MR SAFETY CPT CODES
The MR safety CPT codes are designed to capture the work associated with specific tasks performed while planning for or performing an MR examination for a patient with an implant or foreign body, which is at high risk of interaction with the MR environment. Specific personnel perform and report these tasks, as described in Supplemental Data. CPT codes capture the work of MR technologists and medical physicists as clinical staff time, which is part of the technical component, while the physician’s work is assigned to the professional component.7 These codes are not meant to report the standard safety screening performed for all patients undergoing MR imaging, which is already included in each MR examination’s reimbursement. Similarly, these codes should not be used for all patients with implants or foreign bodies since not all patients will require the additional work. The MR safety CPT codes should only be used when a safety situation requires extra work by the MR safety team outside of the facility’s routine MR safety workflow, which includes MR conditional implants that may require precautions beyond normal operating mode of the MR system, implants lacking MR conditional labeling, or implants or foreign bodies that are typically contraindicated for MR.
The first 2 CPT codes in this family, 76014 and 76015, are used to report the MR safety assessment associated with an implant or foreign body, typically performed by an MR technologist. These 2 CPT codes are time-based and do not include any physician work. Code 76014 captures the first 15 minutes of work associated with the implant or foreign body assessment. As with all time-based CPT codes, this code can be reported when the midpoint (8 minutes) has passed. Code 76015 is used to report additional time after the initial 15 minutes, but the unit of time changes to 30 minutes. A minimum of 16 additional minutes of work is needed to report 76015 after the first 15 minutes captured with 76014. Code 76015 should not be reported without 76014, and 76015 can be reported up to 3 times for a given case as appropriate. Code 76015 would be expected to be used in scenarios requiring prolonged assessment time, such as with complex, multiple, or incompletely documented implants. These codes are typically used before the date of the MR examination; however, they can be used on the same day in urgent clinical situations. The MR technologist must document the relevant details of any implants and/or foreign bodies, along with the work/time in the medical record to report the codes.
CPT code 76016 is used to report an MR safety determination performed by a radiologist or other MR safety-trained QHP, typically performed before the day of the MRI examination. This code is expected to be reported infrequently, as it is only for clinical scenarios that require a risk-benefit analysis due to unclear MR conditions or when the examination may be contraindicated or limited by the presence of the implant or foreign body but important clinical information could be obtained from an MRI. Code 76016 is most likely performed by a radiologist but is not limited to radiologists. This code can be used on the same day as an MRI examination in urgent clinical scenarios. The code requires written documentation of the clinical scenario, risk-benefit analysis, potential alternate diagnostic tests, and recommendations to mitigate risk should the MR examination remain the chosen diagnostic test. A possible result of the work of 76016 is that the ordered MR examination is not recommended.
The safe performance of MRI in the presence of implants, foreign bodies, or other safety concerns may require work on the day of the MR examination in addition to the work typically associated with MR imaging. Codes 76017, 76018, and 76019 are designed for the additional work associated with these safety activities.
Code 76017 captures the work of customizing the MR protocol to address safety concerns identified during the MR safety assessment. The work is performed by a medical physicist and/or MR safety expert to comply with implant-related MR requirements while maintaining/optimizing diagnostic image quality. This code is not time-based. The work is done in collaboration with the supervising physician or QHP. The work must be documented in the medical record by the physician or QHP; best practice may be to have an independent physics report or cosigned report (by a medical physicist and physician).
Code 76018 is used to report work done by the MR team on the same day as the MRI to prepare implanted electronics for the MRI. Many devices require changing the device to “MRI mode” or programming specific settings per the manufacturer’s instructions. This code is not time-based. This code is separate from a cardiac device interrogation performed by cardiology or a neurostimulation analysis-programming service performed by neurology or neurosurgery and should be reported if the MR staff performs separate device programming. Modification of the settings of the device to minimize interactions between the device and MR environment is performed under the supervision of a qualified physician or QHP supervising the MR examination. Documentation of device modification by the physician or QHP overseeing the MR scan is required.
Code 76019 is used to report the work of positioning and/or immobilizing an implant before MR imaging. This can include the removal of a portion of the device or the immobilization of the device with a physical restraint. An example is the compression-wrapping of cochlear implants before an MRI per the manufacturer’s instructions. Immobilization or positioning of the implant is done on the day of the examination and performed under the supervision of a physician or other QHP. It is best practice to follow the manufacturer’s recommendations, including who the manufacturer suggests should position or immobilize the device. This code is not time-based. Documentation of the work is required by the supervising physician or QHP.
Who Can Use the MR Safety Codes?
The MR safety codes should be used by individuals performing the work described by the codes, which can include MR technologists, MR safety experts, medical physicists, and physicians or QHPs. The personnel of the MR safety team are not defined by CPT. It is best practice to follow guidelines established by expert bodies such as the ACR Manual on MR Safety.2 At a minimum, it is best practice that any individual performing an MR safety procedure is designated as “Level 2 Personnel” for the MRI facility.2 Local and state regulations determine technologists’ qualifications for the operation of an MRI. Supervision rules by a physician or QHP are defined by Centers for Medicare & Medicaid Services (CMS). It is best practice for technologists to be registered as an MR technologist with a recognized credentialing body, such as the American Registry of Radiologic Technologists. Individuals may obtain board certification in MR safety, such as that offered by the American Board of Magnetic Resonance Safety. Board certification as a Magnetic Resonance Safety Officer, Magnetic Resonance Medical Director, or Magnetic Resonance Safety Expert is a best practice, but not required, to use the MR safety CPT codes.
When to Use the MR Safety Code?
All patients must undergo a safety evaluation before MRI because of potential interactions between the high-strength magnetic fields of the MR environment and the patient. The MRI safety CPT codes are for situations when the evaluation associated with a given MRI scan exceeds the typical safety activities associated with MR imaging and should not be used as part of routine MR imaging. The MRI safety CPT codes are applicable to all clinical MR imaging regardless of field strength (eg, 1.5T, 3T, 7T). Example scenarios and coding guidance are meant to be general and are available in the Supplemental Data Table. Individual practice patterns may vary.
| Scenario | Description | Associated Codes |
|---|---|---|
| 1 | MR safety evaluation performed by a technologist in advance of the examination | 76014 |
| 2 | MR safety evaluation performed by a technologist in advance of the examination | 76014, 76015 |
| 3 | MR safety evaluation performed by a technologist and radiologist | 76014, 76016 |
| 4 | MRI safety evaluation performed by a technologist, physicist, radiologist in advance of the examination with examination customization on the day of the examination | 76014, 76015, 76016, 76017 |
| 5 | MR safety evaluation performed by a technologist in advance of the examination and in preparation of implant by the MR team on the day of the examination | 76014, 76018 |
| 6 | MR safety evaluation performed by a technologist in advance of the examination and immobilization of an implant by a qualified provider | 76014, 76015, 76019 |
| 7 | MRI safety evaluation performed by a technologist and radiologist with a “no scan” recommendation | 76014, 76016 |
| 8 | MR safety evaluation performed by a technologist in advance of the examination | No code applicable |
MRI safety scenarios and associated CPT codes described in supplemental material
CONCLUSIONS
The MR safety CPT codes available starting in 2025 represent a recognition of the additional work required to safely perform MR examinations in patients with implants or foreign bodies. Radiologists, physicians, and other QHPs, medical physicists, and MR technologists engaged in MR safety activities will be able to report the extra effort/time needed to keep these patients safe. This paper provides guidance on the use of these new codes from the perspective of neuroradiologists, subject matter experts, and medical physicists engaged in MR safety and reimbursement. The use of these codes should be reserved for the preparation of patients with implants or foreign bodies at high risk for interaction with MR magnetic fields that require additional work beyond the typical MR screening process. These codes are not inherently limited to radiology and can be used by individuals tasked with ensuring patient safety in the MR environment. Documentation in the medical record is required when reporting these codes. Documentation can be a distinct note or part of the diagnostic imaging report, depending on the facility’s reporting workflow. MR imaging should be made available to as many patients as possible. These codes recognize the importance of access to MRI and the additional work required to ensure patients can safely undergo MR imaging.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
Indicates open access to non-subscribers at www.ajnr.org
- Received November 6, 2024.
- Accepted after revision January 11, 2025.
- © 2025 by American Journal of Neuroradiology




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.