
Abstract
BACKGROUND AND PURPOSE: Mechanical thrombectomy (MT) along with emergent carotid stent placement (eCAS) has been suggested to have a greater benefit in patients with tandem lesions (TL), compared with other strategies of treatment. Nonetheless, there is no agreement on whether the intracranial occlusion should be treated before the cervical ICA lesion, or vice versa. In this retrospective multicenter study, we sought to compare clinical and procedural outcomes of the 2 different treatment approaches in patients with TL.
MATERIALS AND METHODS: The prospective databases of 17 comprehensive stroke centers were screened for consecutive patients with TL who received MT and eCAS. Patients were divided in 2 groups based on whether they received MT before eCAS (MT-first approach) or eCAS before MT (eCAS-first approach). Propensity score matching was used to estimate the effect of the retrograde-versus-anterograde approach on procedure-related and clinical outcome measures. These included the modified TICI score 2b-3, other procedure-related parameters and adverse events after the endovascular procedure, and the ordinal distribution of the 90-day mRS scores.
RESULTS: A total of 295 consecutive patients were initially enrolled. Among them, 208 (70%) received MT before eCAS. After propensity score matching, 56 pairs of patients were available for analysis. In the matched population, the MT-first approach resulted in a higher rate of successful intracranial recanalization (91% versus 73% in the eCAS-first approach, P = .025) and a mean shorter groin-to-reperfusion time (72 [SD, 38] minutes versus 93 [SD, 50] minutes in the anterograde approach, P = .017). Despite a higher rate of efficient recanalization in the MT-first group, we did not observe a significant difference regarding the ordinal distribution of the 90-day mRS scores. Rates of procedure-related adverse events and the occurrence of both parenchymal hemorrhage types 1 and 2 were comparable.
CONCLUSIONS: Our study demonstrates that in patients with TL undergoing endovascular treatment, prioritizing the intracranial occlusion is associated with an increased rate of efficient MT and faster recanalization time. However, this strategy does not have an advantage in long-term clinical outcome. Future controlled studies are needed to determine the optimal treatment technique.
ABBREVIATIONS:
- eCAS
- emergent carotid stent placement
- GTR
- groin puncture to recanalization
- IQR
- interquartile range
- IVT
- intravenous thrombolysis
- LVO
- large-vessel occlusion
- MT
- mechanical thrombectomy
- mTICI
- modified TICI
- PSM
- propensity score matching
- SMD
- standardized mean difference
- TL
- tandem lesions
Tandem lesions (TL), defined as high-grade stenosis or occlusion of the cervical ICA and concurrent ipsilateral intracranial occlusion in the anterior circulation, account for 10%–15% of all acute ischemic strokes due to large-vessel occlusion (LVO).1 In most cases the intracranial occlusion involves the MCA.
Data from retrospective studies and registries have suggested that mechanical thrombectomy (MT) of intracranial LVO along with emergent carotid stent placement (eCAS) may have a greater benefit compared with other strategies of treatment.2⇓⇓-5 Nonetheless, in this scenario, there is incomplete agreement on whether it is more appropriate to address the intracranial occlusion with MT as a first step and then treat the ICA lesion with eCAS, or vice versa.6⇓-8 Despite different opinions, both techniques are used and are mainly dependent on the preference of the neurointerventionalist, except for cases in which a highly calcified and severely stenotic ICA lesion requires the initial placement of a stent to facilitate the advancement of large-bore intermediate aspiration catheters into the intracranial vessels. To date, there is no clear indication regarding the more effective timing for the 2 steps of the procedure, and results from previous studies are inconsistent.9⇓⇓-12 It has been shown that prioritizing the intracranial occlusion usually results in shorter groin-to-reperfusion time but not always a more favorable clinical outcome.6,7,12
In this retrospective multicenter study, we sought to compare clinical and procedural outcome measures of the 2 different endovascular treatment strategies in patients with high-grade stenosis or occlusion of the cervical ICA and concurrent ipsilateral MCA occlusion. The analysis was conducted in adherence with the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) statement.
MATERIALS AND METHODS
Patients
The prospective databases of 17 comprehensive stroke centers (15 located in Italy, 1 in France, and 1 in Switzerland) were screened for consecutive patients with TL who received MT and eCAS between January 2016 and June 2023. This work was conducted within the framework of a nonprofit study protocol approved by the ethics committee of the coordinating center. The local ethics committees approved the use of patients’ data.
Demographic data, cardiovascular risk factors, medications at baseline, imaging data, as well as data related to the procedures of the acute phase were collected. All patients were diagnosed with an initial plain CT scan, with determination of the ASPECTS,13 followed by CTA to locate sites of occlusion. TL were defined as a severe stenosis or occlusion of the extracranial ICA and concurrent occlusion of the M1 segment or proximal M2 segment of the MCA, according to the criteria reported in the North American Symptomatic Carotid Endarterectomy Trial (NASCET) and the Thrombectomy in Tandem Lesion (TITAN) trials.14,15 Patients with simultaneous extracranial and intracranial occlusion of the ICA were not considered. Intravenous thrombolysis (IVT) was performed when appropriate and according to current protocols.
Endovascular Procedure
The treatment strategies for TL were defined as eCAS-first, when stent placement of the cervical ICA lesion preceded the treatment of the intracranial occlusion, or MT-first, when treatment of the intracranial occlusion was the initial step of the endovascular procedure. If necessary, balloon dilation was performed before stent placement. All patients received intraprocedural antiplatelet therapy for stent patency immediately before its placement and according to local protocols. MT was conducted using a stent retriever, direct contact aspiration, or a combined technique. The recanalization grade was assessed after a first pass and at the end of the procedure with a dedicated final angiographic run. A score of 2b-3 in the modified TICI (mTICI) scale was the measure of successful recanalization after MT.16 All procedures were conducted with the patient under general anesthesia or local anesthesia/conscious sedation, according to the local protocol or at the discretion of the managing physicians. In each participating center, 2 neuroradiologists with >5 years of experience and blinded to clinical outcome records reviewed all radiologic and angiographic data of their patients. In cases of doubt or disagreement, re-evaluation and adjudication were performed through consultation in a subsequent common session.
Clinical and Radiologic Variables and Measures of Outcome.
Demographic data (age and sex), cardiovascular risk factors, pre-event therapies, and baseline radiologic features were collected. Acute clinical assessment used the NIHSS, whereas long-term clinical outcome was measured with the mRS score acquired at 90 days after stroke, either in person or through a telephone interview by a trained neurologist. The presence of hemorrhagic transformation was assessed by CT or MRI between 24 and 72 hours after the endovascular treatment and defined according to the Heidelberg classification of bleeding events after reperfusion therapies.17
Primary outcome measures were the following: 1) the mTICI score 2b-3 after MT, and 2) the ordinal distribution of the 90-day mRS scores. Secondary outcome measures were the following: 1) rates of mTICI scores 2b, 2c, and 3; 2) time elapsed from groin puncture to recanalization (GTR); 3) procedure-related adverse events that included arterial dissection and embolism in a new territory; 4) stent thrombosis occurring within 24 hours after eCAS; 5) rates of parenchymal hemorrhage types 1 and 2 on follow-up scans; and 6) the 90-day mRS score 0−2.
Statistical Analysis.
Standard descriptive statistics were used to define baseline characteristics. The study population was divided into 2 groups based on the type of endovascular strategy that was adopted (eCAS-first versus MT-first). Differences between categoric variables were compared using the Fisher exact test, whereas continuous variables were compared using the Welch 2-sample t test or the Mann-Whitney U test according to their distribution. The Shapiro-Wilk test was used to test the normality of continuous variables. Missing values were not imputed. The significance threshold was set at P < .05.
Because our patients were not randomized, we used propensity score matching (PSM) to estimate differences in outcome measures between patients subject to the MT-first protocol versus those treated using the eCAS-first strategy. Covariates for PSM included age, baseline NIHSS score, baseline ASPECTS, site of intracranial occlusion (M1 or M2 occlusion), and all other variables that were imbalanced in the univariate analysis of the raw population. The greedy nearest neighbor method was used to create 1:1 pairs of patients who had very similar propensity scores, setting a caliper width of 0.02 on the propensity score scale. PSM balance was assessed by checking standardized mean differences (SMDs) between covariates, with a value <0.1 indicating negligible imbalance.18 The Fisher exact test, Welch 2-sample t test, or the Mann-Whitney U test was used as appropriate to compare outcomes measures between the 2 matched groups of patients.
All analyses were performed using the R software, Version 4.3.2 with cobalt package (https://www.r-project.org).
RESULTS
A total of 295 consecutive patients (88 women, 30%) with TL subjected to MT and eCAS were enrolled. Among these patients, 208 (71%) received the endovascular treatment using the MT-first approach. The 2 treatment groups were homogeneous, except for the rates of atherosclerotic (versus dissection) type lesions of the cervical ICA (86% in the eCAS-first group versus 74% in the MT-first group, P = .022), the median baseline ASPECTS (ASPECTS = 8; interquartile range [IQR], 7−9 in the eCAS-first group versus 7 [IQR, 7−9] in the MT-first group, P = .003), and the use of local anesthesia/conscious sedation (74% in the eCAS-first group versus 46% in the MT-first group, P = <.001) (Table 1). Except for a significantly shorter mean GTR time (77 [SD, 52] minutes in the MT-first group versus 89 [SD, 45] minutes in the eCAS-first group, P = .018), there was no difference between the 2 raw groups concerning rates of efficient recanalization, procedure-related adverse events, rates of parenchymal hemorrhage types 1 and 2, and long-term clinical outcome (Table 2).
Baseline, imaging, and procedural data of the raw population of patients after division for type of endovascular approach
Outcome data of the raw population of patients after division for type of endovascular approach
The PSM algorithm, based on the set of covariates indicated above plus variables that were not balanced in the preliminary analysis (atherosclerotic ICA lesion and type of anesthesia), generated 56 matched couples. The SMD between covariates before and after PSM is shown in the Online Supplemental Data. Univariate analysis of baseline clinical features, pre-event therapies, and procedural data of the matched groups of patients are reported in the Online Supplemental Data.
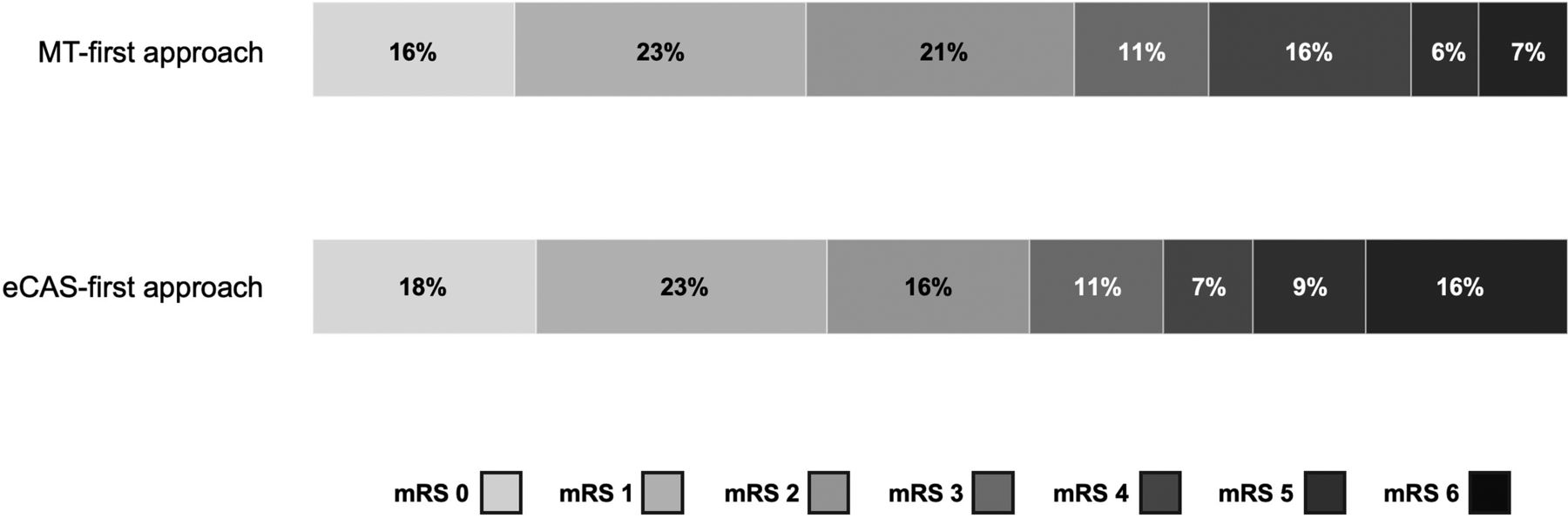
The MT-first approach resulted in a shorter mean GTR time (72 [SD, 38] minutes versus 93 [SD, 50] minutes in the eCAS-first approach, P = .017) and a higher rate of successful intracranial recanalization after MT (rate of mTICI 2b-3 = 91% versus 73% in the eCAS-first approach, P = .025). The difference in rates of successful recanalization was mainly due to a higher proportion of the mTICI grade 2b (30% versus 18%) with similar rates of mTICI 2c and mTICI 3 (25% versus 21% and 36% versus 34%, respectively). There was no difference between the 2 matched groups concerning rates of procedure-related adverse events and occurrence of both parenchymal hemorrhage types 1 and 2. Despite a higher rate of efficient recanalization in the MT-first group, we did not observe significant differences concerning the ordinal distribution of the 90-day mRS scores, the rates of patients with a composite mRS score of 0−2, and mortality of any cause (Table 3 and the Figure).

Ordinal distribution of 90-day mRS scores in patients receiving eCAS-first versus MT-first treatment, after PSM.
Univariate analysis after PSM of clinical and angiographic outcome measures
DISCUSSION
In this multicenter study, we evaluated the effect of the 2 different endovascular strategies for treatment of TL. Our results indicate that the MT-first approach is associated with a higher rate of successful recanalization and a shorter GTR time. However, this evidence does not translate into a more favorable clinical outcome.
Results of previous studies have shown incomplete agreement concerning clinical and procedural outcome measures when the 2 different approaches were compared. In some of them, the MT-first approach was associated with a shorter GTR time, increased rates of successful recanalization, and better clinical outcome.10,19,20 In others, despite a shorter GTR time, there was no significant difference in rates of successful recanalization and favorable clinical outcome between the 2 treatment strategies.6,7,12 Large meta-analyses of retrospective studies have also provided inconsistent results.8,9,11
In real-world practice, there is an operating variability on the acute management of TL, mainly concerning the most appropriate sequence of MT and eCAS and the intraprocedural antiplatelet regimen. Indeed, an international survey has shown that an MT-first approach is preferred by most neurointerventionalists, but still the eCAS-first treatment is adopted in more than one-third of cases.21 Our data on the raw population of patients confirm that the MT-first approach is preferred (71%). Both techniques can offer different advantages on the basis of the patient’s specific needs. The MT-first approach allows a prompter intracranial vessel recanalization, possibly limiting the progression of the ischemic core, but at the same time, it risks re-occlusion due to distal embolization from the untreated ICA lesion. On the other hand, in cases with a severely stenotic or occluded cervical ICA, the eCAS-first approach may be the only feasible treatment strategy, given the difficulty in navigating even the most flexible microcatheters through the atherosclerotic lesion.22,23 In addition to reducing the risk of further embolization or occlusion of intracranial vessels because of a sluggish flow, other advantages of the eCAS-first strategy include the possibility of allowing a better representation of intracranial vessels.5,11,24 Moreover, spontaneous recanalization of the intracranial occlusion following ICA stent placement has been documented in some reports with rates ranging from 6% to 23%.20,25 However, these latter data have not been confirmed by other authors.26
Apart from these considerations, our study on matched cohorts confirms that addressing the intracranial occlusion before the ICA lesion results in shorter GTR time and better MT results. Most important, the rate of embolism in new intracranial territories is not higher than that observed in patients in whom the cervical ICA lesion is addressed as a first step. While it is intuitive that a MT-first approach is associated with a shorter GTR time, there is no clear-cut explanation on why it may also lead to a more efficient recanalization. It has been proposed that a time-dependent change in clot composition, with a progressively increased proportion of fibrin and platelets, results in a less easily retrievable clot when MT is delayed.27 However, it is unlikely that the difference in mean GTR time in favor of the MT-first group will result in a change in clot composition capable of affecting its interaction with the stent retriever. Nonetheless, these data need to be confirmed in forthcoming dedicated studies. On the other hand, in our MT-first matched cohort, better procedural features were not associated with a more favorable clinical outcome. One possible explanation could be that the difference in rates of successful recanalization was mainly due to a higher proportion of the mTICI 2b grade rather than mTICI 2c and 3 in the MT-first group. It is possible that such difference would not be enough to result in a significant difference in clinical outcome, given the limited number of patients after PSM. We also cannot exclude a suboptimal quality of the mRS scores collected in our patients, which may have limited the possibility of detecting differences between groups.
Overall, our results suggest that the more suitable sequence of endovascular treatment for TL should be defined on a case-by-case basis according to the patient-specific vascular characteristics, because procedure-related adverse events are comparable and clinical outcome does not appear to be affected.
The main limitation of our study derives from its retrospective nature and noncontrolled design. Although clinical and procedural records were carefully reviewed, the results could have been affected by the quality of data collected outside the rigid criteria of a randomized trial. For example, we have no information on whether the proximal lesion was treated first due to the inability to pass through the cervical carotid lesion or because of the neurointerventionalist’s preference or other anatomic variations or vessel tortuosity that could have affected procedural and clinical outcome measures. Uncontrolled biases may also derive from the variety of endovascular devices and the type of treatment protocols during the relatively long time of observation. These include, for example, the different use of a balloon-guiding catheter, different first-line MT strategies, and the specific intraprocedural antiplatelet regimens that were adopted. Moreover, the clinical and imaging data provided by individual centers were not assessed by a central core image laboratory, potentially leading to reporting bias in clinical and angiographic outcomes, including rates of successful recanalization. The PSM algorithm applied in our study was centered on a set of covariates that we believe can be relevant for the selected outcome measures, but it is possible that other factors may have been overlooked or missing.
CONCLUSIONS
Our study demonstrates that in patients with TL undergoing endovascular treatment, prioritizing the intracranial occlusion results in faster recanalization time and an increased rate of efficient MT. However, this strategy does not bring a clear advantage when long-term clinical outcome measures are considered and cannot be unequivocally recommended. On the basis of the available data, the sequence of endovascular treatments for TL remains within the judgement of the neurointerventionalist after a case-by-case evaluation of patient characteristics. Future controlled studies are warranted to determine the optimal treatment technique.
Footnotes
Luca Scarcia and Francesca Colò contributed equally to this work.
This work was supported by Ricerca Corrente Reti IRCCS 2022, Rete IRCCS delle Neuroscienze e della Neuroriabilitazione, RIN, Istituto Virtuale Nazionale Malattie Cerebrovascolari x RCR‐2022‐23682294.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received May 14, 2024.
- Accepted after revision July 14, 2024.
- © 2025 by American Journal of Neuroradiology




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.