
Abstract
BACKGROUND AND PURPOSE: A single-aspiration maneuver using a large-volume syringe is a common and effective technique for aspiration thrombectomy. Multiple aspiration cycles using large aspiration syringes have been proposed as a means to improve the efficacy over single aspiration. In this study, we sought to investigate the efficacy of a “triple aspiration technique” in which a large-volume syringe is cycled 3 times before catheter retraction during aspiration thrombectomy.
MATERIALS AND METHODS: A 3D-printed adult vasculature was used as a benchtop thrombectomy platform. Fibrin-rich and red blood cell–rich clots were prepared in centrifuge tubes using human plasma, red blood cells, and calcium chloride. Next, clots were placed in the carotid terminus of the model, and the performances of 3 different aspiration techniques—triple syringe, single syringe, and continuous pump aspiration—were compared in a randomized manner (1:1:1). Outcomes of interest included first-pass efficacy (FPE), complete clot removal (final modified TICI 2c/3), the number of thrombectomy attempts to achieve modified TICI 2c/3, vacuum pressure, and distal embolization. The distal emboli were detected using a 70-μm cell strainer placed at the outflow of the model and quantified using an image-processing algorithm. The vacuum pressures were measured using a pressure transducer.
RESULTS: A total of 102 replicates were performed, 34 for each technique. The triple-aspiration technique provided a significantly higher rate of FPE than the syringe and pump aspiration techniques (67.6% versus 41.1%, P = .02). Additionally, the triple-aspiration technique achieved complete clot removal with a significantly lower mean number of thrombectomy attempts compared with single-syringe aspiration (1.2 [SD, 0.5] versus 1.8 [SD, 0.8], P = .005). The triple-aspiration technique generated significantly higher mean vacuum pressure than both the single-syringe and vacuum pump aspiration (28.3 [SD, 0.2] versus 27.2 [SD, 0.3], P = .002 and 26.2 [SD, 0.4], P = .001, respectively). The differences in complete clot removal and distal embolization parameters were not statistically significantly different across the groups.
CONCLUSIONS: Our findings suggest that the triple aspiration technique can improve FPE rates and vacuum pressure in aspiration thrombectomy. Further studies are needed to examine the safety and efficacy of triple aspiration in the clinical setting.
ABBREVIATIONS:
- AcomA
- anterior communicating artery
- FPE
- first-pass efficacy
- MT
- mechanical thrombectomy
- mTICI
- modified TICI scale
- PcomA
- posterior communicating artery
- RBC
- red blood cell
The development of flexible large-bore catheters with improved trackability has allowed the aspiration thrombectomy to gain widespread recognition among neurointerventionalists. Several clinical trials have established that first-line aspiration is not inferior to stent retriever thrombectomy.1,2 However, the performance of specific aspiration thrombectomy techniques remains largely unexplored.3
In clinical practice, aspiration thrombectomy is generally performed with pump devices or single-syringe aspiration. Several studies indicate that these 2 aspiration techniques are similar and might be open to improvement.4⇓⇓–7 Current data suggest that greater aspiration force and vacuum pressure are correlated with improved recanalization and lower rates of distal emboli.8⇓⇓–11 Therefore, many groups have aimed to use mechanical thrombectomy (MT) techniques that can enhance these parameters during aspiration and, consequently, improve clinical outcomes.
In this study, we introduce a novel aspiration thrombectomy technique called “triple-aspiration,” aiming to enhance vacuum pressure through repeat syringe aspirations in a single pass. This user-friendly approach does not require a special pump system, is cost-effective, and presents theoretic advantages such as greater vacuum pressure and better clot engagement. However, the question of whether these theoretic advantages translate into actual efficacy remains unanswered. Therefore, in this study, we aimed to evaluate the performance of triple aspiration and compare it with conventional aspiration thrombectomy methods, including syringe and pump aspiration.
MATERIALS AND METHODS
Triple-Aspiration Technique and Control Groups
We tested the performance of 3 different aspiration techniques: triple aspiration, single-syringe aspiration, and vacuum pump aspiration.
For the triple-aspiration technique, a 3-way stopcock was connected to a 60-mL aspiration syringe (Vaclok; Merit Medical Systems) and an aspiration catheter (6F Sofia; MicroVention). With the stopcock open to both the 60-mL syringe and the aspiration catheter, the syringe was fully pulled back, and the first aspiration was performed. Then, the stopcock was immediately closed to the aspiration catheter, and any air within the syringe was expelled through the open side port of the 3-way stopcock. Next, the system was closed to the sideport, and a second aspiration was performed using the 60-mL syringe. Then, by means of the same process, any remaining air was expelled through the side port, and subsequently, the third aspiration was performed. We waited for at least 2 minutes after the third aspiration to ensure standardization across all treatment arms, and then the aspiration catheter was removed with the syringe remaining locked. The technique is also demonstrated in a video (Online Supplemental Data).
The single-syringe aspiration was also performed using the 60-mL Vaclok syringe. For the pump aspiration, we used the Riptide vacuum pump (Medtronic). The Riptide pump was set to the highest vacuum pressure achievable after the pressure gauge integrated in the pump reached the plateau, and aspiration was continued for at least 2 minutes for both techniques.
3D-Printed Neurovascular Model
The manufacturing process of the 3D-printed in vitro thrombectomy model has been described by Li et al.12 Briefly, the head and neck arterial vasculature of patients with acute large-vessel occlusion was extracted from anonymized CT angiographies and refined for 3D-printing using the Meshmixer software (Autodesk). Then, the model was 3D-printed using a commercially available resin and printer (Elastic 50A, Form 3 SLA Printer; Formlabs). The elastic 50A resin was specifically chosen because it exhibits a Young Modulus of 1.7 megapascal, mimicking the elasticity of arterial vasculature.
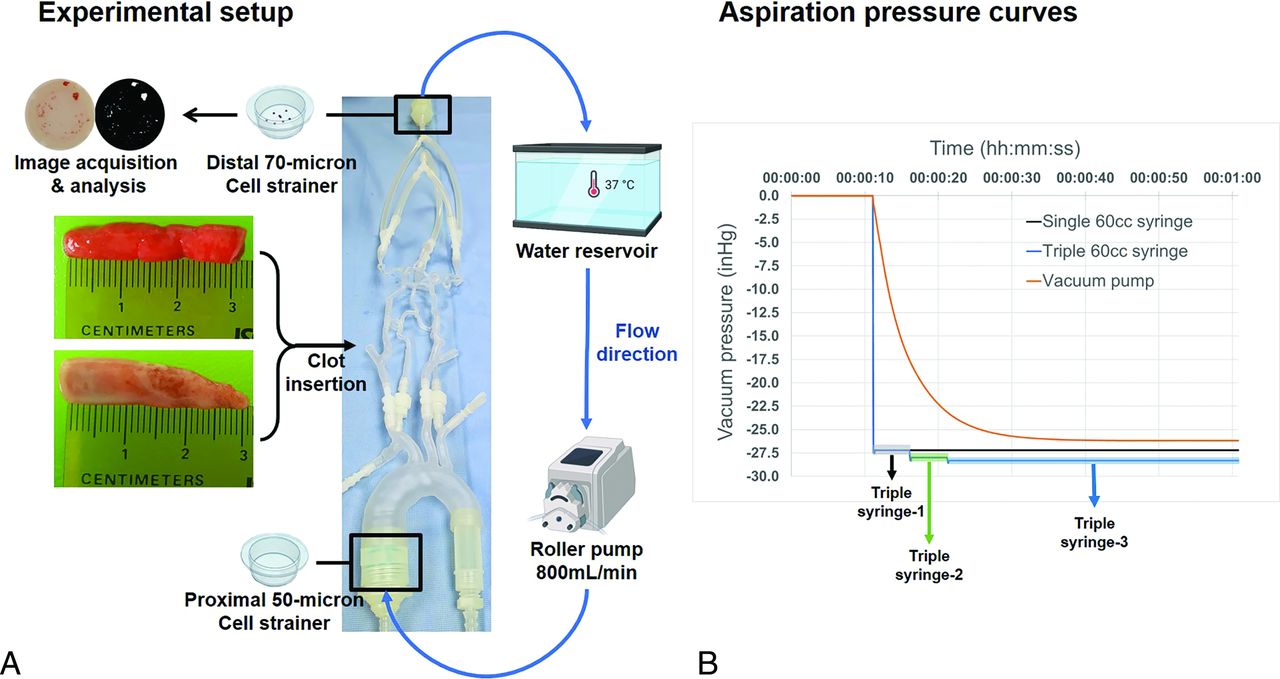
The 3D-printed model had bifurcation MCA anatomy bilaterally and patent anterior (AcomA) and posterior communicating (PcomA) arteries. It included an aortic arch, bilateral carotid arteries (ICA), MCAs (up to 2 distal M2 MCA branches), anterior cerebral arteries (up to the proximal A2 segment), AcomA, PcomA, and posterior cerebral arteries (up to the proximal P2 posterior cerebral artery segments). To mimic transfemoral access, we connected a silicone tubing to the aortic arch, and an 8F introducer sheath was placed into the silicone tubing. Additionally, 2 filters with a 50- and 70-µm pore size were placed at the inflow and outflow of the model for particle filtering and collection purposes, respectively. The 3D-printed model and thrombectomy setup are summarized in Fig 1A.

Experimental thrombectomy setup (A) and aspiration pressure curves (B).
Clot Analogs and Thrombectomy Setup
The performances of aspiration thrombectomy techniques were tested with soft (red blood cell [RBC-rich]) and stiff (fibrin-rich) clot analogs. The RBC and fresh frozen plasma donations were obtained from the Mayo Clinic Blood Transfusion Service. The RBC-rich clots consisted of 16-mL RBC, 32-mL fresh frozen plasma, and 2 mL of 5% calcium chloride (Sigma-Aldrich), and fibrin-rich clots consisted of 47.5 mL of fresh frozen plasma, 0.5 mL of RBC, and 2 mL of 5% calcium chloride. Clot volumes and diameters were standardized to maintain consistency among the replicates. Blood components were put into 50-mL tubes and were mixed by inversion. Then, clot analogs were formed overnight at room temperature. The next day, all clot analogs were cut in 30-mm segments using a 3D-printed rectangular prism with a lumen to ensure standardization across replicates. Subsequently, the clot analogs were measured using a scale, and those significantly smaller or larger than 3 cm were excluded. Next, clot analogs were lodged into the terminus of the right ICA in dynamic flow conditions. Then, clots were measured again, and any outliers were discarded. Fragmented clots and clots that have embolized beyond the terminal ICA were removed from the circulation and not included in the analysis. Following proper occlusion, experiments were randomized into 1 of the 3 treatment arms (ratio 1:1:1), ensuring an equal distribution of stiff and soft clots (ratio 1:1) within each arm. After embolization, the lengths of the clots inside the model were also recorded, and the normal distribution of clot lengths across groups was ensured.
A roller pump was used to circulate approximately 800 mL/min of 37°C water within the model. A 6F FUBUKI guiding catheter (Asahi Intecc Medical) was placed in the right proximal ICA. Then, an aspiration catheter (6F Sofia) was advanced to the occlusion site with the help of a 0.027-inch microcatheter and 0.014-inch micro guidewire. Clots were not passed with the microcatheter or the Micro Guidewire during catheter navigation to avoid introducing distal emboli to the system. After reaching the occlusion site, the microcatheter and micro guidewire were removed, and contract aspiration was performed for at least 2 minutes as described above. Thirty-four replicates (17 RBC-rich and 17 fibrin-rich) were performed for each aspiration technique.
Technical Outcomes, Vacuum Pressures, and Analysis of Distal Emboli
Study end points were complete clot removal, first-pass efficacy (FPE), the number of thrombectomy attempts, vacuum pressure, and distal embolization. Because microscopic clot fragments might be missed during the experiment, complete clot removal was considered analogous to a modified TICI (mTICI) scale score of ≥2c. Because the distinction between mTICI 2a and 2b may not be reliable in an in vitro model, complete clot removal was chosen as the primary recanalization end point. Up to 3 thrombectomy attempts were performed to achieve complete clot removal. FPE was defined as the ability of the aspiration technique to achieve complete clot removal after the first attempt (mTICI 2c/3).
To measure the generated vacuum pressures, we connected the aspiration tubing of the vacuum pump or the 60-mL syringe to a pressure transducer (Model ASDXRRX015PDAA5; Honeywell) and replicated the aspiration approaches described previously. We acquired 5 measurements for each approach, and the pressure data are presented as the mean (SD).
To evaluate distal embolization, we placed a 70-μm cell strainer at the outflow of the model distal to the intracranial vasculature for each replicate. After each experiment, the cell strainer was removed, and the distal embolization was analyzed using an image-processing algorithm, as described by Li et al.12 The algorithm provided the following data: the total count of emboli of >70 μm, the Feret diameter of the largest embolus, the mean Feret diameter of the emboli, the total count of emboli of >1 mm, and the total area of emboli.
Statistics
Statistical analyses were conducted with a statistical software package (SPSS, Version 25.0 for Windows; IBM). The Shapiro-Wilk test was used to examine the distribution of the data. A 1-way ANOVA test and Tukey post hoc analysis were used to examine the differences in normally distributed continuous data. The Kruskal-Wallis test was used for non-normally distributed continuous data. The χ2 and Fisher-Freeman-Halton tests were used for categoric data collected in the benchtop thrombectomy model. For all statistical tests, a P value < .05 was considered statistically significant.
RESULTS
A total of 102 replicates were performed, 34 for each aspiration technique. Mean clot length within the 3D-printed model was 27 (SD, 3) mm without a significant difference across groups (P value = .96). The triple-aspiration technique provided a significantly higher rate of FPE than the syringe and pump aspiration techniques (67.6% [23/34] versus 41.1% [14/34], P = .02). Additionally, the triple-aspiration technique achieved final mTICI 2c/3 recanalization with a significantly lower mean number of thrombectomy attempts compared with single-syringe aspiration (1.2 [SD, 0.5] versus 1.8 [SD, 0.8], P = .005). However, the difference between the triple aspiration and pump aspiration groups was not statistically significant (1.2 ± 0.5 vs. 1.5 ± 0.6, P = .07). The final mTICI 2c/3 rate for the triple- and syringe-aspiration techniques was 85.3%, which was higher than that for pump aspiration (67.6%). Nonetheless, the differences in final mTICI 2c/3 rates were not statistically significant across the groups. The mean total counts of emboli were 25.9 (SD, 19.91) for triple aspiration, 32 (SD, 18.9) for single-syringe aspiration, and 32.3 (SD, 23.9) for pump aspiration, with no statistically significant differences in distal emboli parameters based on aspiration techniques. However, overall, the soft clots were associated with a significantly higher mean total count of emboli (39.1 [SD, 23.4] versus 22 [SD, 14], respectively, P < .001) and a greater mean total emboli area (1.4 [SD, 3.6] mm2 versus 0.3 [SD, 0.3] mm2 respectively, P = .01) compared with the stiff clots. There were no statistically significant differences between soft and stiff clots in terms of mean maximum Feret diameter (0.8 [SD, 0.6] versus 0.6 [SD, 0.3], respectively, P = .22), mean Feret diameter (0.19 [SD, 0.1] versus 0.17 [SD, 0.02], respectively, P = .72), or the mean count of emboli of >1 mm (0.6 [SD, 1.9] versus 0.2 [SD, 0.4], respectively, P = .41). The recanalization and distal embolization outcomes are summarized in Table 1.
Recanalization and distal embolization outcomes
The triple-aspiration technique generated significantly higher mean vacuum pressure than both the single-syringe and vacuum pump aspiration (28.3 [SD, 0.2] inHg versus 27.2 [SD, 0.3], inHg P = .002 and 26.2 [SD, 0.4], P = .001, respectively). The single-syringe aspiration also provided significantly higher mean vacuum pressure than pump aspiration (27.2 [SD, 0.3] inHg versus 26.2 [SD, 0.4] inHg, P = .004). The vacuum pressure outcomes are summarized in Table 2 and Fig 1B.
Vacuum pressures with different aspiration techniques
DISCUSSION
Our study identified several important findings. First, triple aspiration provided significantly higher vacuum pressure and FPE rates compared with single-syringe and pump aspiration. Second, the total number of thrombectomy attempts was also lower with the triple-aspiration technique than with the single-syringe aspiration. Third, triple-aspiration technique was not associated with an increased risk of distal embolization. These findings are important because they suggest that the triple-aspiration technique can generate more vacuum pressure than the conventional techniques and might improve certain recanalization outcomes with aspiration thrombectomy.
Increased vacuum pressure enhances both aspiration and flow rates through the catheter. Considering the viscoelastic properties of clots, force and flow rates are crucial factors influencing clot engagement, facilitating the overcoming of clot adhesion to vessel walls and static friction. Although the theoretic benefits of high vacuum pressure are well-established, the question of how much vacuum pressure is needed for effective aspiration thrombectomy has not been thoroughly investigated thus far. A benchtop study by Gross et al13 found that single-syringe aspiration might generate more vacuum pressure than pump devices. In line with previous literature, single-syringe aspiration provided higher vacuum pressure than pump aspiration in our study. Nevertheless, triple aspiration generated significantly higher vacuum pressure than both aspiration techniques. In our thrombectomy setup using a catheter with a 0.070-inch inner diameter and 115-cm length, a 1-unit increase in pressure (units of mercury) theoretically led to a flow rate increase of 43 mL/min and a force increase of 9.5 mN. Therefore, triple aspiration allowed a catheter with an 0.070-inch inner diameter to achieve a theoretic performance comparable with that of a 0.071-inch inner diameter catheter used with a pump. Most important, empirical evidence supported this hypothesis; the higher vacuum pressure translated into improved efficacy, with triple aspiration providing a significantly higher FPE rate than that achieved with conventional techniques. Multiple previous studies have reported the influence of FPE on clinical outcomes following MT.14⇓–16 In these studies, FPE was associated with favorable outcomes, a low risk of hemorrhagic transformation, and a short procedural time.14⇓–16 Therefore, the triple-aspiration technique can potentially improve outcomes in aspiration thrombectomy. Additionally, triple aspiration achieved complete clot removal with a significantly lower number of thrombectomy attempts compared with the single-syringe technique. Thus, it could also theoretically limit the vascular trauma associated with repeat thrombectomy attempts. However, further studies are necessary to evaluate the efficacy of triple aspiration in a clinical setting.
Clot fragmentation and distal embolization have been associated with unfavorable outcomes following MT.17 Depending on the size and stiffness of the clot, aspiration catheters often engage only the proximal portion of the clot instead of capturing it uniformly. Therefore, during the aspiration attempt, clot fragmentation might occur, particularly if the suction is applied unevenly or if the clot is friable. For this reason, despite the Contact Aspiration versus Stent Retriever for Successful Revascularization (ASTER) and A Direct Aspiration First Pass Technique (COMPASS) trials not finding a significant difference in distal embolization rates between aspiration and stent-retriever thrombectomy,1,2 distal embolization remains a major concern with modern aspiration-based techniques.18 Therefore, distal embolization rates of different aspiration thrombectomy techniques have been a topic of interest. In our study, triple aspiration resulted in a lower total embolus count than other techniques. However, the differences in distal embolization parameters, including the total emboli count, were not statistically significant across groups.
Modified syringe aspiration techniques have been a topic of interest. In 2018, Nikoubashman et al19 introduced a modified aspiration method using two 60-mL VacloK syringes simultaneously. In this technique, the syringes are connected to a 3-way valve, and both are set to open to the aspiration catheter at the initiation of the thrombectomy maneuver. There are 2 notable differences between this method and the triple-aspiration technique. First, the triple-aspiration technique produces higher aspiration pressure compared with the double-aspiration method (Table 2). Second, the triple-aspiration technique facilitates a gradual increase in aspiration pressure with 3 consecutive attempts. In contrast, the double-aspiration method applies the aspiration pressure from 2 syringes to the clot-catheter interface immediately after the 3-way valve is opened.19 Additionally, recently, Froehler10 and Froehler and Good20 proposed another technique known as the plunger technique, which involves manual cyclic aspiration by releasing and pulling back the syringe plunger. Unlike the triple-aspiration technique and the method of Nikoubashman et al, the plunger technique does not aim to increase aspiration pressure but rather to enhance clot engagement and ingestion through manual cyclic aspiration. A recent study by Jablonska et al21 demonstrated that cyclic aspiration with a pump device results in significantly greater clot weight loss than single-syringe aspiration, depending on cyclic aspiration frequency, despite static aspiration generating higher absolute vacuum pressure.22 While it remains unexplored whether these efficient cyclic aspiration frequencies can be imitated without a pump device, early benchtop studies support the efficacy of the syringe-based plunger technique.23 All 3 techniques aim to improve outcomes in aspiration thrombectomy and may offer distinct advantages in clinical settings based on the characteristics of the clot. Further comparative studies are necessary to determine the safety and efficacy of these techniques.
Our study has several limitations. First, performances of different aspiration techniques might change in a real-world setting. Second, in our study, we compared the recanalization outcomes and vacuum pressures of different aspiration techniques. We were unable to provide comprehensive results on safety outcomes beyond distal embolization. Third, although recanalization and neurologic outcomes are interconnected, the clinical benefits of triple aspiration remain unknown. Last, in our study, we used only the Sofia 6F aspiration catheter and the Riptide aspiration pump. The performance of triple-, single-, and pump-aspiration approaches might differ with other aspiration systems.
CONCLUSIONS
The performance of different aspiration techniques remains largely unexplored in the golden era of MT. Our study indicates that the triple-aspiration technique might improve outcomes in aspiration thrombectomy. However, further large-scale studies are needed to establish the performance of triple aspiration in the clinical setting.
Footnotes
C. Bilgin and J. Li contributed equally to this work.
R. Kadirvel received research support from Cerenovus Inc, Medtronic, Endovascular Engineering, Frontier Bio, Sensome Inc, Endomimetics, Ancure LLC, Neurogami Medical, MIVI Biosciences, Monarch Biosciences, Stryker, Conway Medical, Piraeus Medical, and Bionaut Labs. W. Brinjikji holds equity in Nested Knowledge, Superior Medical Experts, Piraeus Medical, Sonoris Medical, and MIVI Neurosciences. He receives royalties from Medtronic; consulting fees from Medtronic, Stryker, Imperative Care, MicroVention, MIVI Neurosciences, Cerenovus, Asahi, and Balt. He serves in a leadership or fiduciary role for MIVI Neurosciences, Marblehead Medical LLC, Interventional Neuroradiology (editor-in-chief), Piraeus Medical, and World Federation of Interventional and Therapeutic Neuroradiology. D.F. Kallmes holds equity in Nested Knowledge, Superior Medical Experts, Conway Medical, Marblehead Medical, and Piraeus Medical; he received grant support from MicroVention, Medtronic, Neurogami, Cerenovus, Brainomix, MIVI Neurosciences, Stryker, Balt, and Insera Therapeutics and has served on the Data Safety Monitoring Board for Vesalio and NoNo Inc. He received royalties from Medtronic. A.A. Oliver is supported by American Heart Association grant No. 23PRE1012781. The remaining authors report no conflicts of interest.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received March 18, 2024.
- Accepted after revision July 7, 2024.
- © 2025 by American Journal of Neuroradiology




{kind=link}