
Article Figures & Data
Figures
- FIG 1.
IDH2-mutated SNUC. A large, infiltrative sinonasal mass with homogeneous, mild T2 hyperintensity (A), avid contrast enhancement, and erosion of the skull base with intracranial extension (B). A large intratumoral cyst (B, arrow) with enhancement of the cyst walls. Radiographic differentials included SNUC and olfactory neuroblastoma. Histopathology shows sheet-like and nested growth of cells with hyperchromatic nuclei, with diffuse positivity on cytokeratin (Oscar) stain (C) distinguishing carcinomas (like SNUC) from nonepithelial malignancies. Immunohistochemistry for IDH1/2 (D) shows strong and diffuse granular cytoplasmic staining, confirming an IDH-mutation.
- FIG 2.
DICER1-mutant tumors. Nasal chondromesenchymal hamartomas with pathogenic germline variation in DICER1 presenting with extensive soft-tissue “masses” in the frontal and ethmoid sinuses involving the anterior skull base with calcific/ossific bodies within the matrix (A and B, arrows). Embryonal bladder rhabdomyosarcoma in the same patient, which is also one of the hallmark tumors associated with a DICER mutation. Bladder rhabdomyosarcoma is seen as a heterogeneous, solid, avidly-enhancing mass within the bladder lumen (C, arrow). Multiple thin-walled pulmonary cysts (D, arrow) with tiny septal nodules are indeterminate but may represent type Ir (regressed) pleuropulmonary blastomas in the setting of the DICER1 mutation. The histopathology of a bladder lesion reveals embryonal rhabdomyosarcoma with diffuse anaplasia (E) and extensive cartilaginous differentiation and diffusely positive staining for desmin (muscle marker) (F).
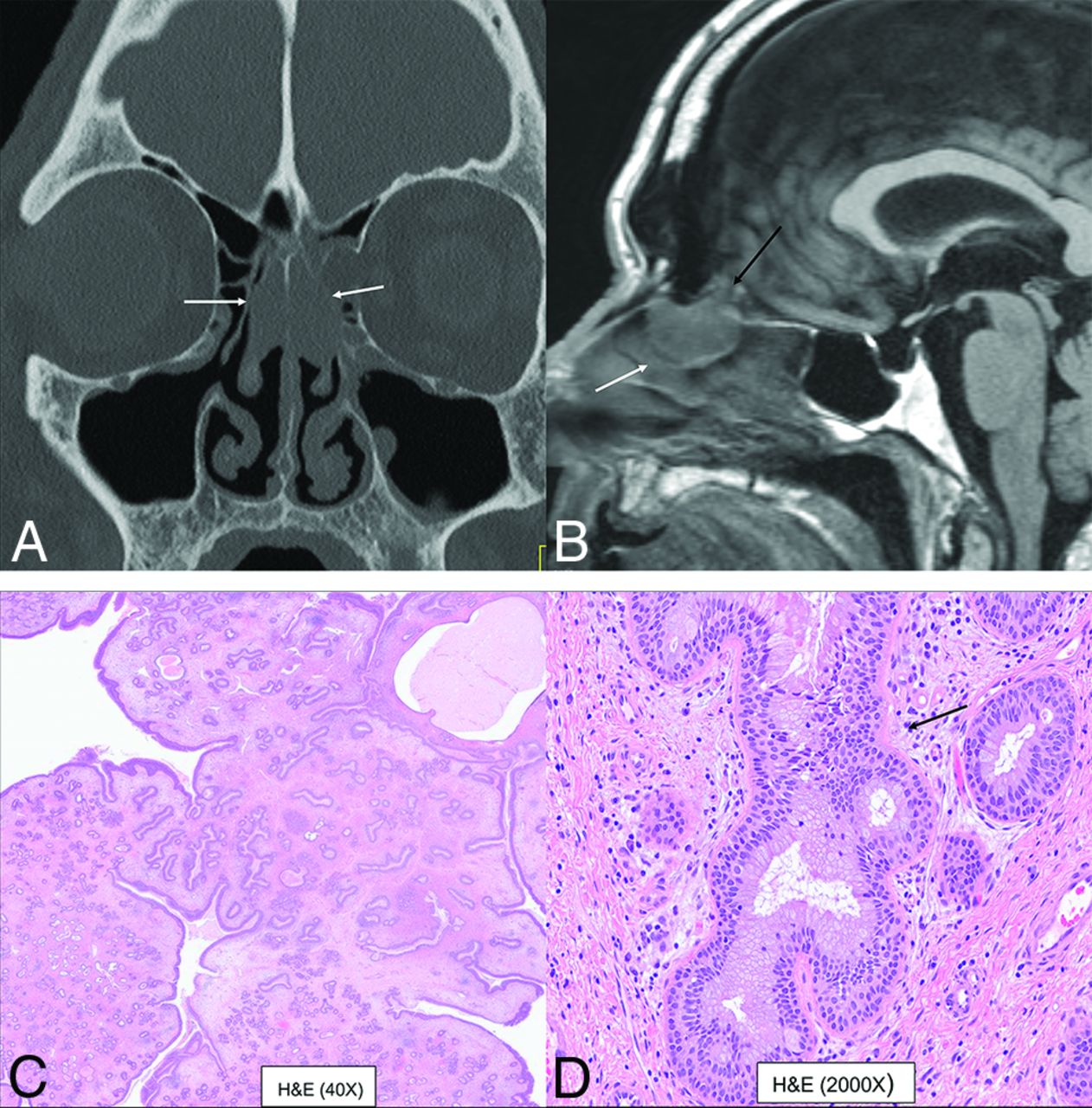
- FIG 3.
Bilateral REAH. Smooth polypoid lesions noted within the nasal cavity bilaterally (A and B, white arrows). The lesion expands the olfactory cleft (B, black arrow) with smooth remodeling, without erosive changes. This cannot be differentiated from seromucinous hamartoma with both exhibiting a crescentic (half-moon) shape on sagittal images (B). Histopathology revealed prominent glandular structures of varying sizes (C). Glands are lined with ciliated respiratory epithelium with bland nuclei and mucinous gland metaplasia (D, black arrow).
- FIG 4.
Sinonasal papilloma, oncocytic type, in the left frontal sinus in a 78-year-old man. Smooth polypoid lesions are noted within the nasal cavity with intrinsic T1 hyperintensity (A, arrow). The lesions obstruct the frontoethmoidal recess with trapped proteinaceous content in the frontal sinus. Lesions show a “cerebriform” pattern on the T2-weighted image (B, arrow) with avid enhancement (C, arrow). Histopathology reveals characteristic oncocytic cuboidal-to-columnar cells and intraepithelial microcysts with mucin and/or neutrophilic microabscesses (D, black arrows).
- FIG 5.
NUT sinonasal carcinoma in a 22-year-old man. Left nasal cavity mass (A and B, white arrows) with hyperostosis of the septum (black arrows). Metastatic disease with lesions in the lymph nodes, liver, and lung (C, white arrows). H&E stain (D) shows sheets and nests of high-grade tumor cells with zones of tumor necrosis. The tumor exhibits positive staining on NUT immunohistochemistry (E) with preserved INI1 staining (F) (ruling out SMARCB1 deficiency). Genetic analysis revealed NUT-BRD4 fusion, the defining feature of NUT carcinomas.
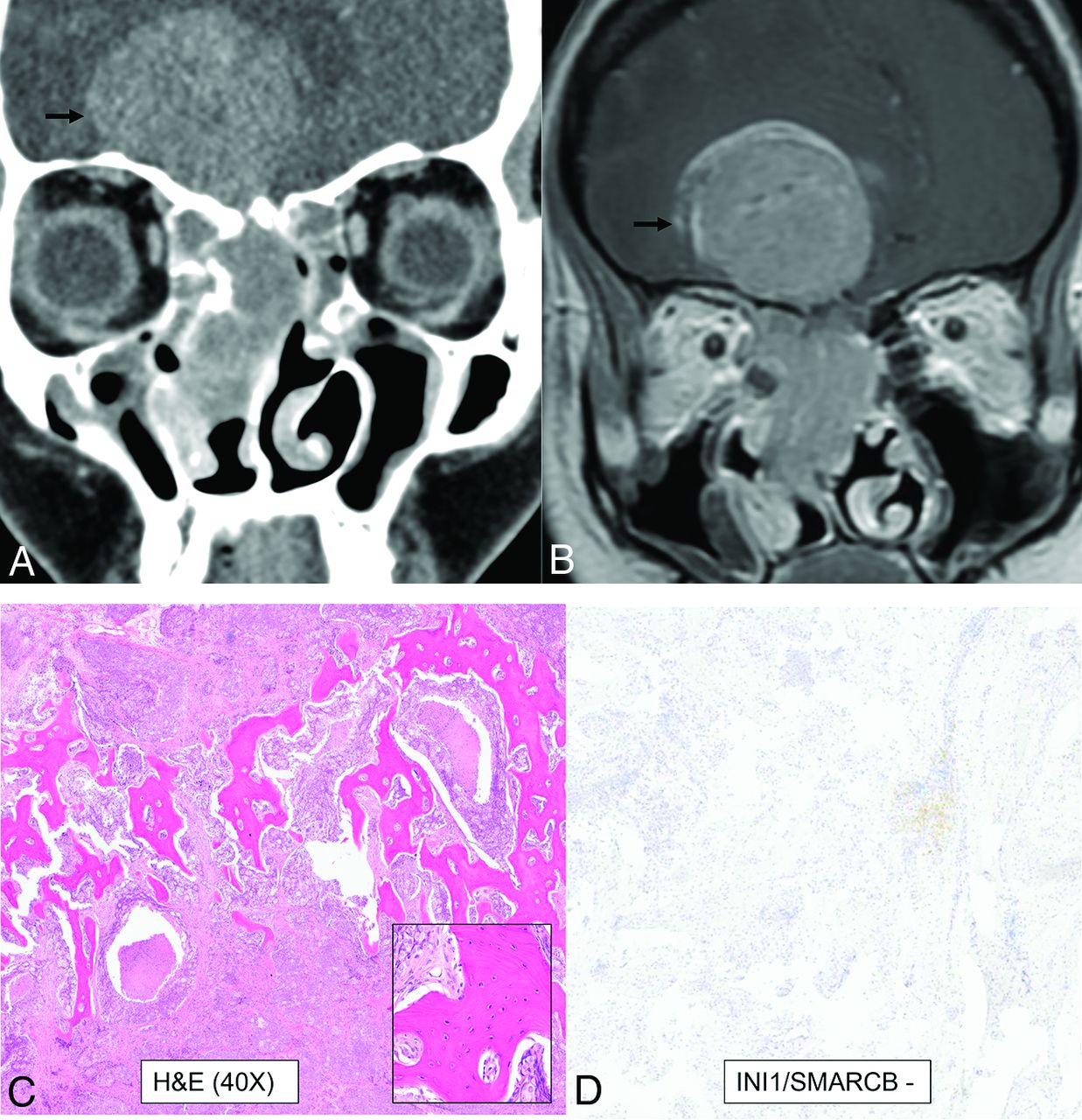
- FIG 6.
SWI/SNF complex–deficient sinonasal carcinoma in a 30-year-old woman. A large infiltrative sinonasal mass with intracranial extension (A and B, black arrows) and marked peritumoral edema in the frontal lobes. Peritumoral cysts were noted in the intracranial component. Radiologic differentials included olfactory neuroblastoma, SNUC, SWI/SNF complex–deficient (SMARCB-deficient) tumor, NUT carcinoma, and high-grade neuroendocrine tumor. H&E stain shows a basaloid low-power appearance (C) with hyaline-appearing cytoplasm showing a “pink” cell appearance, in which the tumor cells are somewhat plasmacytoid (C, inset). Complete loss of INI1/SMARCB1 (D) expression by immunohistochemistry defines this tumor, as seen here. Immunostaining for NUT and synaptophysin (a neuroendocrine marker) were negative.
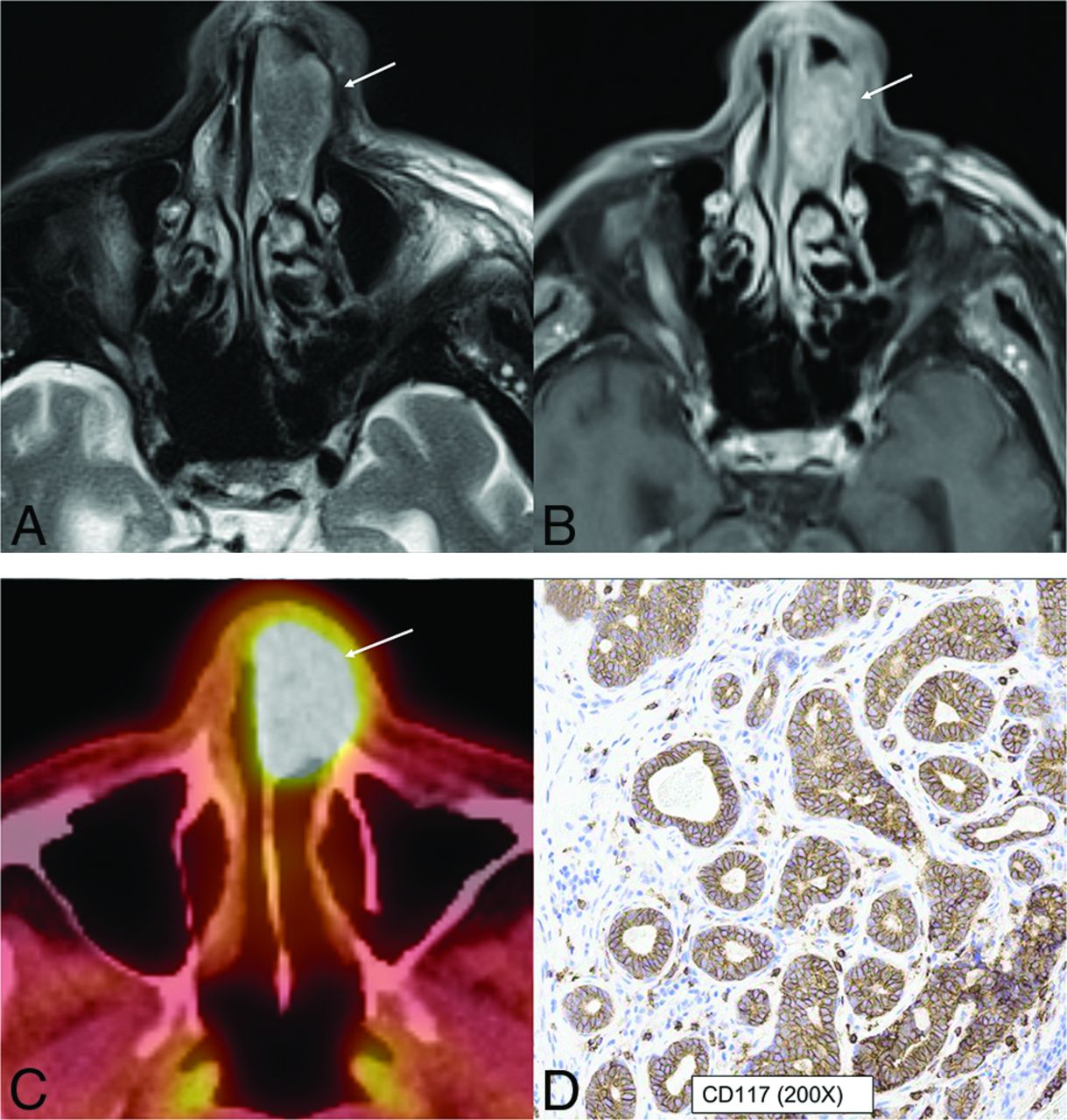
- FIG 7.
HPV-associated multiphenotypic sinonasal carcinoma in an 85-year-old man. A well-circumscribed, low T2-signal mass (A, arrow) with avid contrast enhancement (B, arrow) seen within the left nasal cavity with smooth expansion and high FDG uptake on PET/CT (C, arrow). CD117 (c-kit) (D) highlights the tumor ducts in a staining pattern that is the inverse of the myoepithelial cell markers. Findings of in situ hybridization for HPV (E6/E7) RNA was positive.
- FIG 8.
Biphenotypic sinonasal sarcoma (low-grade sinonasal sarcoma with neural and myogenic features) in a 68-year-old woman. Marked intralesional hyperostotic changes are noted within the nasal component of the tumor (A and B, white arrows). The tumor is well-marginated but locally aggressive with intracranial extension (B, black arrows). H&E stain (C) shows the tumor growing as fascicles of uniform spindle cells with minimal mitotic activity or atypia and overt rhabdomyoblastic differentiation in the form of strap cells (C, arrow). Diffusely positive staining of S-100 (nerve sheath tumor marker) seen as diffuse brown staining (D). Fluorescence in site hybridization testing was positive for PAX3 gene rearrangement, supporting the above diagnosis.
- FIG 9.
Radiographic differentials of an invasive sinonasal mass with intracranial extension are broad with significant overlap in imaging features, including previously described characteristic findings like intratumoral cyst in olfactory neuroblastoma. The final diagnosis is now based primarily on immunohistochemistry and genetics rather than histology. The prognosis of these tumors is also widely variable depending on the underlying molecular and genetic expression. Ca indicates carcinoma.
- FIG 10.
DEK-AFF2 carcinoma. A smooth homogeneous density mass (A, arrow) noted within the posterior ethmoid and nasal cavity with heterogeneous enhancement on MRI (B, arrow). The mass blocks the sphenoethmoidal recess with trapped secretions in the sphenoid sinus. The carcinoma demonstrates classic features of nonkeratinizing SCCa, with blunted papillae and invasion into the stroma as interconnecting ribbons on the H&E stains (C) with infiltrate of inflammatory cells, including lymphocytes and neutrophils. The tumor is diffusely positive for the squamous immunohistochemical marker p40 (D). To evaluate fusion-driven tumor, we performed targeted RNA sequencing, and DEK-AFF2 fusion was found, with breakpoints of DEK (exon 7) and AFF2 (exon 6).










Tables
Summary of changes including deletion, addition, and reclassification of SNT tumors in the 5th edition of the WHO Classification 2022
WHO Classification 4th Edition 2017 (Chapter 1) WHO Classification 5th Edition 2022 (Chapter 2) Respiratory epithelial lesions Hamartomas (new category) REAH REAH Seromucinous hamartoma (new entity in 4th edition) Seromucinous hamartoma Nasal chondromesenchymal hamartoma (reclassification from “other” category) Sinonasal papillomas Subcategory under respiratory epithelial lesions in 5th edition (2022) Respiratory epithelial lesions (includes papillomas, carcinomas, adenocarcinomas with removal of hamartomatous lesions) Sinonasal papillomas Carcinomas Subcategory under respiratory epithelial lesions in 5th edition(2022) Carcinomas Keratinizing SCCa Keratinizing SCCa Nonkeratinizing SCCa Nonkeratinizing SCCa (includes emerging entity DEK-AFF2 carcinoma) Spindle cell (sarcomatoid) SCCa NUT carcinoma Lymphoepithelial carcinoma SWI/SNF complex-deficient sinonasal carcinoma (new entity) Sinonasal undifferentiated carcinoma Sinonasal lymphoepithelial carcinoma NUT carcinoma (new entity in 4th edition) Sinonasal undifferentiated carcinoma (includes emerging entity IDH-mutated carcinoma) Neuroendocrine carcinoma Adenocarcinomas separated as a new subcategory Teratocarcinosarcoma Adenocarcinoma HPV-associated multiphenotypic sinonasal carcinoma (new entity) Intestinal-type adenocarcinoma
Non–intestinal-type adenocarcinomaAdenocarcinomas (new subcategory, was previously under carcinomas) Intestinal-type sinonasal adenocarcinoma
Non-intestinal-type sinonasal adenocarcinomaMalignant soft-tissue tumors Categories removed with dedicated chapters on soft-tissue tumors in the new edition Mesenchymal tumors of the SNT (new category with few retained entities from soft-tissue tumors, occurring exclusively or primarily in the SNT) Borderline/low-grade malignant soft-tissue tumors SNT angiofibroma Benign soft-tissue tumors Sinonasal glomangiopericytoma Neuroectodermal/melanocytic tumors Biphenotypic sinonasal sarcoma Hematolymphoid tumors Chordoma Other tumors Sinonasal ameloblastoma Meningioma Adamantinomatous craniopharyngioma (reclassified from chapter on “nasopharynx”) Sinonasal ameloblastoma Meningioma of the SNT, ear Chondromesenchymal hamartoma (moved to hamartomas) Olfactory neuroblastoma




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.