
Article Figures & Data
Figures
- FIG 1.
Unilateral cerebellitis in a 6-year-old boy who presented with ataxia with increased WBC on blood tests (infectious acute cerebellitis). Lumbar puncture was not performed. MR imaging acquired at presentation (upper row, A–F) shows unilateral left cerebellar gray matter and diffuse T2- and FLAIR hyperintensity (A and B, thick arrow), causing a shift of midline structures and displacement of the vermis (A, thin arrows). DWI (C) and an ADC map (D) show vasogenic (C and D, thick arrows) and cytotoxic edema (C and D, thin arrows). Leptomeningeal contrast enhancement is appreciated on postcontrast T1-weighted imaging (E, thick arrows). Sagittal T2-weighted imaging (F) shows the swollen cerebellum with upward (F, thick arrow) and downward (F, dashed arrow) herniation, supratentorial hydrocephalus, and effacement of the fourth ventricle (F, asterisk) and posterior subarachnoid spaces (F, thin arrow). Last follow-up MR imaging, which was acquired after 68 days, shows near-complete resolution of brain MR imaging findings (lower row, G–L) and atrophy. Note that sagittal T1-weighted imaging (L) shows the complete resolution of swollen cerebellum without any upward (L, thick arrow) and downward herniation (L, dashed arrow), no supratentorial hydrocephalus, and no effacement of the fourth ventricle (L, asterisks) and posterior subarachnoid spaces (L, thin arrow).
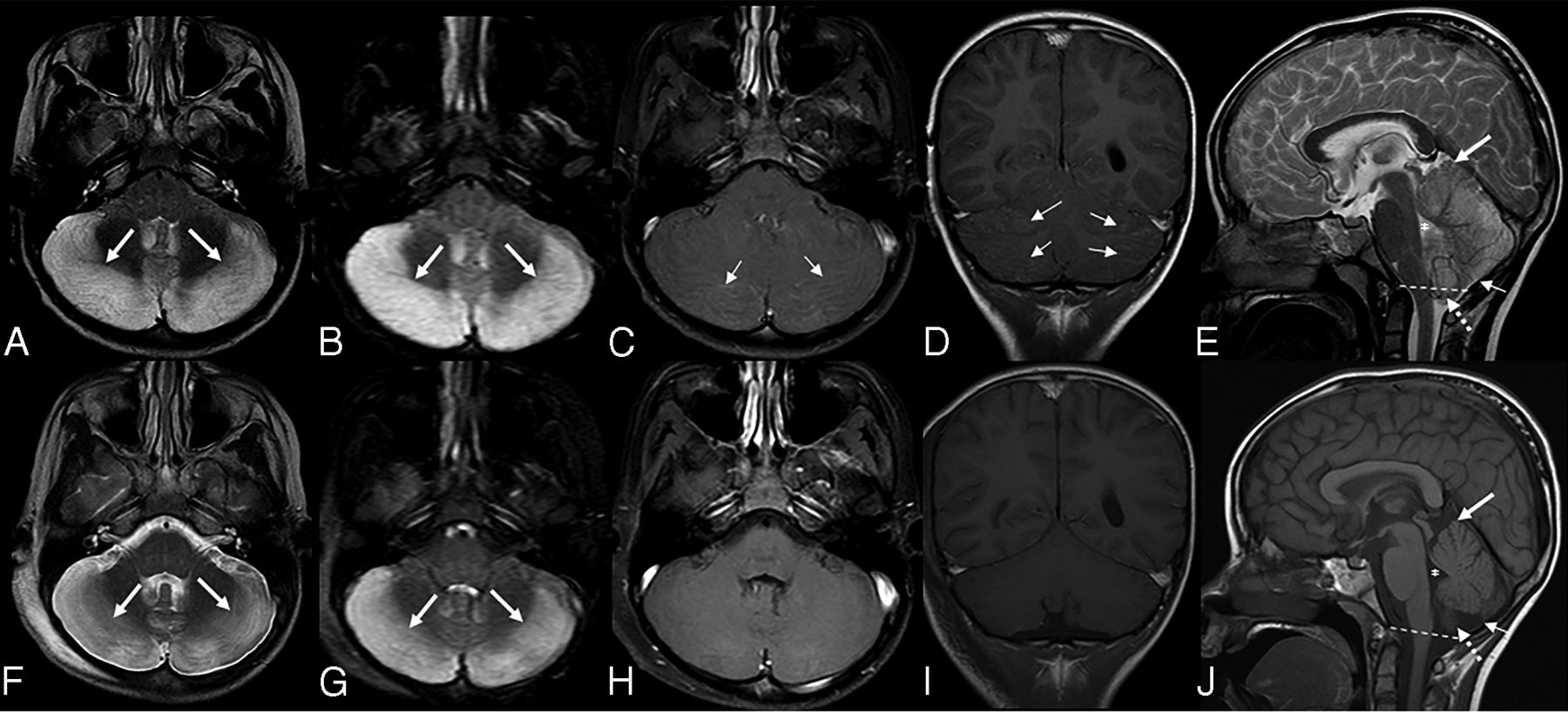
- FIG 2.
Bilateral cerebellitis in a 7-year-old boy who presented with ataxia and headache. He had a history of appendectomy 2 weeks before presentation (infectious acute cerebellitis). Blood tests at the time of imaging revealed WBC within normal limits. There were low total protein levels in the CSF, which was tapped 1 day before. The CSF culture had negative findings. A head CT (not shown) demonstrated diffuse swelling of the bilateral cerebellar hemispheres with crowding at the level of the foramen magnum with supratentorial hydrocephalus. Brain MR imaging acquired a day later (upper row, A–E) shows diffuse bilateral hyperintense signal on T2 (A, thick arrows) and FLAIR (B, thick arrows) sequences with corresponding leptomeningeal enhancement (thin arrows) on postcontrast axial (C) and coronal (D) T1-weighted imaging. Sagittal T2-weighted imaging (E) shows the swollen cerebellum with upward (E, thick arrow) and downward (E, dashed arrow) herniation, supratentorial hydrocephalus, and effacement of the fourth ventricle (E, asterisk) and posterior subarachnoid spaces (E, thin arrow). Follow-up MR imaging (lower row, F–J) acquired after 8 days shows improvement of hyperintense signal on axial T2 (F, thick arrows) and FLAIR (G, thick arrows) sequences. No contrast enhancement is seen on postcontrast axial (H) and coronal (I) T1-weighted imaging. Sagittal T1-weighted imaging (J) shows complete resolution of cerebellar edema, no upward (J, thick arrow) and downward (J, dashed arrow) herniation, no supratentorial hydrocephalus, and no effacement of the fourth ventricle (J, asterisk) and posterior subarachnoid spaces (J, thin arrow).
- FIG 3.
Acute disseminated encephalomyelitis in a 5-year-old girl who presented with ataxia and absent lower extremity reflexes (immune-mediated acute cerebellitis). Blood tests and CSF revealed an increased white blood cell count. CSF culture had negative findings. Brain MR imaging at presentation shows bilateral, diffuse, patchy hyperintense signal on axial T2 (A, arrows) and FLAIR (B, arrows) sequences. Corresponding vasogenic edema is seen on axial DWI (C, arrows) and ADC (D, arrows). Axial postcontrast T1-weighted imaging demonstrates bilateral, subtle leptomeningeal contrast enhancement (E, arrows). Consecutive supratentorial slices reveal subtle T2-hyperintense signal in the white matter of the adjacent trigone of the left lateral ventricle (F and G, arrow) without contrast enhancement or diffusion alteration (not shown). Sagittal T1-weighted imaging (H) shows no upward or downward herniation. Follow-up MR imaging was not available.
- FIG 4.
Bilateral cerebellitis in a 6.5-year-old boy (infectious acute cerebellitis) who had a history of gastroenteritis for 2–3 days. He developed marked and prolonged headache after a few days. Neurologic examination showed no cerebellar dysfunction. CSF examination was not performed. MR imaging shows bilateral, diffuse, T2 hyperintense signal and mild edema (A–C, arrows) in the cerebellar white and gray matter. Postcontrast imaging shows mild leptomeningeal contrast enhancement (D–F, arrows).
- FIG 5.
Bilateral cerebellitis in a 12.5-year-old girl (infectious acute cerebellitis). Initial presentation was nonspecific. The patient was tired with headache for a few days and spontaneously recovered. MR imaging at presentation (upper row) shows bilateral, diffuse, T2-hyperintense signal predominantly on the right side (A–D, arrows) and downward herniation (D, dashed line). A follow-up examination after 3 months shows no abnormal neurologic findings. Follow-up MR imaging after 3 months (lower row) shows complete resolution of previous MR imaging findings (E–H).
- FIG 6.
Upper row A–C, Acute disseminated encephalomyelitis in a 1-year 10-month-old boy (with immune-mediated acute cerebellitis) who presented with acute ataxia and fever with vomiting. A blood test revealed increased white blood cell count, and CSF revealed elevated WBC and normal protein and glucose levels. Blood culture and CSF culture had negative findings. Lower row D–F, Bilateral cerebellitis in a 5-year-old boy (with infectious acute cerebellitis) with a history dominated by intense headache, predominantly at night with some fluctuation. The patient had treatment of symptoms, but there was no clear improvement in headaches. MR imaging was performed about 2 weeks later. He had no cerebellar signs on examination. This figure aims to show the most predominant MR imaging findings for immune-mediated versus infectious acute cerebellitis. Note that there is no downward herniation in immune-mediated acute cerebellitis (A) versus cerebellar tonsil downward herniation in infectious acute cerebellitis (D, arrow). Axial T2 shows subtle hyperintense signal in right middle cerebellar peduncle in immune-mediated acute cerebellitis (B, arrow) versus bilateral diffuse T2-hyperintense signal with diffuse edema in infectious acute cerebellitis (E, arrows). Note that axial FLAIR shows extensive, multifocal, and confluent bilateral hyperintensity involving the cerebral white matter and the gray matter, including the bilateral basal ganglia extensively and bilateral thalami (C, arrows) in immune-mediated acute cerebellitis versus normal supratentorial brain axial T2 signal intensities in infectious acute cerebellitis (F).






Tables
Brain MR imaging findings at presentation between infectious (n = 35) and immune-related (n = 8) acute cerebellitis subgroups
T2/FLAIR Hyperintense Signal Infectious (No.) (%) Immune-Related (No.) (%) P Valuea Unilateral cerebellar 4 (11.42) 2 (25.00) .31 Bilateral cerebellar 27 (77.14) 4 (50.00) .19 Brainstem 1 (2.85) 3 (37.50) .016 Supratentorial brain 0 (0.00) 3 (37.50) .004 Cerebellar white matter 10 (28.57) 1 (12.50) .65 Cerebellar gray matter 25 (71.42) 5 (62.50) .68 Associated findings Involvement of vermis 8 (22.85) 1 (12.50) 1.00 Effacement of fourth ventricle 12 (34.28) 1 (12.50) .39 Effacement of posterior fossa subarachnoid spaces 11 (31.42) 0 (0.00) .09 Downward herniation 15 (42.85) 0 (0.00) .03 Upward herniation 10 (28.57) 0 (0.00) .16 Supratentorial hydrocephalus 8 (22.85) 0 (0.00) .31 Contrast enhancement Leptomeningeal 12 (34.28) 2 (28.57) 1.00 Cortical 7 (20.00) 1 (14.28) 1.00 Diffusion-weighted imaging Vasogenic edema 20 (58.82) 4 (50.00) .71 Cytotoxic edema 6 (17.64) 1 (12.50) 1.00 ↵a P is based on the Fisher exact test.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.