
Article Figures & Data
Figures
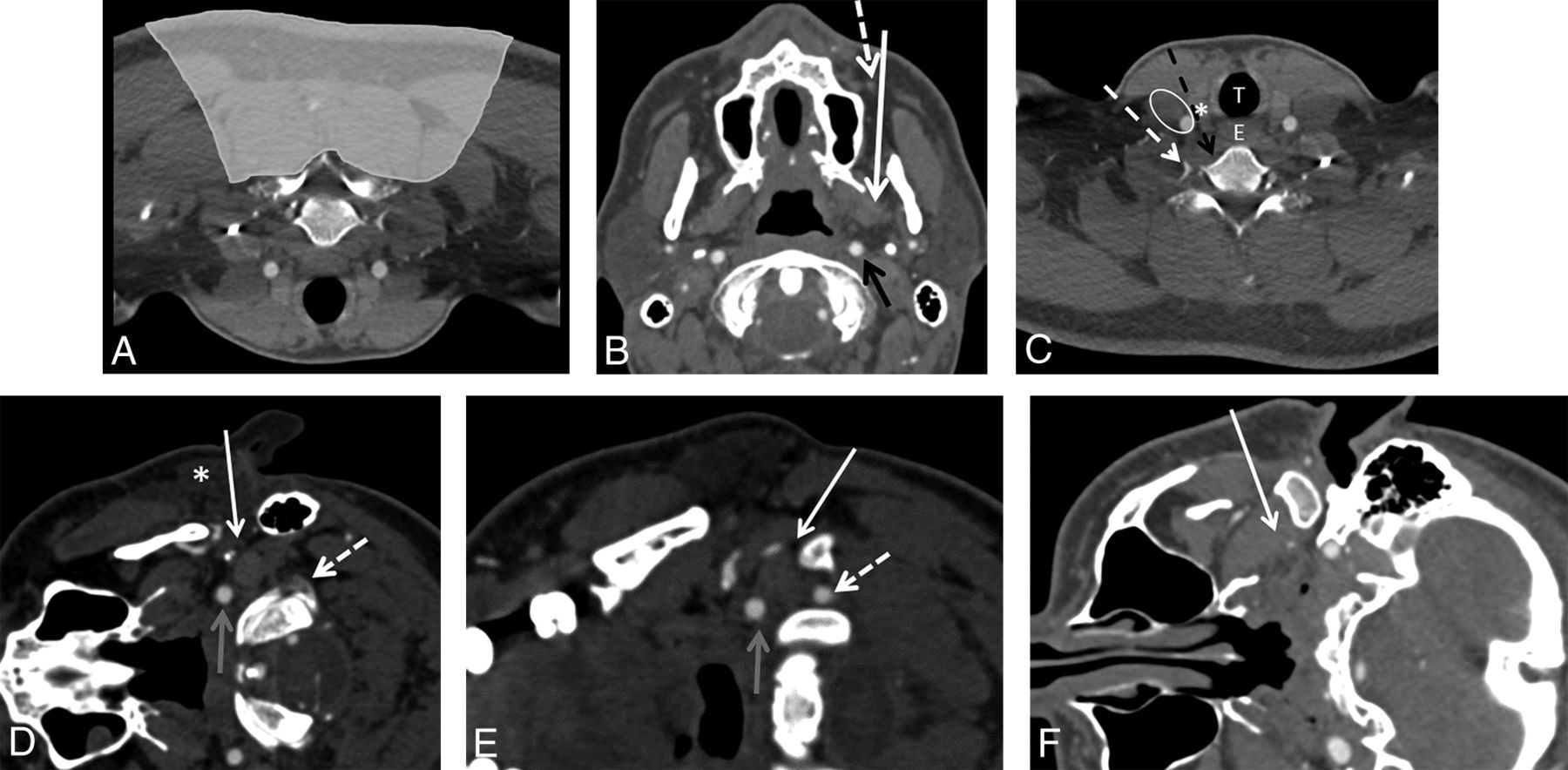
- FIG 1.
CT-guided neck biopsies can be performed using multiple different approaches depending on the location of the lesion. In almost all approaches, there are critical neural and vascular structures adjacent to the needle tract. A, CT angiogram of the neck flipped vertically to depict prone positioning for a posterior-approach neck biopsy. Neck biopsies in the shaded region would commonly be performed using a posterior approach. In the shaded region, there are no critical neurovascular structures. B, CT angiogram soft-tissue-windowed image of the neck with the patient in a supine position for the paramaxillary approach (white arrow). The needle course is between the maxillary sinus and the mandible adjacent to the facial artery (dashed arrow) through the buccal space. This approach can be used for lesions in the buccal, masticator, parapharyngeal, retropharyngeal, and carotid sheath spaces. The critical structures to avoid include the facial artery (dashed arrow) and the internal carotid artery (black arrow). C, CT angiogram of the neck with the patient in a supine position for anterior-approach biopsies, which can be either medial (black dashed arrow) or lateral (dashed white arrow) to the carotid and jugular vasculature (white oval). These approaches can be used for lesions in the infrahyoid neck and lower cervical vertebrae. The critical structures to avoid include the carotid artery, jugular vein, and vagus nerve (white oval); the trachea (white T); the esophagus (white E); and the thyroid gland (white asterisk). CT angiograms of the neck with the patient in a decubitus position: This positioning will be used for the retromandibular (D), submastoid (E), and subzygomatic (F) approaches denoted by white arrows. Note that the needle will sometimes pass through a portion of the parotid gland for the retromandibular approach (white asterisk). Critical structures to avoid include the carotid (gray arrows) and vertebral arteries (dashed white arrows) with the retromandibular and submastoid approaches and the retromandibular vein in the retromandibular approach because of its proximity to the facial nerve. These approaches can be used for lesions in the deep parotid, parapharyngeal, pharyngeal, and retropharyngeal spaces.
- FIG 2.
A 74-year-old woman with a previously excised papillary thyroid carcinoma also treated with radioactive iodine who has a new mass in the right visceral space of the neck adjacent to the thyroidectomy bed. Axial contrast-enhanced CT image (A) from a neck CT demonstrates an enhancing mass (black asterisk) in the right visceral space abutting the trachea (white asterisk), the esophagus (white oval), and the right internal jugular vein (dashed white arrow). Intraprocedural axial CT soft-tissue-windowed image (B) with the core biopsy needle in place. An anterior approach was chosen to pass just medial to the internal jugular vein (dashed white arrow), just lateral to the trachea (white asterisk), and stopping short of the esophagus (white oval). The histopathology from the biopsy was recurrent papillary thyroid carcinoma.
- FIG 3.
A 75-year-old woman with previously excised and re-excised left base-of-tongue and retromolar squamous cell carcinoma. Axial contrast-enhanced neck CT (A) and fused PET/CT (B) images demonstrate an enhancing FDG avid mass (black asterisk) in the left masticator space. A paramaxillary approach was chosen to perform the biopsy (C). The histopathology from the biopsy was recurrent squamous cell carcinoma. With this biopsy, the facial artery is medial to the needle-entry site just anterior to the maxilla and is not problematic for the needle path.
- FIG 4.
A 69-year-old woman with an incidentally found right-neck mass on a cervical spine MR imaging. Axial T2-weighted MR image (A) from a cervical spine MR imaging demonstrates an indeterminate T2-hyperintense mass (white asterisk) at the deep margin of the parotid gland, centered within the parapharyngeal space posterior to the masticator space. Intraprocedural contrast-enhanced soft-tissue-windowed CT image (B) with the patient in the left lateral decubitus position. Note the internal carotid artery (white arrow) and other vascular structures including the retromandibular vessels adjacent to the mandibular ramus (white dashed arrow). Intraprocedural axial CT bone-windowed image (C) with the core biopsy needle in place (black arrow). A retromandibular course with the entry point posterior to the ear was chosen to access the mass. The needle path is to avoid the vascular structures adjacent to the mandibular ramus, including the retromandibular vein, but anterior to the styloid process (black dashed arrow) and internal carotid artery (approximately at the site of the black asterisk but occult on noncontrast CT). The pathology was adenoid cystic carcinoma.
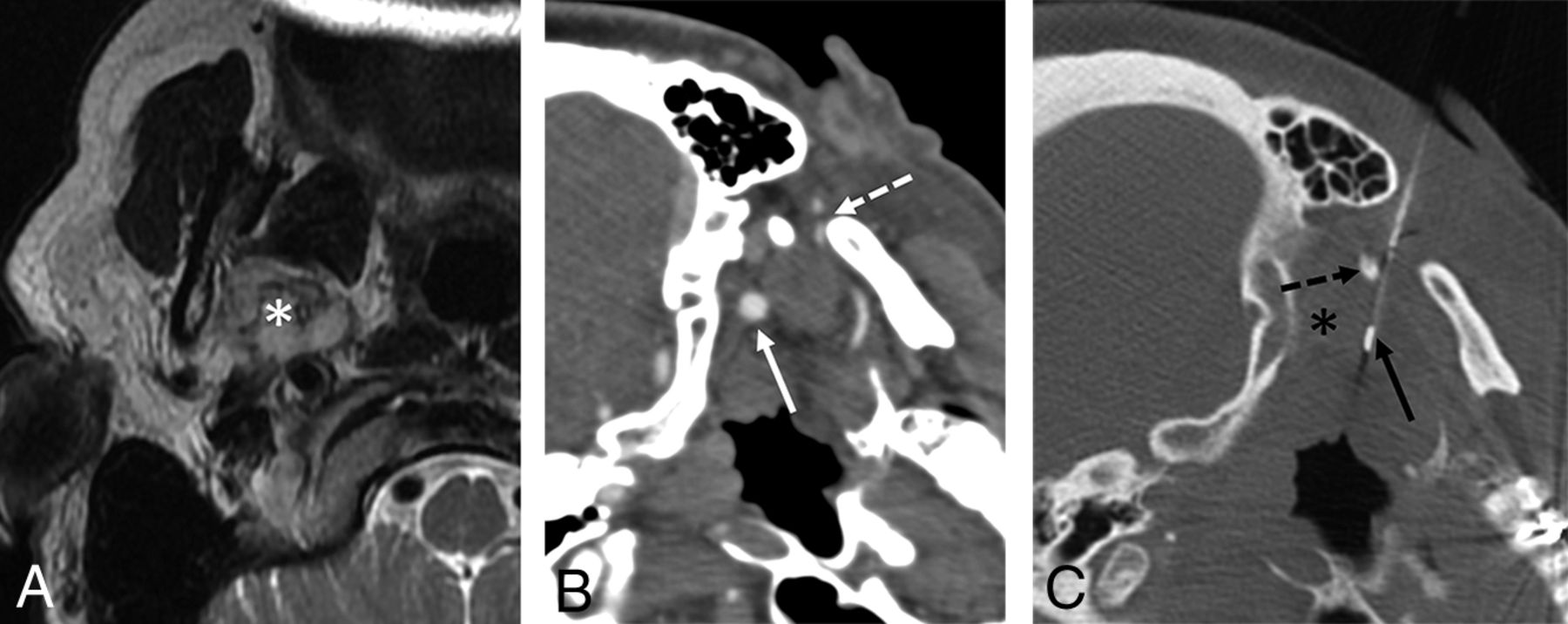
- FIG 5.
A 25-year-old man with neurofibromatosis type 1, new vagus nerve–related symptoms, and a enlarging painful left carotid space mass. Axial T1-weighted fat-suppressed postcontrast MR image (A) from a neck MR imaging demonstrates an enhancing carotid space mass (black asterisk). Intraprocedural contrast-enhanced soft-tissue-windowed CT image (B) with the patient supine but with the head turned to the right. Note that the mass (white asterisk) is located between the internal carotid (black arrow) and vertebral (black dashed) arteries and is pushing the carotid artery anteriorly. Intraprocedural axial CT soft-tissue-windowed image (C) with the core biopsy needle in place (white arrow). A submastoid approach was chosen to avoid the carotid and vertebral arteries. The histopathology from the biopsy was neurofibroma. Given the progressive symptoms, concern for sampling error, and the high risk given the diagnosis of type neurofibromatosis 1, the mass was excised and final pathology was plexiform neurofibroma containing focal areas of low-grade malignant peripheral nerve sheath tumor.





Tables
Size and Brand No. Biopsy needle gauge 14-ga 14 16-ga 6 18-ga 6 20-ga 1 Needle brand Bard Mission 13 Achieve 9 Unknown 5 Arrow OnControl 2a a The OnControl needle used for access in 2 cases followed by coaxial placement of a soft-tissue needle.
Approach No. Anterior 7 Paramaxillary 2 Posterior 5 Retromandibular 2 Submastoid 8 Subzygomatic/sigmoid notch 3 Target Lesion No. Anterior cervical 3 Carotid space 3 Masticator space 5 Parapharyngeal 6 Perivertebral 7 Pharyngeal 1 Prevertebral 1 Visceral space 1 Histopathology No. Acute on chronic inflammation 1 Adenoid cystic carcinomaa 1 Atypical melanin rich neoplasma 1 Benign fibrocollagenous tissue 1 Chondroid lesion 1 Fibrosis with foreign body giant cell reaction 1b Granulation tissue 1 Metastatic myxoid liposarcomaa 1 Malignant peripheral nerve sheath tumora 2 Myxoma 1 Neurofibroma 1b Papillary thyroid cancera 1 Pleomorphic adenoma 1 Round cell sarcomaa 1 Schwannoma 2 Spindle cell neoplasma 1 Squamous cell carcinomaa 8 Synovial cyst 1




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Ultrasound Fusion-Guided Core Needle Biopsy for Deep Head and Neck Space Lesions: Technical Feasibility, Histopathologic Yield, and Safety
- Percutaneous CT-Guided Core Needle Biopsies of Head and Neck Masses: Review of 184 Cases at a Single Academic Institution, Common and Special Techniques, Diagnostic Yield, and Safety