
Article Figures & Data
Figures
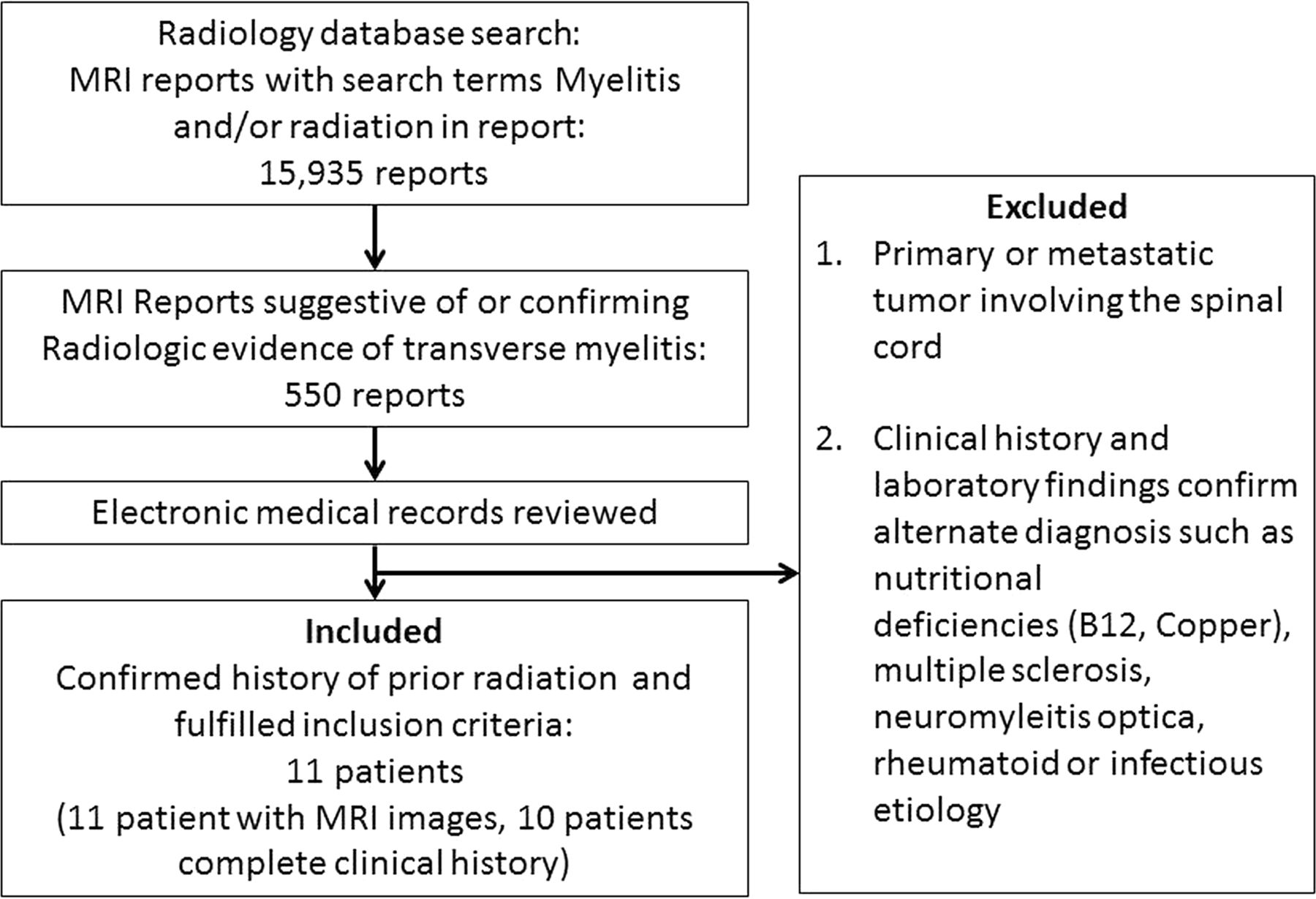
- Fig 1.
Study schema describes the method used to identify the patients in this series. It also highlights the rarity of the occurrence of radiation myelitis.
- Fig 2.
Longitudinally extensive myelitis. A, The cervical or thoracic cord or both were involved in all patients in a longitudinally extensive pattern. B, Maximum myelopathic changes (yellow arrows) correspond to the central field of radiation identified by apparent fatty vertebral bone marrow on T1-weighted images (yellow brackets).
- Fig 3.
Central cord involvement. The central two-thirds of the cord on axial T2-weighted images was involved in 9 patients, and 1 patient presented with a small focal area of central and dorsal cord involvement.
- Fig 4.
Sequential changes on imaging in a patient with severe radiation myelitis. Fatty bone marrow changes present with hyperintense T1 signal involving C7 and the upper thoracic vertebrae on the first image (white arrows). Less extensive longitudinally extensive myelitis at the C7, T1, and T2 levels is noted on the T2-weighted image with hyperintense signal at presentation (yellow arrow). At 3 months, cord expansion and extensive T2/STIR hyperintense signal changes involving the cervical and upper thoracic cord are noted (white arrowhead) with contrast enhancement at the C7, T1, and T2 levels (single large white arrowhead). The patient was paraplegic with urinary and bowel incontinence. She was treated with a high dose of steroids. Follow-up images at 18 months show cord atrophy (blue arrow). She eventually was able to ambulate with a walker after extensive physical therapy. CE indicates contrast enhancement.




Tables
Symptoms at presentationa Paresthesia lower limbs: 6/10 (60%) Pain (back and legs): 5/10 (50%) Lower extremity motor weakness: 7/10 (70%) Urinary incontinence: 4/10 (40%) Bowel incontinence: 2/10 (20%) Treatment received Steroids: 9 IvIg: 1 Hyperbaric oxygen: 2 Plasmapheresis: 2 Bevacizumab (Avastin): 1 Mean duration of clinical follow-up (mo) 22 (range: 4–162) Clinical course on follow-up (available in 7 patients) Improved with some sequelae: 5 Progressive: 2 Resolved: 0 Note:—IvIg indicates intravenous immunoglobulin.
↵a Detailed clinical examination was not available for 1 patient. Hence, only 10 patients were included for evaluation of the clinical course.
Attributes Median (Range) Sex 6 males, 5 females Median age (yr) 33 (11–60) Primary malignancy (No. of patients) 1) Recurrent Hodgkin lymphoma: 5 2) Hodgkin lymphoma: 1 3) Gastric carcinoma: 1 4) Acute lymphocytic lymphoma: 1 5) Brain stem glioma: 1 6) Medulloblastoma: 1 7) Recurrent multiple myeloma: 1 Median time to symptom onset from RT (mo) 17 (2–194) Median delay in diagnosis from symptom onset (mo) 6 (0–14) Note:—RT indicates radiation therapy.
Patient Age (yr) Cancer Type Prior Chemotherapy Prior Chemotherapy Regimen Adjuvant Chemotherapy 1 33 Recurrent Hodgkin lymphoma Yes ABVD ICE followed by cyclophosphamide (Cytoxan) and busulfan Autologous bone marrow transplant 2 32 Recurrent Hodgkin lymphoma Yes CHOP/ABVD Ara-C, vincristine, cisplatin Danazol 3 11 Brain stem medulloblastoma No – Vincristine, VP-16, carboplatin CCNU, cisplatin 4 60 Recurrent gastric adenocarcinoma (stage IV) No – 5-FU, leucovorin 5 42 Refractory acute lymphocytic leukemia Yes Hyper-CVAD Intrathecal cytarabine Methotrexate Autologous bone marrow transplant 6-Mercaptopurine 6 41 Hodgkin lymphoma No – No 7 29 Brain stem glioma No – TMZ 8 28 Recurrent Hodgkin lymphoma Yes ABVD ICE followed by cyclophosphamide and busulfan Autologous bone marrow transplant 9 33 Recurrent Hodgkin lymphoma Yes ABVD ICE followed by cyclophosphamide and busulfan Brentuximab vedotin Autologous bone marrow transplant 10 37 Recurrent Hodgkin lymphoma Yes ABVD ICE followed by cyclophosphamide and busulfan Autologous bone marrow transplant Note:—ABVD indicates doxorubicin, bleomycin, vinblastine, dacarbazine; CHOP, cyclophosphamide, doxorubicin hydrochloride, vincristine, prednisone; Hyper-CVAD, cyclophosphamide, vincristine, doxorubicin, and dexamethasone; TMZ, temozolomide; CCNU, lomustine; ICE, ifosfamide, carboplatin, etoposide chemotherapy protocol; Vp-16, etoposide phosphate.
Mean time from symptom onset to first MRI (mo) 6 (Range, 0–41) Level of longitudinally extensive myelitis (No. of patients) (%) Cervical: 3 (27%) Thoracic: 5 (45%) Cervical and thoracic: 2 (18%) Entire spine: 1 (9%) Level of vertebral T1 hyperintensities (No. of patients) (%) Cervical: 2 (18%) Cervical and thoracic: 3 (27%) Thoracic: 1 (9%) Thoracic and lumbar: 1 (9%) Entire spine: 2 (18%) No changes: 2 (18%) Location of axial T2 changes (No. of patients) (%) Central (>2/3): 4 (36%) Central and posterior: 1 (9%) Entire cord: 5 (45%) Indeterminate: 1 (9%) Cord expansion (No. of patients) (%) Present: 6 (54%) Absent: 3 (27%) Indeterminate: 2 (18%) Contrast enhancement (No. of patients) (%) Enhancement present: 5 (45%) No enhancement: 5 (45%) Contrast not given: 1 (9%) Radiographic follow-up available Yes: 8 No: 3 Median follow-up (mo) 14.5 (4–69) Cord atrophy (No. of patients) (%) Present: 2 (25%) Absent: 6 (75%) T2 findings (No. of patients) (%) Decreased T2 abnormalities: 4 (50%) Resolved: 1 (12.5%) Hemorrhagic changes: 1 (12.5%) Syringohydromyelia: 1 (12.5%) Persistent T2 abnormalities: 4 (50%)




{kind=link}
{kind=link}
{kind=link}
{kind=link}