
Article Figures & Data
Figures
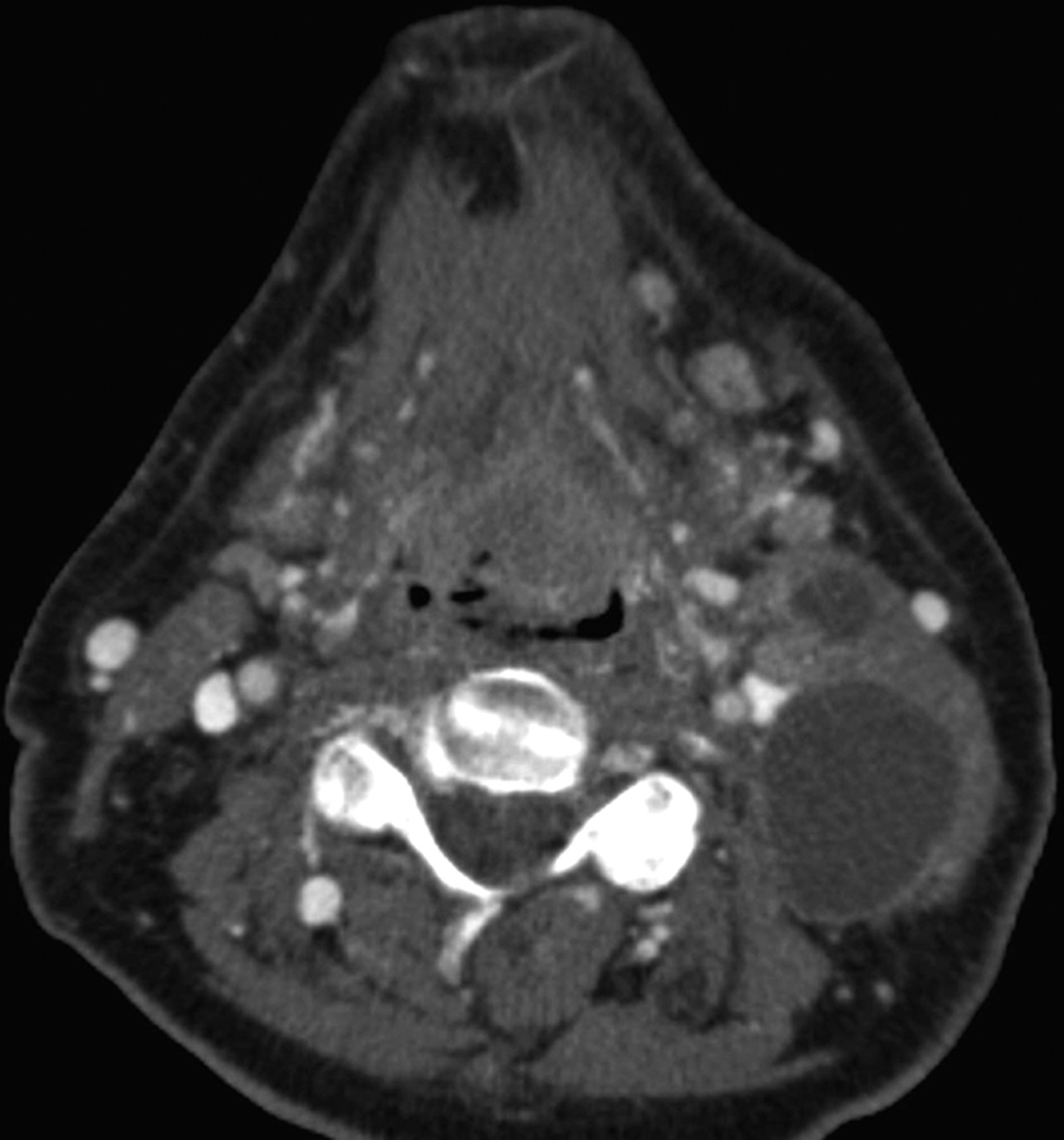
- Fig 1.
Axial contrast-enhanced CT in a 69-year-old man demonstrates a heterogeneously enlarged lingual tonsil filling the valleculae and at least 2 left cystic cervical nodes. No right neck adenopathy was evident. Biopsy of the primary site revealed p16(+) OPSCC. This was staged as cT2N2b, stage IVA OPSCC. In the eighth edition of the AJCC, the T-category does not change; however, multiple ipsilateral nodes are now assigned N1 category if <6 cm in greatest diameter. In the eighth edition, T2N1 p16(+) OPSCC is designated stage I disease.
- Fig 2.
HPV-related p16(+) OPSCC in a 62-year-old man presenting with bilateral neck masses determined to be p16+ squamous cell carcinoma. Coronal T1 postcontrast fat-saturated MR image (A) demonstrates a left tonsillar tumor extending superiorly to the soft palate. Because this tumor measured >4 cm in longest dimension, it is assigned T3 with no change in the primary tumor staging from the seventh-to-eighth edition of the AJCC Cancer Staging Manual. Axial T2 fat-saturated image (B) shows bilateral heterogeneous nodal masses with a high degree of suspicion of extranodal extension bilaterally. In the seventh edition, bilateral adenopathy of <6 cm in greatest dimension for all OPSCCs is designated T2c disease, with prognostic grouping of T3N2c as stage IVA. In the new eighth edition, bilateral adenopathy of <6 cm is N2 disease and the new prognostic grouping for p16+ OPSCC T3N2 is stage II. Extranodal extension does not affect the N designation for HPV/p16(+) OPSCC or NPC.
- Fig 3.
Two patients with nasopharyngeal carcinoma. A and B, A 64-year-old man with a nasopharyngeal mass found incidentally on PET/CT and determined to be EBV(+) undifferentiated nonkeratinizing carcinoma. Axial T1 postcontrast fat-saturated images (A and B) demonstrate an asymmetric nasopharyngeal mass with lateral extension to the right masticator space lateral pterygoid muscle. In the seventh edition, this would be T4 disease; however, in the eighth edition, this is only T2 disease. Note however that in this patient, there is also involvement of the pterygoid plates, which is now clarified as T3 disease, and superior extension to the right cavernous sinus, which is T4 disease in both AJCC Cancer Staging Manual seventh and eighth editions. C and D, A 15-year-old boy presenting with epistaxis and a large mass arising from the nasopharynx determined to be EBV(+) undifferentiated nonkeratinizing carcinoma. Sagittal T1 (C) shows the large mass filling the nasopharynx, extending inferiorly to the oropharynx and anteriorly to the nasal cavity. Axial postcontrast T1 with fat saturation (D) shows lateral extension of the mass into the masticator space but also to the left parotid gland. In the eighth edition, involvement of the parotid gland or extension of tumor beyond the lateral surface of the lateral pterygoid muscle determines T4 status.
- Fig 4.
Axial T2-weighted MR image through the neck in a 45-year-old man presenting with neck masses. The enlarged solid left level 2A node measured 3.5 cm in maximal diameter with additional abnormal nodes seen on the right at 2A and bilaterally at levels 3 and 5A. No primary tumor was evident on clinical examination or on this MR imaging. In the absence of a primary tumor, it is difficult to determine which nodal table to use, though most unknown primary tumors are HPV/p16(+) OPSCC. If fine-needle aspiration of the node reveals HPV/p16(+), then an OPSCC primary would be assumed and this would be assigned T0N2. If pathology revealed HPV-negative, p16 negative, and ENB negative, then this would be assigned N2c and no primary site assigned. Fine-needle aspiration revealed this to be undifferentiated, nonkeratinizing carcinoma EBV+, with categories then assigned as T0N2 NPC.




Tables
N Category N Criteria Nx Regional lymph nodes cannot be assessed N0 No regional lymph node metastasis N1 Metastasis in a single ipsilateral lymph node ≤3 cm in greatest dimension and ENE− N2a Metastasis in a single ipsilateral lymph node >3 cm but ≤6 cm in greatest dimension and ENE− N2b Metastasis in multiple ipsilateral nodes, none >6 cm in greatest dimension and ENE− N2c Metastasis in bilateral or contralateral lymph node(s), none >6 cm in greatest dimension and ENE− N3a Metastasis in a lymph node >6 cm in greatest dimension and ENE− N3b Metastasis in any node(s) with clinically overt ENE+ (ENEc) Note:—ENEc indicates invasion of skin, infiltration of musculature, dense tethering or fixation to adjacent structures, or cranial nerve, brachial plexus, sympathetic trunk, or phrenic nerve invasion with dysfunction.
↵a Note the addition of ENE to the staging system, creating a new N3b designation in the eighth edition of the AJCC Cancer Staging Manual. Table used with the permission of the American Joint Committee on Cancer (AJCC), Chicago, Illinois. The original source for this material is the AJCC Cancer Staging Manual.1
N Category N Criteria Nx Regional lymph nodes cannot be assessed N0 No regional lymph node metastasis N1 One or more ipsilateral lymph nodes, none larger than 6 cm N2 Contralateral or bilateral lymph nodes, none >6 cm N3 Lymph node(s) >6 cm ↵a The HPV-related OPSCC nodal staging shows a dramatic change compared with the eighth edition non-HPV OPSCC staging. Table adapted with permission of the American Joint Committee on Cancer, Chicago, Illinois. The original source for this material is the AJCC Cancer Staging Manual.1
N Category N Criteria Nx Regional lymph nodes cannot be assessed N0 No regional lymph node metastasis N1 Unilateral metastasis in cervical lymph node(s) and/or unilateral or bilateral metastasis in retropharyngeal lymph node(s) ≤6 cm in greatest dimension, above the caudal border of cricoid cartilage N2 Bilateral metastasis in cervical lymph nodes ≤6 cm in greatest dimension, above the caudal border of cricoid cartilage N3 Unilateral or bilateral metastasis in cervical lymph node(s) >6 cm in greatest dimension, and/or extension below the caudal border of cricoid cartilage ↵a Changes in the eighth edition reflect the designation of level IV or VB nodes as N3 disease with no distinct a or b status. Table adapted with permission of the American Joint Committee on Cancer, Chicago, Illinois. The original source for this material is the AJCC Cancer Staging Manual.1
T Category T Criteria T0 No primary identified T1 Tumor ≤2 cm in greatest dimension T2 Tumor >2 but ≤4 cm in greatest dimension T3 Tumor >4 cm in greatest dimension or extension to lingual surface of epiglottis T4 Moderately advanced local disease; tumor invades the larynx, extrinsic muscles of tongue, medial pterygoid, hard palate or mandible, or beyond ↵a The T4a and T4b features from OPSCC staging in the seventh edition are now combined as T4 in the new eighth edition. Table adapted with permission of the American Joint Committee on Cancer, Chicago, Illinois. The original source for this material is the AJCC Cancer Staging Manual.1
When T Is… And N Is… And M Is… Then the Stage Group Is… T0, T1, or T2 N0 or N1 M0 I T0, T1, or T2 N2 M0 II T3 N0, N1, or N2 M0 II Any T N3 M0 III T4 Any N M0 III Any T Any N M1 IV ↵a Table adapted with permission of the American Joint Committee on Cancer, Chicago, Illinois. The original source for this material is the AJCC Cancer Staging Manual.1
T Category T Criteria Tx Primary tumor cannot be assessed T0 No tumor identified, but EBV+ cervical lymph node(s) involvement Tis In situ carcinoma T1 Tumor confined to nasopharynx, or extension to oropharynx and/or nasal cavity without parapharyngeal involvement T2 Tumor with extension to parapharyngeal space, and/or adjacent soft-tissue involvement (medial pterygoid, lateral pterygoid, prevertebral muscles) T3 Tumor with infiltration of bony structures at skull base, cervical vertebrae, pterygoid structures, and/or paranasal sinuses T4 Tumor with intracranial extension, involvement of cranial nerves, hypopharynx, orbit, parotid gland, and/or extensive soft-tissue infiltration beyond the lateral surface of the lateral pterygoid muscle ↵a The eighth edition shows critical changes from the prior edition with downstaging of masticator space involvement from T4 to T2 and clarification of the T-staging for invasion of bony structures. Table adapted with permission of the American Joint Committee on Cancer, Chicago, Illinois. The original source for this material is the AJCC Cancer Staging Manual.1
T Category T Criteria Tx Primary tumor cannot be assessed Tis Carcinoma in situ T1 Tumor ≤2 cm, ≤5-mm DOI; DOI is depth of invasion and not tumor thickness T2 Tumor ≤2 cm, DOI >5 mm and ≤10 mm or tumor >2 but ≤4-cm and ≤10-mm DOI T3 Tumor >4 cm or any tumor >10-mm DOI T4a Moderately advanced local disease; tumor invades adjacent structures only (eg, through cortical bone of the mandible or maxilla or involves the maxillary sinus or skin of the face); note that superficial erosion of bone/tooth socket (alone) by a gingival primary is not sufficient to classify a tumor as T4 T4b Very advanced local disease; tumor invades masticator space, pterygoid plates, or skull base and/or encases the internal carotid artery ↵a Note that the greatest diameter of the primary tumor is still measured, but primary tumor depth of invasion is also a critical determinant of T-staging. This is the deep extent of tumor invasion below the surface and is distinct from tumor thickness. Lip tumors are no longer staged along with oral cavity SCC, but using the tables from “Cutaneous Carcinoma of HN.” Table adapted with permission of the American Joint Committee on Cancer, Chicago, Illinois. The original source for this material is the AJCC Cancer Staging Manual.1
T Category T Criteria Tx Primary tumor cannot be identified Tis Carcinoma in situ T1 Tumor ≤2 cm in greatest dimension T2 Tumor >2 but ≤4 cm in greatest dimension T3 Tumor >4 cm in maximum dimension or minor bone erosion or perineural invasion, or deep invasionb T4a Tumor with gross cortical bone/marrow invasion T4b Tumor with skull base invasion and/or skull base foramen involvement ↵a This new chapter in the eighth edition should be used for all HN cutaneous malignancies except the eyelid and cutaneous melanoma and Merkel cell carcinoma. Lip tumors are now staged using this table. Table adapted with permission of the American Joint Committee on Cancer, Chicago, Illinois. The original source for this material is the AJCC Cancer Staging Manual.1
↵b Deep invasion is defined as invasion beyond the subcutaneous fat or >6 mm (as measured from the granular layer of adjacent normal epidermis to the base of the tumor). Perineural invasion for the T3 classification is defined as tumor cells within the nerve sheath of a nerve lying deeper than the dermis or measuring ≥0.1 mm in caliber or presenting with clinical or radiographic involvement of named nerves without skull base invasion or transgression.




{kind=link}
{kind=link}
{kind=link}
{kind=link}