
Article Figures & Data
Figures
- FIG 1.
Illustration depicting the common location of meningiomas and associated genetic/cytogenetic alteration and grades. NF2 and SMARCB1 mutations are more frequently seen in convexity meningiomas. Grade 2 and 3 meningiomas are more common along the convexity than the skull base. AKT1, KLF4, TRAF7, and POLR2A genetic changes are more frequently seen in skull base meningiomas. Grade 1 is more common in the posterior fossa. Grade 2 (atypical) meningiomas are more frequently seen along the brain convexity and spine and can have a loss of a copy of chromosomes 1, 10, or 14.
- FIG 2.
“Mutation map” of skull base meningiomas with a regional propensity of meningiomas dependent on specific mutations. Meningiomas arising from the sphenoid wing have KLF4/TRAF7 mutations, midline tumors have AKT1/TRAF7 mutations, and tumors originating from the olfactory groove tend to have SMO mutations. Meningiomas along the posterior skull base commonly have a loss of chromosome 22-loss (NF2). Adapted from Baranoski J. Smarcb1-Mutant Intracranial Meningiomas: A Distinct Subtype of Nf2-Mutant Tumors, 2015. Yale Medicine Thesis Digital Library. 1947.
- FIG 3.
“Mutation map” of convexity meningiomas with the regional propensity of meningiomas dependent on a specific mutation. Meningiomas along the falx and midline parasagittal region tend to have the SMARCB1 mutation. Meningiomas along the posterior cerebral convexity tend to have NF2/chromosomal 22 with higher chances of TRAF mutation along the anterior cerebral convexity. Adapted from Baranoski J, Smarcb1-Mutant Intracranial Meningiomas: A Distinct Subtype of Nf2-Mutant Tumors, 2015. Yale Medicine Thesis Digital Library. 1947.
- FIG 4.
Chart illustration of the grading of meningiomas according to the 2016 WHO classification scheme and the changes made in the 2021 CNS5 classification, with the CNS5 addition of new molecular entities for grading and removal of a few grade 3 histologic subtypes.
- FIG 5.
Transcalvarial frontal atypical, grade 2 meningioma in a 54-year-old man. Sagittal T1-weighted (A) and contrast-enhanced (B) images reveal a large frontal convexity meningioma with intraosseous components and transcalvarial extension into the scalp (B, arrow). Mild hyperostosis of the adjacent calvaria along with a “hair-on-end” periosteal reaction along the outer table is seen on CT (C, arrow). Tumor shows meningothelial morphology, with, however, other features such as focal spontaneous necrosis (D, asterisk) and peripheral nests of tumor cells (D, arrows). A high Ki-67 rate in hot spot areas and areas of tumor that are devoid of progesterone receptors is also noted, supportive of the diagnosis of atypical meningioma (WHO grade 2). Mitotic count of 4 mitoses per 10 high-power fields is noted, on its own fulfilling the criteria for a diagnosis of an atypical meningioma.
- FIG 6.
An anaplastic (malignant) grade 3 meningioma along the right middle cranial fossa floor. Coronal T2-weighted (A) and coronal and axial contrast-enhanced (B and C) images depict the meningioma with strongly suggestive imaging features of parenchymal invasion, including poor interface between the tumor and cortex (A, arrow) and nodules as foci of cortical enhancement (B and C, white arrows) along with linear leptomeningeal enhancement (B, black arrow). Histopathology shows frank anaplasia cells with numerous pleomorphic cells giving this tumor a sarcomatoid appearance (D, arrows) with a grade 3 classification. Mitotic count of 22 mitoses per 10 high-power fields was noted, on its own fulfilling the criteria for the diagnosis of an anaplastic meningioma.
- FIG 7.
Right intraorbital CNS WHO grade 3 meningioma with activation of the TERT promoter. A meningioma is initially classified as grade 2 (atypical) based on histopathologic features; however, it was upgraded to grade 3 on the basis of detection of TERT activation on chromosomal microarray. Preoperative contrast-enhanced MRI at presentation (A) and at 6 months’ follow-up (B) reveals rapid enlargement of the intraorbital meningioma (arrows). The patient had multiple postoperative recurrences during the next 18 months. Preoperative contrast-enhanced MRI (C and D) performed at 3-month intervals shows rapid enlargement of recurrent enhancing tumor along the orbital roof (C and D, arrows).
- FIG 8.
Histologic grade 1 skull base meningiomas in 2 different patients (patients A and B) with upgrading to grade 3 (anaplastic) in patient B based on CDKN2 deletion. Axial (A) contrast-enhanced MRI in patient A reveals a left middle cranial fossa meningioma (arrow) with no recurrence and minimal residual activity on the 1-year postresection follow-up DOTATATE scan (B, arrow). A right sphenoid wing meningioma with intraorbital extension is seen on axial contrast-enhanced MRI (C, arrow) in patient B. Tumor recurrence was noted at the 1-year postresection follow-up DOTATATE scan (D, arrows), consistent with high-grade morphology. Despite histologic grade 1, the meningioma was upgraded to grade 3 (anaplastic) on the basis of identification of a CDKN2 deletion.
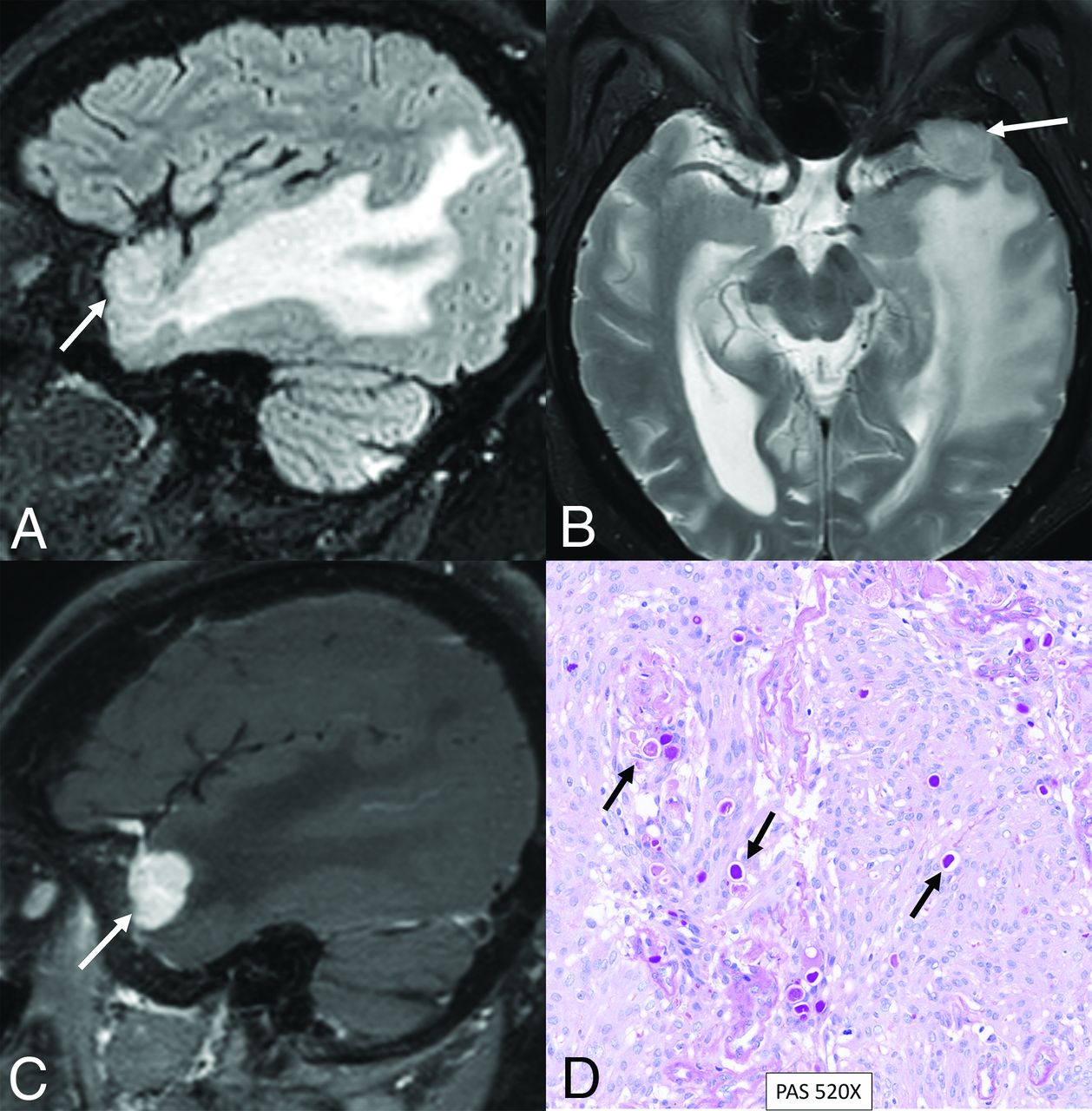
- FIG 9.
Secretory meningioma with a TRAF7 mutation in a 71-year-old woman. Sagittal FLAIR (A), axial T2-weighted (B), and sagittal contrast-enhanced (C) images reveal a small meningioma along the left greater wing of the sphenoid bone (arrows). Extensive parenchymal edema is noted in the right temporal lobe, disproportionate to the size of the meningioma. Histopathology revealed a secretory histologic subtype, with clusters of eosinophilic globules highlighted by pseudopsammoma bodies (D, arrows) with low mitotic activity (<1 mitosis in 10 high-power fields) and no atypical features, supporting a CNS WHO grade 1 designation. Next-generation sequencing studies demonstrated a pathogenic variant in TRAF7 (c.1136-1G>A).
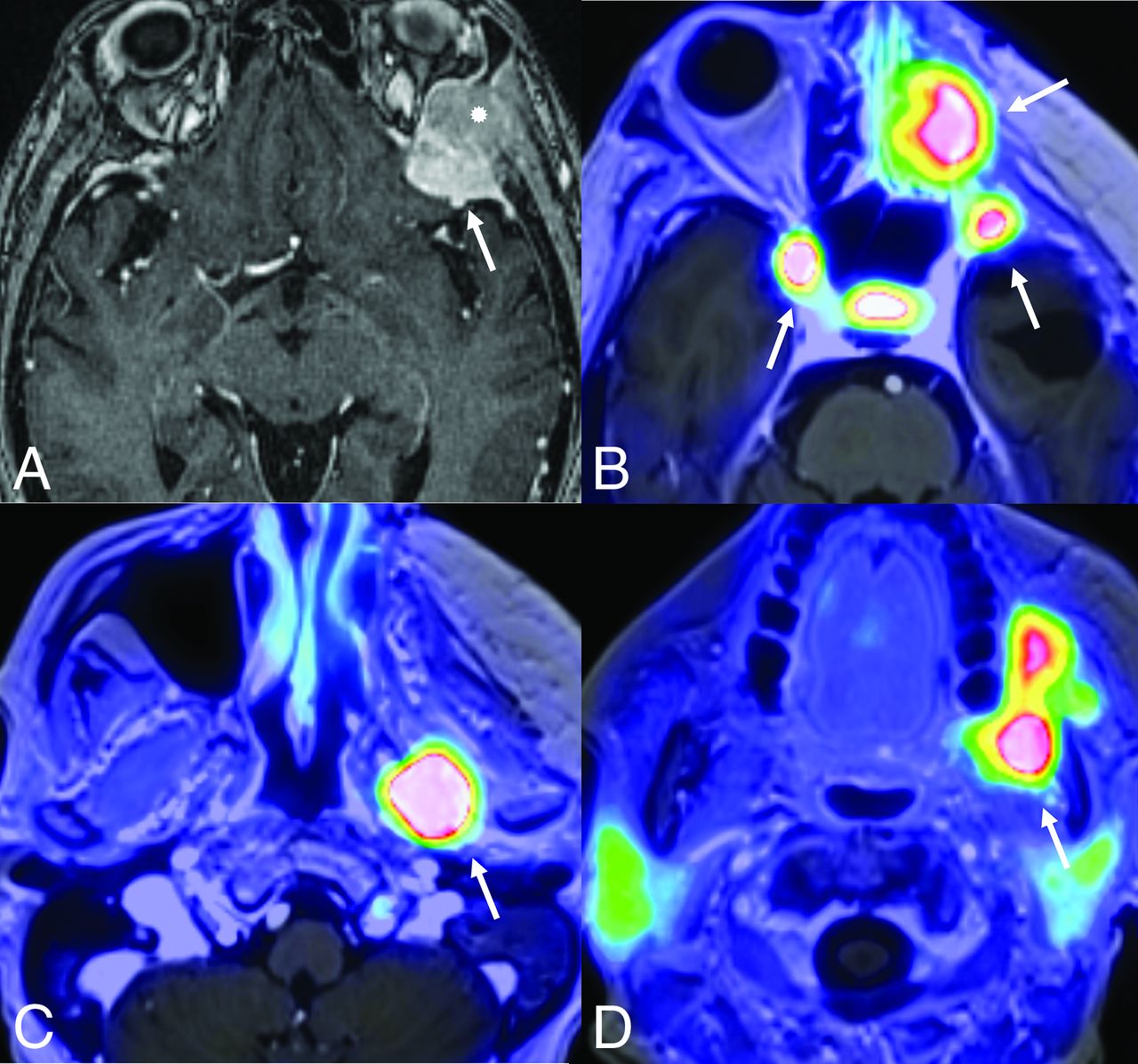
- FIG 10.
Rapid multifocal recurrence of CDKN2A/B-deleted CNS WHO grade 3 meningioma along the left sphenoid wing. The meningioma was initially classified as grade 2 (atypical) on the basis of histopathologic features; however, it was upgraded to grade 3 on the basis of detection of a homozygous deletion of CDKN2A/B on next-generation sequencing. Contrast-enhanced axial MRI depicts the left sphenoid wing meningioma (A, arrow) with intraosseous extension (asterisk). Rapid multifocal recurrence is noted on PET (DOTATATE) MRI (B–D, arrows) within a few months postresection.










Tables
Commonly identified germline and somatic mutations in meningiomas with corresponding WHO grade, location, and clinical significance
Genetic Mutation Name WHO Grade Typical Location Clinical Significance NF2 1−3 Parafalcine, posterior fossa–falcotentorial Most common70% of fibroblastic and transitional meningiomasSporadic mutations present in 40%−60% of meningiomas50%−75% of patients with germline mutations develop meningiomasAssociated with larger, more aggressive course TRAF7 1−3 Central and lateral skull base 2nd most commonSecretory subtypeHigh likelihood of hyperostosisMeningiomas tend to be benign, chromosome-stable TERT 3 Any location Commonly seen in higher grade, particularly grade 3Associated with shorter time to progression, shorter overall survival, and higher recurrence CDKN2A/B 3 Any location Mutations associated with shorter time to recurrenceClassification criteria for WHO grade 3 meningiomas SMO/SUFU 1 Olfactory groove meningiomas, anterior skull base Higher recurrence rates among olfactory groove meningiomasLarger tumor volume among anterior skull base meningiomasLinked to development of isolated familial and multiple meningiomas KLF4 1 Central and lateral skull base Secretory subtypeLarger peritumoral brain edemaResults in up-regulation of HIF-1a pathwayMay respond to mTOR inhibition POLR2A 1 Parasellar/tuberculum sellae Found almost exclusively in WHO grade 1 meningiomas (meningothelial) AKT1 Anterior and middle skull base, posterior fossa MeningothelialMutations occur with higher frequency among skull base meningiomasAssociated with shorter time to recurrence PIK3CA 1–3 Anterior and middle skull base Low recurrence riskProgesterone and cyproterone antiandrogen therapy show higher PIK3CA mutation rates in skull base meningiomas Hedgehog Midline anterior skull base Low-grade and less aggressive SMARCB1SMARCE1 1–3 Parafalcine and lateral skull base Clear cell typeSMARCB1 has been linked to multiple meningiomasSMARCE1 mutations linked with familial multiple spinal meningiomasHigher recurrence risk, faster growth BAP1PBRM1 3 Rhabdoid and papillary subtypesAggressive clinical behavior (consistent with CNS5 WHO grade 3) Note:— HIF-1-α indicates hypoxia-inducible factor 1.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.