
Article Figures & Data
Figures
- FIG 1.
Simultaneous AAT-PET MR imaging acquisition protocol. Min indicates minute; UTE, ultrashort echo time; vol, volume; SUV, standardized uptake value.
- FIG 2.
A 12-year-old boy presented with right focal seizures for a month. Electroencephalography was noncontributory. Imaging-based diagnosis of a tuberculoma was made on the initial contrast-enhanced MR imaging in November 2019. Antitubercular treatment was started empirically. Follow-up MR imaging in February 2022 showed an interval increase of the mass from approximately 1.5 × 1.3 cm to 3.8 × 3.6 cm (images not shown), which led to further work-up, and the patient underwent AA-PET MR imaging and FDOPA-PET MR imaging. T2 FLAIR (A) demonstrates a hyperintense left posterior frontal mass with equivocal diffusion restriction on the diffusion-weighted image (B and C, blue arrow). A predominantly nonenhancing mass with small peripheral nodular enhancement is seen on postcontrast T1-weighted image (D, blue arrow). No apparent increased regional CBV is seen on DSC PWI (E, white arrow). On FDOPA-PET (F, blue arrow) and fused FDOPA-PET MR imaging (G, white arrow), the lesion showed uniformly increased DOPA uptake throughout with a high maximum standard uptake value of 3.62 (lesion/striatum ratio of 1.81 versus <1.0 as normal) and TBR. Multivoxel MRS (H) showed Cho/NAA and Cho/Cr ratios of 2.78 and 1.4, respectively, with a prominent lactate peak. In this patient, FDOPA-PET MR imaging confirmed the precise diagnosis of neoplastic etiology, which, on biopsy, was revealed to be an anaplastic astrocytoma. CE indicates contrast-enhanced.
- FIG 3.
A 43-year-old man treated for a left anterior temporal lobe glioblastoma (IDH wild-type) status post resection (positive for generalized paroxysmal fast activity, negative for p53 and IDH1, MIB1 labeling index = 10%–12%, fluorescence in site hybridization epidermal growth factor receptor amplification, and no loss of 1p19q) and chemoradiation. He underwent follow-up FET-PET MR imaging after 3 years. T2 FLAIR (A, blue arrow) image shows postsurgical changes in the left anterior temporal lobe with peripheral nodular enhancement on the postcontrast T1-weighted image (B), mild increased diffusion restriction (C), and increased perfusion (rCBV of 6.7). Multivoxel MRS (E) shows noisy spectra with mildly raised choline and an inverted lactate peak. Corresponding increased FET uptake (TBR = 2.8; maximum standard uptake value = 3.7) on FET-PET (F) and fused FET-PET MR imaging (G, white arrow). The patient underwent resection, and pathology showed a recurrent tumor. This case highlights the congruent findings on contrast-enhanced MR imaging and FET-PET with a larger TBR leading to less interobserver variability and improving diagnostic performance for differentiating recurrence from TRC. CE indicates contrast-enhanced.
- FIG 4.
A 35-year-old man was initially diagnosed with left frontal lobe oligodendroglioma grade II, status post resection and chemoradiation in 2008. He underwent a follow-up [18F] DOPA-PET MR imaging. T2 FLAIR axial (A) and coronal (B) images demonstrate a large cortical and subcortical area of abnormal T2-FLAIR hyperintensity in the left parasagittal frontal lobe extending to the left gangliocapsular area and the corpus callosum and across the midline in the right parietal region without apparent diffusion restriction (C), enhancement (D), and increased rCBV perfusion (E). Multivoxel MRS (F) shows increased Cho/Cr and Cho/NAA ratios (1.86 and 2.31, respectively). FDG-PET MR imaging (G and H) shows no appreciable FDG uptake. FDOPA-PET MR imaging shows areas of significant DOPA tracer uptake (maximum standard uptake value = 1.54 versus <1.0 as normal) more prominently in the left paramedian frontal region. FDOPA-avid, FDG-nonavid nonenhancing lesion in the left frontal region involving the corpus callosum with positive MR imaging correlates suggests active underlying residual/recurrent disease. This case again highlights the superiority of AATs over FDG and the importance of multiparametric MR imaging over individual sequences. AAT uptake in the absence of contrast enhancement and increased perfusion helped with the planning of surgery and radiation. CE indicates contrast-enhanced.
- FIG 5.
A 35-year-old man was treated for left frontal glioma (grade II), status post surgical resection and chemoradiation in 2009. He underwent a reoperation in February 2018 for tumor recurrence. In June 2019, [18F] DOPA PET MR imaging (A–C) showed a postresection surgical cavity in the left anterior parasagittal basifrontal region without nodular enhancement or any increased focal FDOPA uptake. There was no evidence of recurrence. In June 2020, follow-up [18F]-DOPA PET MR imaging (D and E) showed a new focal nodular enhancing lesion in the left basifrontal area (arrow) on the postcontrast T1-weighted image (D), with mildly increased rCBV perfusion (E) and corresponding increased FDOPA uptake on fused FET-PET MR imaging (F) (maximum standard uptake value = 3.9; lesion/striatal ratio; 1.38; <1.0 as normal), suggesting recurrence. The patient underwent a reoperation with recurrence found. This case also highlights the congruent findings on contrast-enhanced MR imaging and FDOPA-PET in differentiating TRC from recurrence. CE indicates contrast-enhanced.
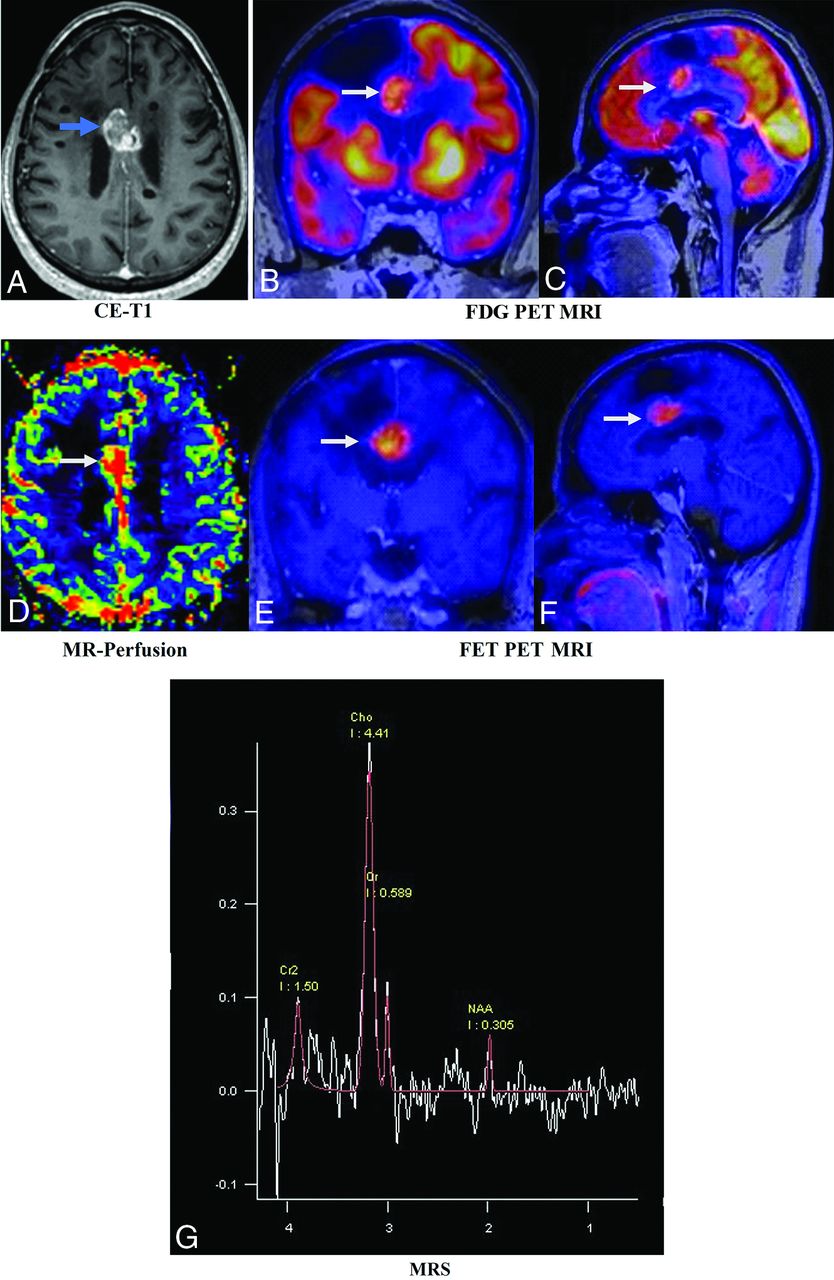
- FIG 6.
A 37-year-old man with a known diagnosis of oligodendroglioma, status post resection and chemoradiation. Postcontrast T1-weighted image (A, blue arrow) shows a recurrent enhancing lesion along the inferomedial aspect of the resection cavity of the right frontal region involving the body of the corpus callosum. Fused-PET MR images (B and C) show intralesional increased FDG slightly higher than in the white matter and lower than in the gray matter with increased rCBV perfusion (D, white arrows). Fused FET-PET MR images (E and F) show a relatively larger volume of a recurrent lesion, allowing better estimates of the extent of the lesion. Multivoxel MRS (G) shows an increased choline peak and decreased NAA peak. The pathologic diagnosis was a recurrence. This case highlights the superiority of AAT over FDG, congruent findings on MR imaging and FET-PET, and an excellent TBR, which were helpful in radiation therapy planning and re-surgical resection. CE indicates contrast-enhanced.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.