
Article Figures & Data
Figures
- FIG 1.
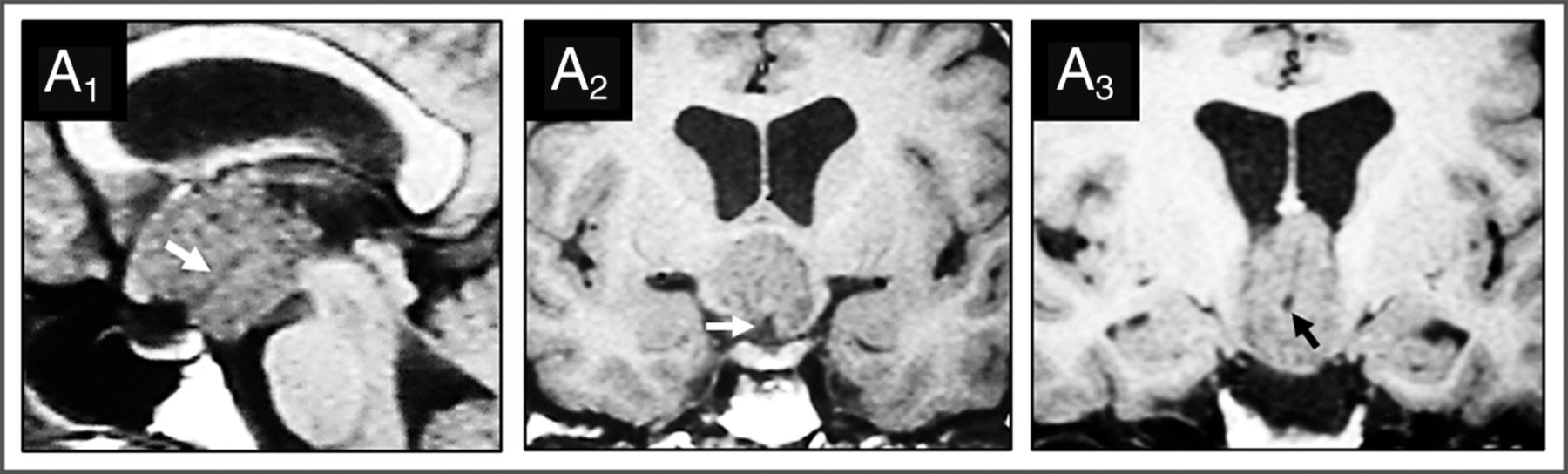
Basal recess in strictly 3V CPs of the papillary type: MR imaging evidence in 1 case identified from our series. Case 1 (Online Supplemental Data): This papillary CP was diagnosed in a 34-year-old woman with headaches, Fröhlich syndrome, poikilothermy, and emotional lability. Preoperative T1WI shows this strictly 3V homogeneously isointense lesion above the intact 3VF, with papillomatous excrescences at its surface. On the midsagittal (A1) and coronal (A2, A3) scans, a long basal recess can be identified as a tube-like hypointense structure extending from the suprasellar cistern to the center of the tumor (white arrows, A1 and A2; black arrow, A3).
- FIG 2.
Epidemiologic, pathologic, and topographic characterization of the 52-craniopharyngioma cohort with a basal recess (CP-DR cohort). A, Bar chart shows the age distribution. Observe that no cases were diagnosed in the first decade. About 65% of cases occurred in adults between 30 and 60 years of age. B, Stacked bar chart comparing the distribution of histologic CP types between the CP-DR and the CP-nDR cohorts. All tumors with a DR belonged to the squamous-papillary type, only diagnosed in 23% of CPs without a DR in the adult CP population (P < .001). C, Stacked bar graph comparing tumor consistencies. Most CP-DR tumors had a homogeneous solid consistency (90%), whereas a mixed solid-cystic pattern was predominant among ACPs without a DR (61.5%) (P < .001). D, Topographic distribution of tumors. More than 80% of papillary CPs with a DR corresponded to strictly 3V tumors located above an anatomically intact 3VF. No CP-DR lesions originated at the sellar or suprasellar compartments below the 3VF (P < .001).
- FIG 3.
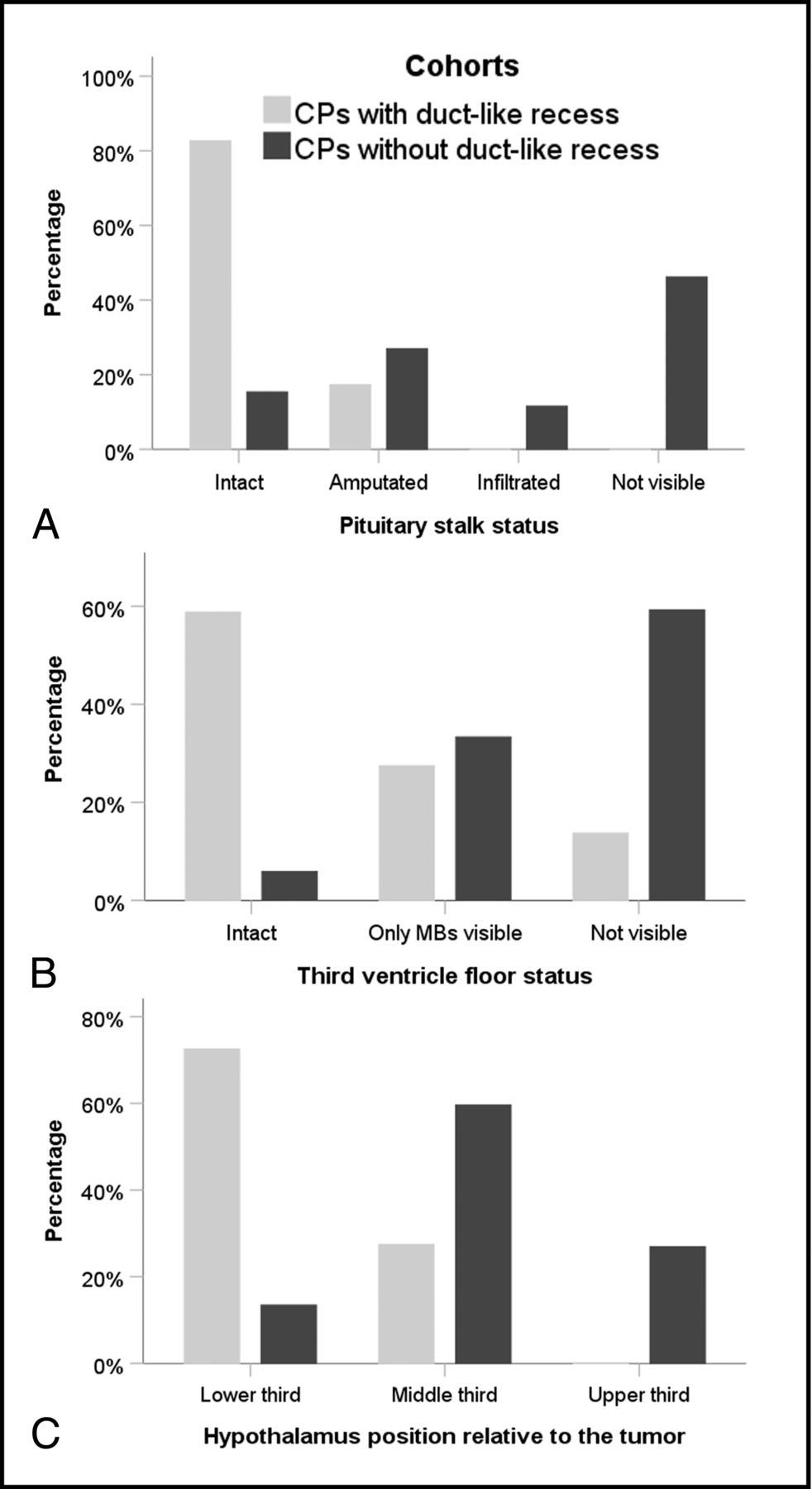
MR imaging characterization of the anatomic relationships between the tumor and the 3V in CPs with or without a DR. A, PS status. Among the lesions in the CP-DR cohort, the PS is observed intact under the basal recess (85%), whereas it is wholly or partially engulfed by the tumor in about 85% of adults with CPs without a DR (P < .001). B, Anatomic status of the 3VF. An intact 3VF was observed in 60% of CPs with a DR, whereas this structure cannot usually be distinguished from the tumor boundaries in CPs without a DR (P < .001). C, Bar graph shows the distribution of hypothalamus positions relative to the tumor. In almost 75% of papillary CPs with a DR, the hypothalamus is located around the lower third of the lesion. In contrast, it is observed encircling its central portion in 60% of adult CP cases without a DR (P < .001). MBs indicates mamillary bodies.
- FIG 4.
Basal recess at the infundibular portion of 3V papillary craniopharyngiomas. MR imaging characterization in seminal cases from the medical literature (A1–A2). Diverticulum-like recess at the base of a strict 3V papillary CP identified on preoperative MR imaging (Online Supplemental Data). On the midsagittal T1WI (A1), the hypointense recess (black arrowhead) is open at the suprasellar cistern and extends to the tumor center, following the same trajectory as the PS. The coronal-transinfundibular MR image (A2) shows the hypointense signal of the recess identical to CSF, indicating free passageway of CSF between the suprasellar cistern and the recess and the rounded dead end of the recess at the tumor center. Reproduced with permission from the Fukushima et al.8 B, Duct-like long-recess type in a strict papillary CP (Online Supplemental Data). This midsagittal T2WI shows the hyperintense signal of the duct, identical to that in the CSF (white arrow). Reproduced with permission Gu et al.21 C, Coronal-transinfundibular T1WI of a short-type basal DR in a strict 3V PCP (Online Supplemental Data). Note the isointense rim of the 3V floor covering the undersurface of this solid homogeneously gadolinium-enhancing tumor and how the 3VF invaginates at the midline of the basal pole of the CP to form the recess (white arrow). Reproduced with permission from Rambarki and Rajesh.22 PG indicates pituitary gland; MB, mammillary body; OC, optic chiasm.




Tables
Differential characteristics between the CP-DR on MR imaging and a cohort of adults with CPs without such a structure
CP Characteristics Categories CP-DR (n = 52) Adult CP-nDR (n = 52) P Value Sex Male 73% 50% .012 Female 27% 50% Hydrocephalus Present 71% 25.5% <.001 Headache Present 75% 49% .01 Visual deficits Present 51% 73.5% .032 Endocrine deficits Present 38.5% 39% NS Hypothalamus disturbances Present 20.5% 0% .001 Mental alterations Present 58% 12% <.001 HTIC Sd Present 72% 41% .002 Hypothalamic Sd Present 67.5% 26.5% <.001 Tumor histology Squamous-papillary 100% 23% <.001 Adamantinomatous 0% 77% Tumor topography Sellar/suprasellar 0% 40% <.001 Infundibulo-tuberal 4% 41% Strictly 3V 96% 19% Calcifications Present nodular 0% 58% <.001 Tumor consistency Pure solid 90% 17% <.001 Cystic-cauliflower 10% 4% Pure cystic 0% 17.5% Mixed solid-cystic 0% 61.5% Sella turcica Occupied by tumor 0% 31% <.001 PS status Intact 84.5% 15.5% <.001 Lower portion visible 15.5% 27% Infiltrated/invaded 0% 57.5% Suprasellar cistern status Tumor-free 44% 31% .001 Partially occupied 54% 32.5% Wholly occupied 2% 36.5% Hypothalamus position Around CP lower third 74.5% 13.5% <.001 Around CP middle third 26.5% 60% Around CP upper third 0% 26.5% 3VF status Visible intact 61% 6% <.001 Only MBs visible 27.5% 33% Not visible 11.5% 61% Note:—HTIC indicates high intracranial pressure; MBs, mammillary bodies; NS, not significant; Sd, syndrome.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.