
Article Figures & Data
Figures
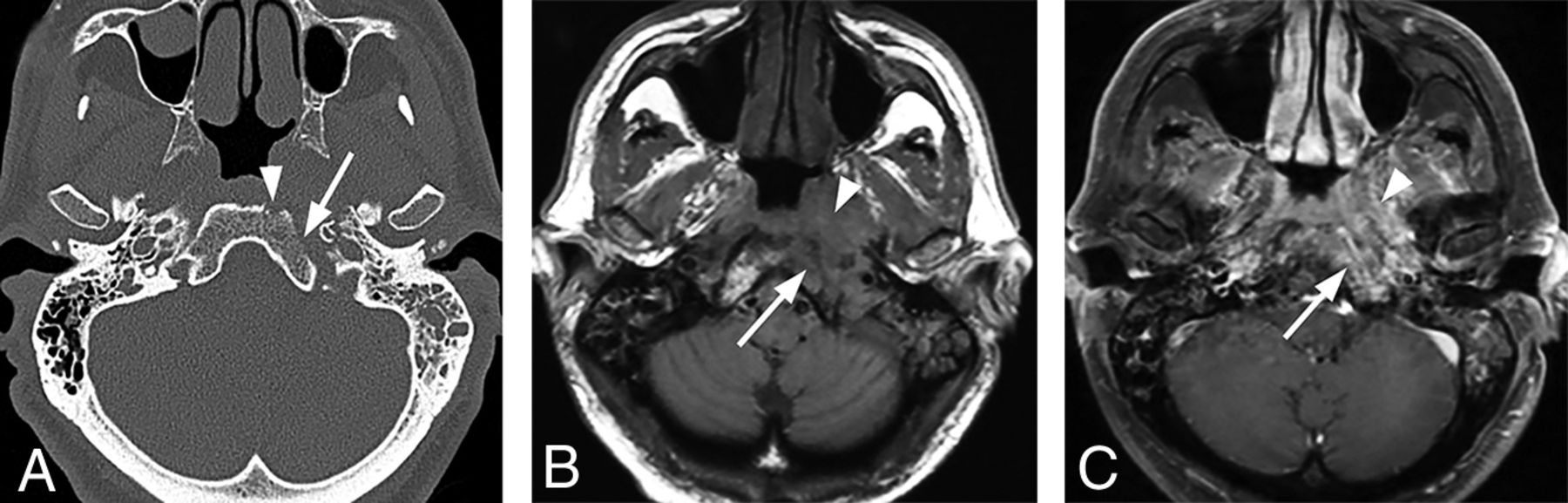
- FIG 1.
Typical skull base osteomyelitis. A 55-year-old man with type 2 diabetes with low-grade fever, severe pain, and drainage from his left ear. Eight weeks before imaging, the patient had been diagnosed with left-sided otitis media and possible otitis externa. He had initially been treated with amoxicillin and ofloxacin drops, without improvement. Culture from left-ear drainage revealed methicillin-sensitive S aureus. The patient was treated with IV vancomycin and piperacillin/tazobactam for 2 weeks and then 14 weeks of amoxicillin/clavulanate. All clinical and laboratory parameters initially resolved during 4 months. However, a gallium scan continued to indicate abnormal activity of the skull base at both 8 and 16 weeks. Despite the gallium scan, antibiotics were discontinued. Within 2 weeks, the patient had recurrent symptoms and severe neck pain. Additional imaging (not shown) indicated new cervicocranial septic arthritis, requiring an additional 3 months of IV antibiotics that led to a cure. A, Axial CT demonstrates opacification of left-mastoid air cells. There is subtle erosion along the petro-occipital fissure (arrow) and loss of cortical bone along the left lateral margin of the clivus (arrowhead). B, Axial unenhanced T1-weighted MR image demonstrates abnormal signal in the marrow space of the basiocciput (arrow), ill-defined signal in the left carotid space, and masslike submucosal infiltration of the left nasopharynx (arrowhead). C, Axial T1-weighted fat-saturated contrast-enhanced image demonstrates abnormal enhancement involving the marrow space of the clivus (arrow) as well as heterogeneous enhancement of infiltrating soft tissue in the left nasopharynx (arrowhead).
- FIG 2.
Atypical skull base osteomyelitis. A 72-year-old man with history of hypertension presented with a 9-week history of sinus congestion, rhinorrhea, and headache. The patient had been treated for severe sinusitis with several courses of oral antibiotics and steroid injections prescribed by his primary care physician as well as community ear, nose, and throat physicians. Just before admission, he developed left hearing loss and left-sided facial palsy. Swab culture of the nasopharynx revealed P aeruginosa. The patient was treated with amoxicillin-pot clavulanate (Augmentin) and Ceftazidime (Ceftaz) with clinical resolution after several weeks. Follow-up MR imaging at 4 months confirmed improvement. A, Axial contrast-enhanced CT scan demonstrates patchy heterogeneous density in the preclival soft tissues extending to involve the carotid spaces bilaterally (arrows). The inflammatory tissues in the preclival soft tissues could mimic an infiltrative neoplasm of the nasopharynx. B, Axial bone CT at the same level shows irregular erosions of the ventral clivus (arrows). C, Axial T1-weighted contrast-enhanced MRI. There is nodular enhancement involving the clivus at this level with focal areas of necrosis and abscess just inferior to the foramina lacerum (arrow). Note circumferential enhancement of the petrous internal carotid arteries (arrowhead). D, Axial DWI depicts small foci of fluid near the foramen lacerum bilaterally as diffusion-restricted, consistent with focal abscesses (arrows).
- FIG 3.
Bilateral external otitis. A 44-year-old woman presented with severe bilateral ear pain and drainage with conductive hearing loss. Clinically, there was marked inflammatory thickening of the EACs bilaterally. Pseudomonas species were cultured from the external auditory canals bilaterally. The patient was treated with IV vancomycin and piperacillin/tazobactam for 4 days followed by 2 weeks of oral ciprofloxacin. Symptoms resolved at 3 weeks without additional imaging work-up. A, Axial enhanced CT images are shown. Upper image with bone windows shows marked opacification of the EACs (arrows). The lower image with a soft-tissue filter shows marked inflammation of the EACs and periauricular tissues (arrowheads). B, The upper coronal T1 image shows marked opacification and thickening of the EACs (arrows) and associated opacification of the middle ear cavities. The lower image depicts postcontrast fat-saturated T1 images. A discrete mass is not identified. However, there is marked enhancement along the walls of the EACs (arrowheads), compatible with otitis externa.
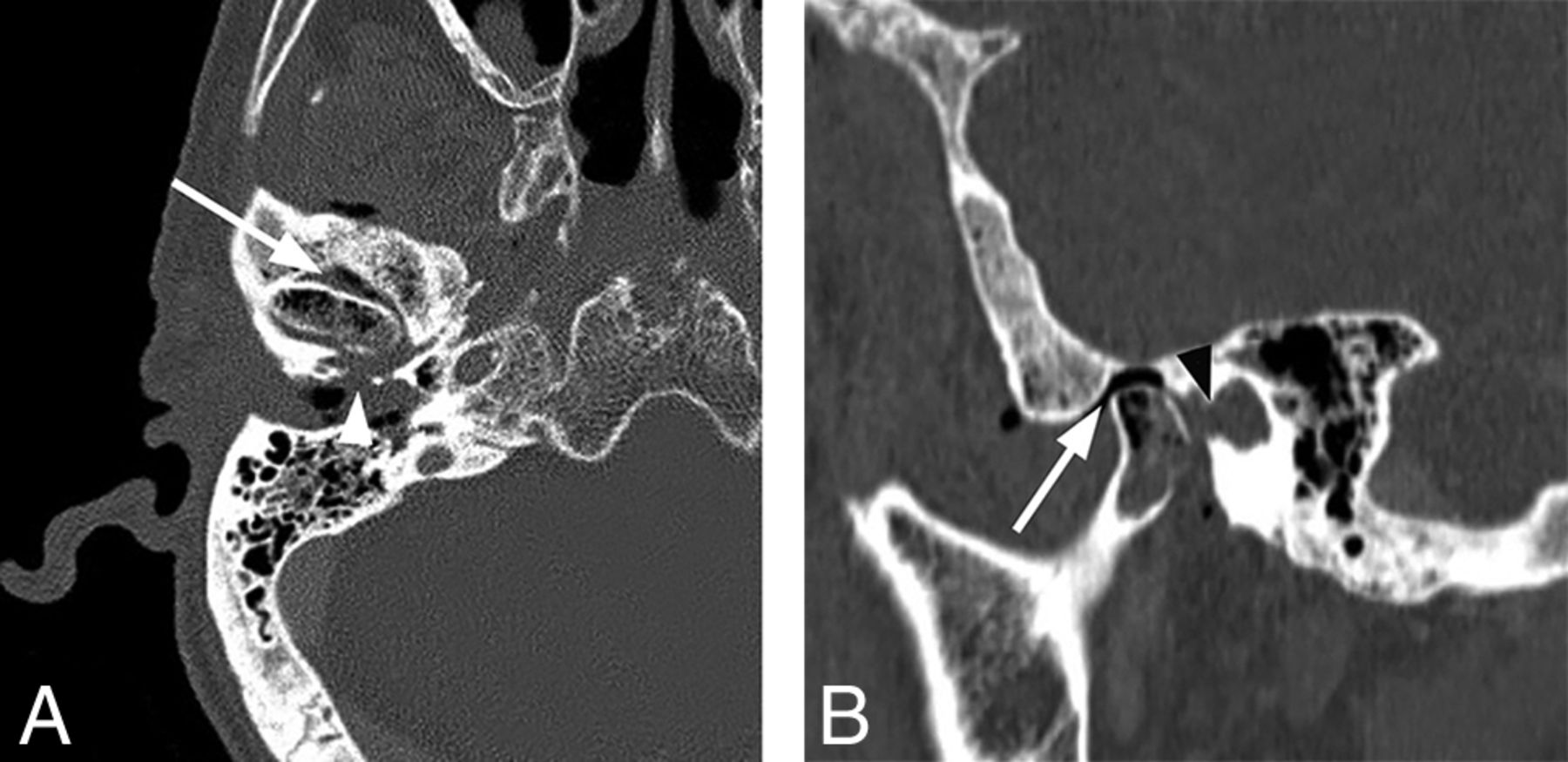
- FIG 4.
Necrotizing external otitis complicated by septic temporomandibular joint arthritis. An 88-year-old man with several months of right ear pain and drainage presented with progressive symptoms and right temporomandibular joint pain and trismus. In the prior weeks, he had been treated for NEO with oral and IV antibiotics at an outside facility. After initial evaluation, debridement and temporomandibular joint replacement were planned, but the patient was lost to follow-up. A, Axial contrast-enhanced CT with bone windows demonstrates abnormal opacification of the right EAC and inferior middle air cavity. There is erosion of the floor of the EAC, potentially involving the foramen of Huschke (arrowhead), and communication with the right temporomandibular joint. Air/gas density is identified within the temporomandibular joint (arrow) as well as within the mandibular condyle itself. B, Sagittal reformatted CT scan again demonstrates abnormal air density within the right temporomandibular joint and mandibular condyle (arrow). Note a defect in the anterior inferior margin of the EAC (black arrowhead).
- FIG 5.
Typical SBO from NEO. An 82-year-old woman with insulin-dependent diabetes presented with a several-month history of pain and drainage from the right ear. The patient was recently treated as an outpatient with several rounds of antibiotics (including amoxicillin/clavulanate and ciprofloxacin) for otitis media and NEO, but symptoms had progressed. Following imaging and a diagnosis of SBO, the patient was treated with 4 weeks of IV vancomycin and piperacillin/tazobactam and additional 4 weeks of oral ciprofloxacin. The patient initially had clinical improvement, but a gallium scan at 8 weeks showed persistent uptake. The patient did not return for follow-up as instructed but returned 8 months after the original admission with progressive infection extending to the central skull base and left temporal bone, requiring an additional 6 weeks of IV antibiotic treatment. A, Axial CT scan through the right EAC demonstrates thickening and partial opacification of the external auditory canal (arrow). There is subtle erosion along the posterior wall of the external auditory canal and mild soft-tissue fullness of the right nasopharynx. B, Axial T1-weighted MR image demonstrates obliteration of normal fat planes in the submucosal and preclival tissues of the nasopharynx (arrows). This process extends posterolaterally to the tip of the mastoid on the right. C, Axial T1-weighted contrast-enhanced image demonstrates heterogeneous enhancement of abnormal tissue extending from the tip of the mastoid on the right to the nasopharynx (arrows) without discrete abscess formation.
- FIG 6.
Extensive atypical skull base osteomyelitis secondary to invasive fungal sinusitis (mucormycosis). A 68-year-old man with insulin-dependent diabetes mellitus and a history of chronic sinusitis and previous sinus operations presented with a 6-month history of severe headache, nausea and vomiting, and weight loss. Endoscopic debridement and biopsies were performed. While cultures were negative for fungus, pathologic evaluation of sinus material yielded microscopic evidence of invasive fungal sinusitis consistent with mucormycosis. The patient was treated with micafungin and amphotericin B. A protracted course was complicated by persistent symptoms, and the patient had additional sinonasal debridement at 4 months. Endoscopic culture at that time yielded P aeruginosa as a new or potentially coexistent organism, and IV ceftazidime was added to treatment. The patient was followed clinically and with CT/MR imaging until resolution. A, Axial unenhanced CT image through the skull base demonstrates diffuse osteolysis and fragmentation of the sphenoid bone, including the walls of the sphenoid sinus and greater wing (arrows). There is marked mucosal thickening and opacification of the visualized sinuses. B, Axial CT image through the central skull base shows diffuse bone demineralization of the body of the sphenoid bone (arrows). C, Axial T1-weighted fat-saturated contrast-enhanced image shows abnormal enhancement in the greater wings of the sphenoid bone bilaterally (arrows) and confluent opacification of the sinuses. There is evidence of devitalization and necrosis in the upper clivus (arrowhead). D, Axial T1-weighted fat-saturated contrast-enhanced image shows marked infiltrative signal abnormality and enhancement in the greater wings of the sphenoid bone (arrows). There is marrow necrosis and devitalization of the body of the sphenoid bone centrally (arrowheads). E, Axial fused Tc99m MDP bone scan SPECT image shows marked radiotracer uptake in the greater wing of the sphenoid bone on the left and the anterior midline skull base, consistent with osteomyelitis. F, Axial fused Tc99m MDP bone scan SPECT image shows multifocal areas of radiotracer uptake in the sphenoid bone bilaterally.
- FIG 7.
Typical SBO with atypical organisms. A 75-year-old man with diabetes presented with left-ear discharge, conductive hearing loss, and headache. Initial imaging suggested an infiltrative neoplasm of the nasopharynx, and multiple endoscopic biopsies of the nasopharynx were performed to exclude nasopharyngeal carcinoma. Ultimately, biopsies of the external auditory canal revealed an infectious organism, Aspergillus species. The patient was treated with amphotericin with gradual resolution of symptoms. A, Axial enhanced CT image through the level of the nasopharynx suggests an infiltrative soft-tissue abnormality involving the submucosa and preclival soft tissues of the nasopharynx (arrow). B, Axial T1-weighted MR image through the nasopharynx shows poorly defined infiltrative soft tissue (arrowhead) in the submucosa of the nasopharynx on the left, extending to involve the left carotid space. There is also replacement of normal marrow on the left side of the basiocciput (arrow). C, Axial enhanced fat-saturated T1 image through the nasopharynx demonstrates abnormal enhancement on the left side of the occipital bone (arrow) as well as abnormal enhancing infiltrative tissue (arrowheads) in the preclival soft-tissue left carotid space and left retromandibular region. Courtesy of Dr Christine Glastonbury, Professor of Clinical Radiology, Otolaryngology Head and Neck Surgery, and Radiation Oncology, University of California, San Francisco, California.
- FIG 8.
Extensive skull base osteomyelitis. A 70-year-old man with poorly controlled diabetes presented with symptoms of otomastoiditis with associated hearing loss, left facial nerve paralysis, and dysphagia. A culture of the left external auditory canal revealed Pseudomonas infection. The patient received aggressive treatment for several months, including IV vancomycin and piperacillin/tazobactam, but he ultimately died from meningitis and aspiration pneumonia. A, Axial CT demonstrates multiple focal areas of cortical dehiscence involving the temporal bones bilaterally as well as the clivus (arrowheads). The generalized erosion is compatible with diffuse osteomyelitis of the skull base. B, Axial fused Tc99m MDP bone scan SPECT image demonstrates significant accumulation of radiotracer in the skull base bilaterally, preferentially affecting the temporal bones. C, An axial fused gallium scan SPECT image shows bilateral accumulation of radiotracer in the temporal bones, with some extraosseous accumulation in the left preclival region.
- FIG 9.
Typical skull base osteomyelitis. A 63-year-old man with diabetes presented to an outside hospital with a several-month history of left ear pain. He was initially diagnosed with otitis media and treated with several rounds of antibiotics. A recent evaluation at an outside hospital suggested the presence of a nasopharyngeal mass with skull base invasion. Two separate biopsies of the nasopharynx failed to demonstrate nasopharyngeal carcinoma. While a discrete organism was not cultured, the patient was presumptively treated with levofloxacin and clindamycin with gradual improvement and resolution of all symptoms. He was monitored using serial CT, MR imaging, and gallium scans. A, Axial postcontrast CT of the soft tissue of the neck at the level of the nasopharynx demonstrates a heterogeneously enhancing soft-tissue lesion involving the submucosal region of the left nasopharynx (arrow). The process extends laterally to the left carotid space, and there is occlusion or thrombosis of the left internal jugular vein. B, Axial postcontrast CT scan through the skull base with bone windows demonstrates focal cortical erosion along the margins of the foramen lacerum (arrow), consistent with osteomyelitis. C, Axial T1-weighted MR image through the skull base shows an infiltrative process involving the left side of the clivus (arrow) and adjacent preclival tissues of the left nasopharynx. The lesion appears masslike on the left (arrowhead). The infiltrative process extends posterolaterally on the left to the jugular foramen. Partial thrombosis of the jugular bulb and sigmoid sinus is identified (black arrowhead). D, Axial enhanced T1-weighted MR image through the skull base shows an enhancing infiltrative process involving the left side of the clivus (arrow) and adjacent preclival tissues of the left nasopharynx (arrowhead). The process extends posterolaterally on the left to the jugular foramen. Partial thrombosis of the jugular bulb and sigmoid sinus is identified (black arrowhead). E, Axial DWI shows no diffusion restriction in the nasopharyngeal soft tissue, favoring a non-neoplastic process over lymphoma or nasopharyngeal carcinoma. F, Axial fused Tc99m MDP bone scan SPECT image shows localized accumulation of radiotracer in the left skull base, compatible with osteomyelitis. G, An axial fused gallium scan SPECT image at the level of the nasopharynx shows mild uptake in the soft tissues of the nasopharynx. H, A follow-up fused gallium scan SPECT image at the level of the nasopharynx demonstrates resolution of previously seen uptake in the nasopharyngeal soft tissues, favoring a treatment response.
- FIG 10.
Progressive left-sided skull base osteomyelitis. A 65-year-old man with multiple comorbidities, including poorly controlled diabetes, presented with a relatively long-standing history of chronic sinusitis and bilateral otitis media. He was recently treated for otitis media of the left ear and presented with new headache and left-sided hearing loss. Culture from the left EAC was negative for a causative organism, and cultures from the sphenoid sinus demonstrated methicillin-resistant S aureus. The patient was treated with 4 weeks of IV vancomycin and piperacillin/tazobactam. The patient improved, and a gallium scan performed during follow-up showed significant improvement and only mild residual uptake in the skull base. Antibiotics were discontinued. The patient returned 4 weeks later with sepsis, and blood cultures were positive for Klebsiella species. In the next 3 months, the patient had a return of headaches and new right-sided symptoms. Imaging evaluation demonstrated progressive infection of the right skull base. Re-institution of IV antibiotics led to gradual resolution of clinical and imaging findings. A, Axial T1-weighted MRI through the skull base shows an infiltrative soft-tissue abnormality (arrows) involving the central skull base with abnormal marrow signal on the left side of the occipital bone (arrowhead). B, Axial enhanced T1-weighted MR image shows heterogeneous enhancement in the corresponding areas of the left petro-occipital fissure (arrow). C, Axial bone scan fused with CT shows radiotracer accumulation in the left central skull base, including the sphenoid bone and left petrous apex. D, Following initiation of empiric IV antibiotic treatment, the patient had improvement of symptoms on the left, but 4 months later, he developed severe headache, fever, and right-sided facial pain. Axial T1-weighted image shows an infiltrative process (arrows) of the central skull base that now extends to the right. E, Axial enhanced fat-saturated T1-weighted image demonstrates improved enhancement of the left central skull base and the adjacent soft tissues but interval worsening of enhancement of the right skull base (arrowhead) and soft tissues of the nasopharynx (arrow). F, Follow-up axial fused bone scan SPECT image demonstrates radiologic worsening with marked radiotracer uptake in the central skull base in the right petro-occipital region.










Tables
Comparison of clinical characteristics of typical versus atypical SBO
Typical SBO Atypical SBO Age Elderly Middle-aged Predisposing factors DM more common than immunocompromised DM, immunocompromised Clinical features Otorrhea, otalgia (severe, with pain out of proportion to the physical findings), hearing loss Headache, atypical facial pain, cranial neuropathies, sinonasal symptoms in 25% Cranial nerve involvement VII most common VI, IX, and X more common than VII Pathogen P aeruginosa in most cases; fungal more common in immunosuppressed patients without diabetes S aureus slightly more common than P aeruginosa and fungal Primary epicenter of disease process EAC, petrous apex, and clivus Central skull base, sphenoid bone, or clivus with or without evidence of regional infection of the sinuses, deep face, or oral cavity Note:—DM indicates diabetes mellitus.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.