
Article Figures & Data
Figures
- Fig 1.
A 27-year-old woman with relapsed pre-B-cell acute lymphoblastic leukemia was admitted for chemotherapy. She had an MR imaging examination due to headache. Axial (A) and coronal (B) T1-weighted postcontrast images with fat saturation showed nonenhancement centered in the left middle turbinate (long arrows) with irregular and invasive borders extending into the left inferior turbinate (short arrow). The patient had tissue-proved invasive fungal rhinosinusitis and went through a series of 12 aggressive surgical debridements and eventually died.
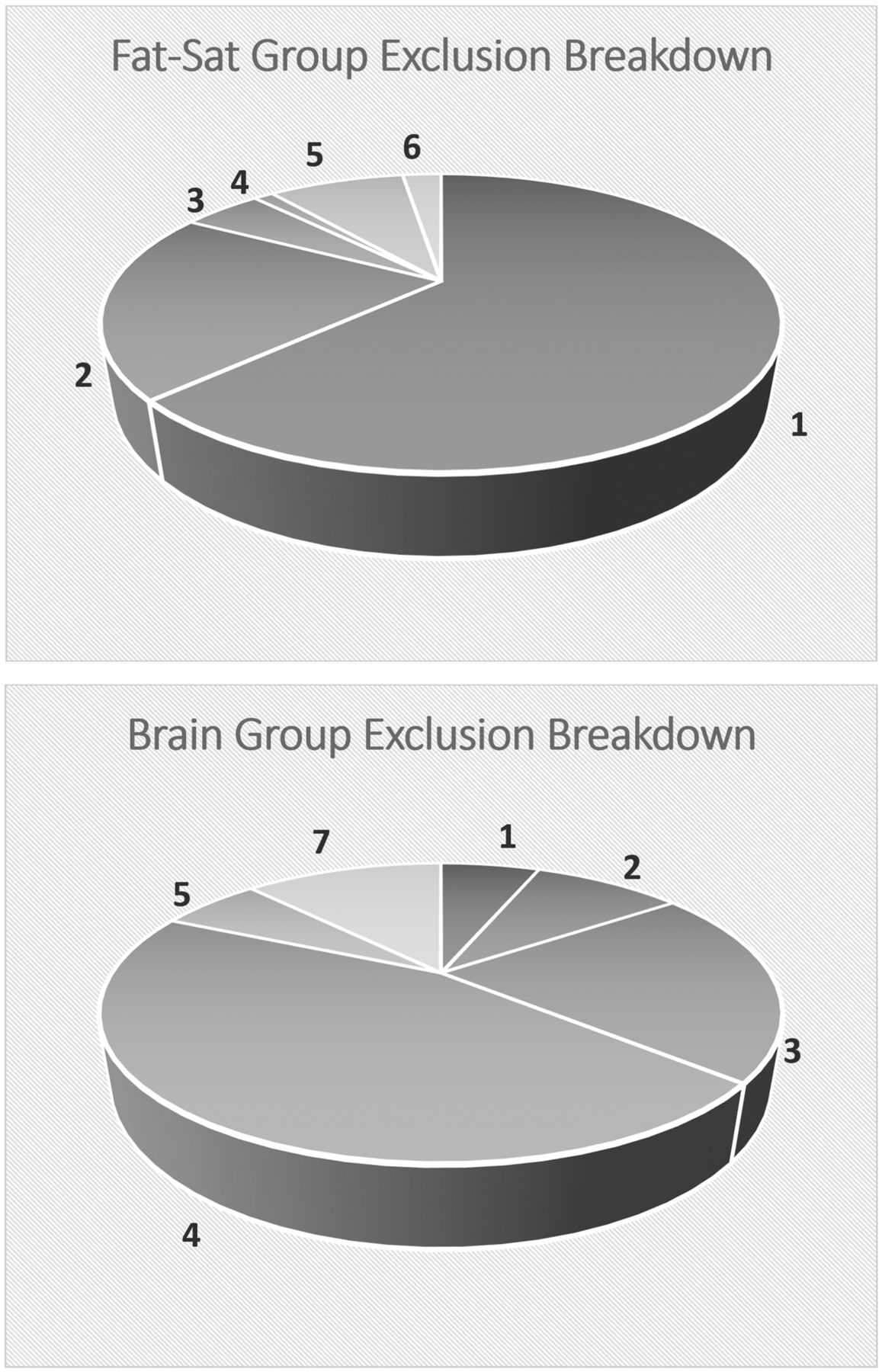
- Fig 2.
Breakdown of excluded cases: 1) insufficient inclusion of nasal turbinates, 2) significant postoperative or posttreatment changes involving the nasal cavity, 3) inappropriate scan sequence, 4) specific protocols, 5) significant motion or other artifacts, 6) significant nasal mass, and 7) scans from outside or satellite hospitals.
- Fig 3.
A 24-year-old immunocompetent woman with a history of a gestational trophoblastic neoplasm who had a brain MR imaging for a metastatic work-up. Coronal (A) and sagittal (B) postcontrast T1-weighted images show nonenhancement of the posterior aspect of the left inferior turbinate (long arrows) with thin rim enhancement (short arrows). The posterior aspect of the inferior turbinate is a common location of a black turbinate in immunocompetent patients.
- Fig 4.
A 14-year-old immunocompetent adolescent girl with right-sided blurred vision, who had orbit and brain MR imaging for a multiple sclerosis work-up. The postcontrast images for the orbit MR imaging were obtained before those for the brain MR imaging. Axial (A) and coronal (B) postcontrast T1-weighted images with fat saturation show nonenhancement most pronounced in the posterior aspects of both inferior turbinates (long arrows) with thin rim enhancement (short arrows) and scattered nonenhancing foci in the right middle turbinate (arrowhead). The inferior turbinate, especially the posterior portion, is a common location of a BT in immunocompetent patients. The sagittal postcontrast image from the brain MR imaging (C), which is the last postcontrast sequence available, shows that the BT of the right interior turbinate is almost completely resolved and has transitioned into mildly scattered nonenhancing foci (curved arrow).
- Fig 5.
Axial postcontrast T1-weighted images with fat saturation from 3 different patients. A, A 43-year-old woman shows extensive nonenhancing “dots” in both inferior turbinates, left more than right, with relative sparing of the anterior aspects, which is a typical pattern of scattered nonenhancing foci. B, A 12-year-old girl shows the more homogeneous and intense enhancement of the nasal turbinates, which is typical of pediatric patients. C, A 36-year-old woman shows relatively homogeneous enhancement, but it is less intense than that in the pediatric patient, and there are a few small nonenhancing dots (arrows).





Tables
Skyra adult protocols Orbit Axial T1 FS Coronal T1 FS Cor MPRAGE (O) Timing 04:10 04:42 04:14 Face Coronal T1 FS Axial T1 FS Sagittal T1 FS Timing 03:58 04:31 05:03 Neck Sagittal T1 FS Coronal T1 FS Axial T1 FS Timing 06:43 04:39 08:02 Skull base Axial FLAIR Axial T1 FS Coronal T1 FS Sagittal FLAIR FS Timing 01:54 06:58 06:42 02:54 Brain Axial T1 FLAIR Coronal T1 FLAIR Sagittal T1 FLAIR Timing 01:54 02:54 02:54 Verio adult protocols Orbit Axial T1 FS Coronal T1 FS Timing 03:14 01:51 Face Coronal T1 FS Axial T1 FS Sagittal T1 FS Timing 04:00 04:00 05:04 Neck Axial T1 FS Coronal T1 FS Axial T1 FS Timing 03:56 04:04 05:03 Skull base Axial T1 FS Coronal T1 FS Axial T1 Sagittal T1 FS Timing 05:13 05:13 01:41 05:07 Brain Axial T1 Coronal T1 Sagittal T1 FLAIR Cor MPRAGE (O) Timing 01:21 01:45 01:39 04:18 Note:—Cor indicates coronal; FS, fat saturation; O, optional sequence; VIBE, volume interpolated gradient echo.
↵a Skyra and Verio scanners (Siemens, Erlangen, Germany). All timing is in minutes and seconds.
Category Grades 1 2 3 Size symmetry Markedly asymmetric Mildly-to-moderately asymmetric Symmetric Degree of enhancement Less than extraocular muscle Similar to extraocular muscle Greater than extraocular muscle T2 signal intensity Similar to extraocular muscle Similar to gray matter Similar to vitreous ↵a Grading criteria for the symmetry of the size of the nasal turbinates, their overall degree of enhancement, and their signal intensity on the T2-weighted images. Scores range from 1 to 3, with scores of 1.5 or 2.5 representing the intermediate grade between 2 levels.
Grades 1 1.5 2 2.5 3 FS group (16 cases) Size symmetry 10 6 Enhancement level 12 1 2 1 T2 signal intensity 8 1 7 Brain group (29 cases) Size symmetry 3 8 1 17 Enhancement level 5 24 T2 signal intensity 10 17 2 ↵a Grading criteria for the symmetry of the size of the nasal turbinates, their overall degree of enhancement, and their signal intensity on the T2-weighted images. Scores range from 1 to 3, with scores of 1.5 or 2.5 representing the intermediate grade between 2 levels.
Groups Superior Middle Inferior Temporal-Improvingb Temporal-Transientc FS 6 16 5 11 Brain 8 28 13 16 ↵a The location of the black turbinates and the change in enhancement during multiple series are shown. Because a patient can demonstrate BT in >1 turbinate (ie, both the middle and inferior turbinates can show BT simultaneously), the total number of turbinates seen with BT is larger than the number of cases in each group.
↵b BT persists across all sequences but improves gradually.
↵c BT resolves on later sequences.
- Table 5:
Relationship of turbinate size to BT, presence of BT at 2 time points, and nasal cyclinga
Groups Cases with BT Cases with Size Asymmetry BT Seen in Smaller Turbinates Cases with Prior Exam BT Seen on Prior Exam Cases with Nasal Cycling FS 16 10 6 9 4 0 Brain 29 12 4 13 10 3 ↵a The occurrence of BT relative to turbinate size shows that BT did not primarily occur in the smaller turbinate when size asymmetry was present. Patients who had a BT on 1 scan often did not always have a BT on a prior exam. Nasal cycling indicates a change in nasal turbinate symmetry between the index and prior study. This occurred relatively infrequently.
Total Female Male P (M vs F) Pediatric Patients Adult Patients P (Adult vs Pediatric) FS group 75 40 (53%) 35 (47%) .74b 16 (21%) (6 mo to 14 yr) 59 (79%) (range, 18–81 yr) .74b Brain group 75 41 (55%) 34 (45%) .62b 17 (23%) (2 mo to 17 yr) 58 (77%) (range, 24–86 yr) 1.00b P FS vs Brain 1.00c 1.00c Note:—P indicates P value; M, male; F, female.
↵a All P values were calculated using the Fisher exact test.
↵b To compare the sex and age composition of each group with the general population, assuming even sex distribution and approximately 24% pediatric population.
↵c To compare the sex and age composition between the FS and brain groups.
Total Female Male P (M vs F) Pediatric Patients Adult Patients P (Adult vs Pediatric) FS group 16 11 (69%) 5 (31%) .28b 2 (12%) (11 and 14 yr) 14 (88%) (range, 31–74 yr) .73b Brain group 29 17 (59%) 12 (41%) .83b 1 (3%) (10 yr) 28 (97%) (range, 24–79 yr) .02b,c P FS vs brain .54d .28d ↵a All P values were calculated using the Fisher exact test.
↵b To compare the sex and age compositions of each BT group with the general population, assuming even sex distribution and approximately 24% pediatric population.
c Significant.
↵d To compare the sex and age composition between the FS and brain BT groups.
- Table 8:
Imaging features of benign BT in immunocompetent patients compared with those of invasive fungal rhinosinusitis in immunocompromised patients
Incidental BT in Immunocompetent Patients Patients with IFRS Enhancement pattern Nonenhancing centrally with smooth, thin peripheral enhancement, likely normal mucosal enhancement Infiltrative nonenhancement extending into adjacent structures, without smooth, thin enhancing margin T2 characteristic Intermediate to hyperintense, but not hypointense Variable: hypointense, intermediate, or hyperintense Internal feature Faint septa or confluent dots Confluent nonenhancement Most common location for BT Posterior and midportions of inferior turbinate Middle turbinate NE confined to turbinate? Yes No Temporal feature Increased enhancement with time Persistent nonenhancement





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.