
Article Figures & Data
Figures
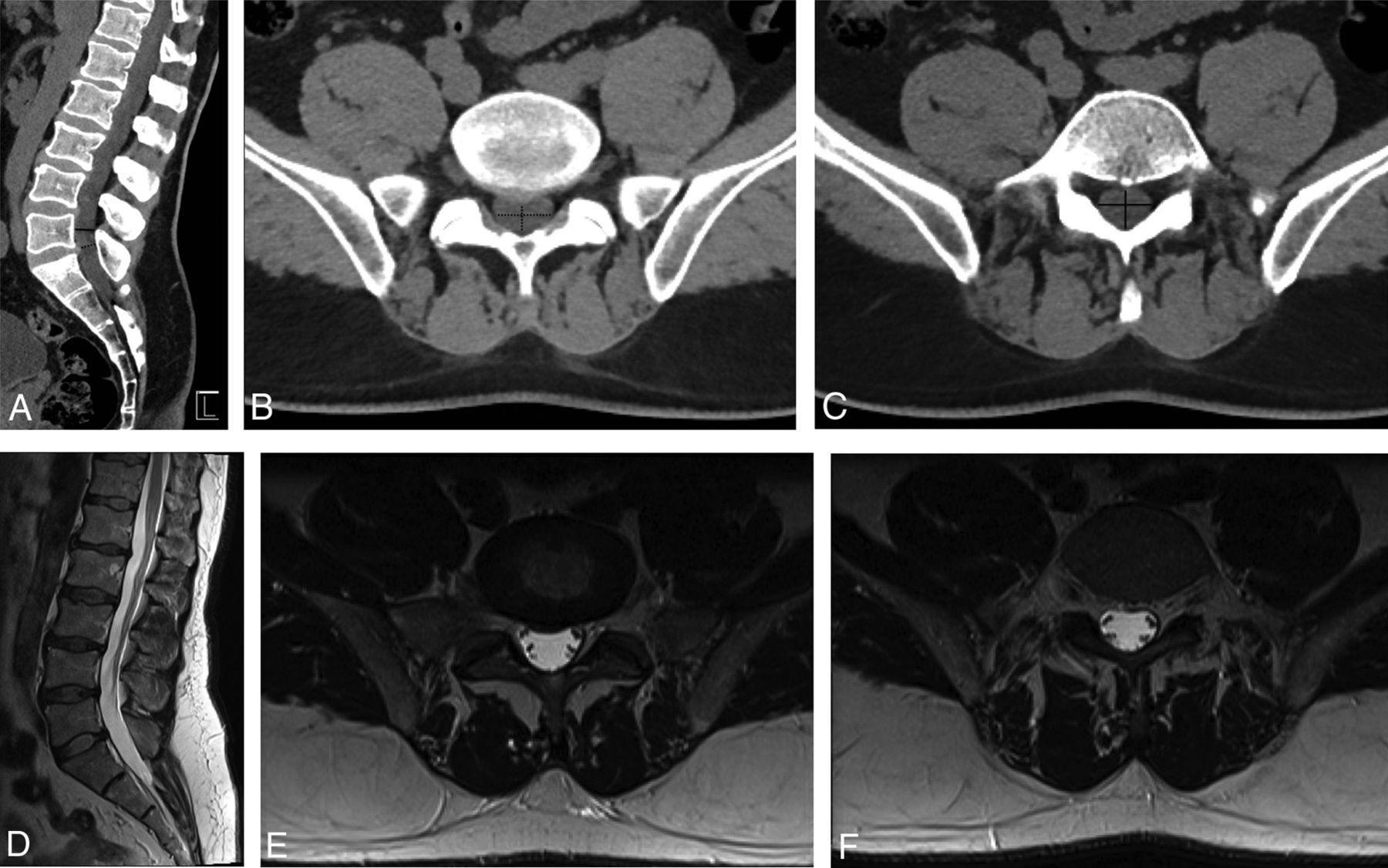
- Fig 1.
A 50-year-old man with acute-onset bilateral lower extremity numbness and severe low back pain. Application of the CT-PTSE imaging marker is demonstrated. Spinal stenosis from a disc protrusion at the L5/S1 level is assessed by delineating the estimated area of the thecal sac at this level (dashed black line, A and B). A normal reference level is identified just cranial to the stenosis (solid black line, A and C). The readers determined that CT-PTSE for this stenosis and others throughout the lumbar spine was <50%. MR imaging of the lumbar spine performed on the same day (D–F), with axial images through the L5–S1 stenosis (E) and the reference level (F), demonstrates concordant results with <50% thecal sac effacement and no evidence of cauda equina impingement.
- Fig 2.
A 61-year-old man with acute bilateral increased lower extremity paresthesias. CT (A and B) demonstrates degenerative spinal stenoses, most severe at L3/4 and L4/5 (solid arrow). Readers determined that CT-PTSE was ≥50%. MR imaging (C and D) confirms PTSE of ≥50% and demonstrates early impingement of the cauda equina.
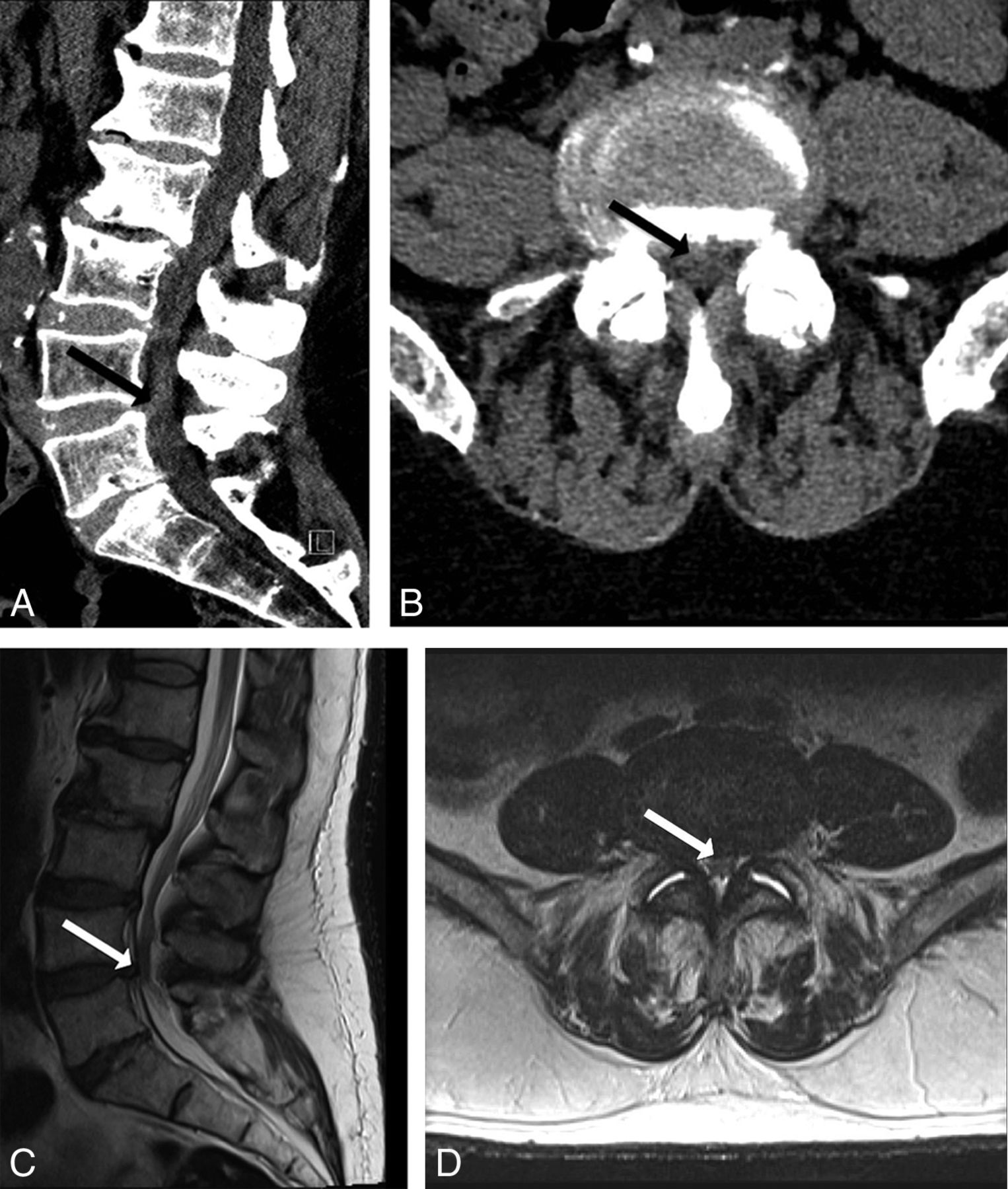
- Fig 3.
A 59-year-old man with metastatic renal cell carcinoma with worsening left lower extremity pain and difficulty ambulating. CT (A and B) demonstrates sclerotic osseous metastasis at L3, with a hyperdense soft-tissue component bowing and extending through the posterior vertebral body wall (solid arrow). Readers determined that CT-PTSE was ≥50%. MR imaging (C and D) confirms PTSE of ≥50 and demonstrates impingement of the cauda equina by tumor.
- Fig 4.
A 55-year-old man with severe low back pain following a fall from a roof. CT (A and B) demonstrates an L3 burst fracture with osseous retropulsion into the spinal canal (solid arrow). Readers determined that CT-PTSE was ≥50%. MR imaging (C and D) confirms PTSE of ≥50% and demonstrates impingement of the cauda equina.
- Fig 5.
A 42-year-old woman with lumbar back pain following trauma. CT (A and B) demonstrates a burst fracture of L1 with retropulsion of bone into the spinal canal (solid arrow). Streak artifacts from bone and the patient's upper extremities obscure the margins of the thecal sac, and readers determined that CT-PTSE may be ≥50%. This case proved to represent a false-positive because MR imaging (C and D) demonstrates a PTSE of <50% and no evidence of cauda equina impingement.





Tables
Demographic and clinical characteristics of the study populationa
Characteristics Patients (No.) 151 Female (No.) 46 (30.5%) Age (mean) (yr) 54.5 ± 19.5 MR-PTSE ≥50% (No.) 40 (26.5%) MR-PTSE <50% (No.) 111 (73.5%) CEI (No.) 19 (12.6%) MR-PTSE ≥50%, degenerative changes (No.) 23 (15.2%) MR-PTSE ≥50%, traumatic osseous retropulsion (No.) 12 (8%) MR-PTSE ≥50%, neoplastic (No.) 3 (1.9%) MR-PTSE ≥50%, hematoma (No.) 1 (0.7%) MR-PTSE ≥50%, infection (No.) 1 (0.7%) ↵a Results are expressed as absolute numbers (%) and mean.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}