
Abstract
BACKGROUND AND PURPOSE: Hereditary hemorrhagic telangiectasia is associated with a wide range of neurovascular abnormalities. The aim of this study was to characterize the spectrum of cerebrovascular lesions, including brain arteriovenous malformations, in patients with hereditary hemorrhagic telangiectasia and to study associations between brain arteriovenous malformations and demographic variables, genetic mutations, and the presence of AVMs in other organs.
MATERIALS AND METHODS: Consecutive patients with definite hereditary hemorrhagic telangiectasia who underwent brain MR imaging/MRA, CTA, or DSA at our institution from 2001 to 2015 were included. All studies were re-evaluated by 2 senior neuroradiologists for the presence, characteristics, location, and number of brain arteriovenous malformations, intracranial aneurysms, and nonshunting lesions. Brain arteriovenous malformations were categorized as high-flow pial fistulas, nidus-type brain AVMs, and capillary vascular malformations and were assigned a Spetzler-Martin score. We examined the association between baseline clinical and genetic mutational status and the presence/multiplicity of brain arteriovenous malformations.
RESULTS: Three hundred seventy-six patients with definite hereditary hemorrhagic telangiectasia were included. One hundred ten brain arteriovenous malformations were noted in 48 patients (12.8%), with multiple brain arteriovenous malformations in 26 patients. These included 51 nidal brain arteriovenous malformations (46.4%), 58 capillary vascular malformations (52.7%), and 1 pial arteriovenous fistula (0.9%). Five patients (10.4%) with single nidal brain arteriovenous malformation presented with hemorrhage. Of brain arteriovenous malformations, 88.9% (88/99) had a Spetzler-Martin score of ≤2. Patients with brain arteriovenous malformations were more likely to be female (75.0% versus 57.6%, P = .01) and have a family history of hereditary hemorrhagic telangiectasia (95.8% versus 84.8%, P = .04). The prevalence of brain arteriovenous malformation was 19.7% in endoglin (ENG) mutations and 12.5% in activin receptor-like kinase (1ACVRL1) mutations.
CONCLUSIONS: Our study of 376 patients with hereditary hemorrhagic telangiectasia demonstrated a high prevalence of brain arteriovenous malformations. Nidal brain arteriovenous malformations and capillary vascular malformations occurred in roughly equal numbers.
ABBREVIATIONS:
- BAVM
- brain arteriovenous malformation
- DVA
- developmental venous anomaly
- HTT
- hereditary hemorrhagic telangiectasia
Hereditary hemorrhagic telangiectasia (HHT), also known as Rendu-Osler-Weber disease, is an autosomal dominant disorder affecting vascular beds in multiple organ systems. Pathognomonic vascular lesions in HHT include arteriovenous malformations and telangiectasias of the skin, mucous membranes, and visceral organs, including the lung, liver, gastrointestinal tract, brain, and spinal cord.1 HHT is diagnosed clinically by using the Curacao criteria,2 which include spontaneous and recurrent epistaxis, mucocutaneous telangiectasias (lips, oral cavity, face and fingers), visceral AVMs (brain, liver, gastrointestinal, lung, and so forth), and a diagnosis of HHT in a first-degree relative by using the same criteria. Patients who meet ≥3 of the 4 criteria are labeled as having “definite HHT,” while those with 2 of the 4 criteria are labeled as having “possible” or “suspected” HHT.3
Patients with HHT can present with myriad CNS complications, including vascular malformations of the brain and spinal cord. There has been much interest in studying the prevalence, characteristics, and natural history of brain AVMs (BAVMs) and other vascular anomalies in patients with HHT due to their associated morbidity. While several studies have examined the prevalence of vascular malformations and anomalies in patients with HHT, few have sought to provide a detailed characterization of the anatomic, angiographic, and clinical correlates of these lesions. The aims of the present study were the following: 1) to determine the prevalence of cerebral vascular lesions, including BAVMs and nonshunting vascular lesions such as developmental venous anomalies (DVAs), intracranial aneurysms, and cavernous malformations in the HHT population; 2) to subclassify BAVMs by using previously described criteria4; and 3) to determine whether there are any associations between the presence of BAVMs and demographic variables, vascular lesions in other organs, and genetic mutation status.
Materials and Methods
Patient Population
The study was approved by our institutional review board. We included all patients with definite HHT with available neuroimaging studies (cerebral angiography, CT angiography, MR imaging, and/or MR angiography) seen at our institution from January 2001 to May 2015. Patients were initially identified by querying our electronic medical record for the terms HHT, hereditary hemorrhagic telangiectasia, Osler-Weber-Rendu, or Rendu-Osler-Weber. We also searched for any patients with an International Classification of Diseases-9 code for HHT (448.0) in their electronic medical record. Then, all the shortlisted patient records were individually reviewed to determine which Curacao criteria were met. Only those meeting ≥3 Curacao criteria and with available neuroimaging studies were included in the final cohort. Patients meeting ≤2 Curacao criteria (ie, patients with suspected HHT) were excluded.
Demographic and Clinical Data
The following baseline demographic data were collected for each patient: age, sex, HHT mutation status (if available), and family history. HHT mutations were classified as ENG mutations (as seen in HHT1), ACVRL1 mutations (as seen in HHT2) and SMAD4 mutations. Information on the presence of HHT-associated complications, including epistaxis; liver, gastrointestinal, or pulmonary AVMs; and mucocutaneous telangiectasia was collected as well.
Imaging Evaluation
All neuroimaging was evaluated by 2 senior neuroradiologists with 15 and 20 years of experience and a senior radiology resident. Images were re-evaluated for the presence of BAVMs, DVA, intracranial aneurysms, cavernous malformations, and capillary telangiectasias. In case of disagreement, a consensus was reached with the help of a third neuroradiologist. BAVMs were classified according to the criteria put forth by Krings et al4 as high-flow “single-hole” pial fistulas, nidus-type BAVMs, and capillary vascular malformations. A pial AVF was defined by the presence of shunting in association with an abnormally dilated pial artery and the absence of an intervening nidus. Nidus-type BAVMs were defined by the presence of an abnormal network of dilated vessels (ie, a nidus) present between the feeding artery and draining vein. Capillary vascular malformations were defined by the presence of a blush of abnormal vessels seen either during the capillary phase of cerebral angiography with a single draining vein or by an area of fluffy, stainlike enhancement on contrast-enhanced CT or MR imaging, with a nondilated feeding artery and draining vein. Capillary vascular malformations did not show flow voids on MR imaging. The Spetzler-Martin score was calculated for each BAVM, and the presence of hemorrhage at the time of diagnosis was also recorded. In assessing the Spetzler-Martin score and eloquent location was defined as the sensorimotor, language or visual cortex, hypothalamus, thalamus, brainstem, cerebellar nuclei or regions directly adjacent to these structures. The locations of DVAs, aneurysms, cavernous malformations, and capillary telangiectasias were recorded as well.
Statistical Analysis
Continuous variables were compared by using the Student t test, and categorical variables, with the χ2 test. All analyses were performed by using JMP 12.0 (SAS Institute, Cary, North Carolina). We determined prevalence of BAVMs, DVAs, intracranial aneurysms, and cavernomas in the HHT population. We also tested for differences in age, sex, and HHT gene mutation, and the presence of other vascular abnormalities between patients with HHT and BAVMs and those without. Additional tests were performed to determine variables associated with BAVM multiplicity.
Results
Patient Population
Three hundred seventy-six patients with definite HHT were included in this study. The mean patient age was 53.0 ± 43.4 years, and most were women (n = 225, 59.8%). Manifestations of HHT included epistaxis in 334 (88.8%) patients, mucocutaneous telangiectasias in 327 (87.0%), visceral AVMs in 321 (85.4%), and a positive family history of HHT in 324 (86.2%) patients. One hundred thirty-three patients had genetic testing, of whom 123 (27.1%) had positive findings on a genetic test. Of the 123 with positive findings on a genetic test, 61 (49.6%) had endoglin (ENG) mutations, 48 (39.0%) had activin receptor-like kinase 1 (ACVRL1) mutations, and 14 (11.4%) had SMAD family member 4 (SMAD4) mutations. Of the 10 with negative findings on a genetic test, all 10 met at least 3 Curacao criteria, suggesting a diagnosis of definite HHT. Of the 311 patients with chest CTs, 176 (56.6%) had pulmonary AVMs. Of the 344 patients with abdomen and pelvis CTs, 185 patients (53.8%) had evidence of hepatic vascular malformations. These data are summarized in Table 1.
Patient population and prevalence of vascular lesions
Prevalence and Characteristics of Brain AVMs
One hundred ten BAVMs were found in 48 patients (12.8%), including 26 patients with multiple BAVMs. These included 51 nidal BAVMs (46.4%), 58 capillary vascular malformations (52.7%), and 1 pial arteriovenous fistula (0.9%). Hemorrhage was the presenting manifestation in 5 patients (10.4%), each with a single nidal BAVM; all lesions were successfully treated on the first presentation. The 2 most common locations of BAVMs were the frontal lobes (n = 48, 43.6%) and the cerebellum (n = 17, 15.4%). Size measurements were available for 100 lesions, exact cortical location was available for 100 lesions, and venous drainage data were available for 99 lesions. Complete Spetzler Martin scores were calculated for 99 BAVMs, of which most (n = 88, 88.9%) had scores of ≤2. Of the characterizable BAVMs, 97 (97.0%) had a nidus size of <3 cm, 51 (51.0%) were in an eloquent location, and 16 (16.1%) had deep venous drainage. These data are summarized in Table 2.
Characteristics of AVMs
Of the 51 nidal BAVMs, 40 (78.4%) were supratentorial and 11 (21.6%) were infratentorial. A nidus size of >3 cm was seen in 2 nidal BAVMs (4.8%), and 10 (25.0%) had deep venous drainage. Twenty-six nidal BAVMs (63.4%) were in an eloquent location; 80.0% (32 nidal BAVMs) had a Spetzler-Martin score of ≤2. Representative examples of nidal-type BAVMs are shown in Fig 1.

Characteristics of nidal AVMs. A and B, Superficially located nidal AVMs in the frontal lobes of 2 patients with definite HHT. The lesions lack features such as venous stenoses or intranidal aneurysms and drain into superficial veins. C, A cerebellar nidal AVM in a patient with definite HHT, which drains into a superficial cerebellar vein and into the transverse sinus. D, Diffuse AVM involving a large portion of the right cerebral hemisphere. The AVM has multiple large venous ectasias and drains into the deep and superficial venous systems.
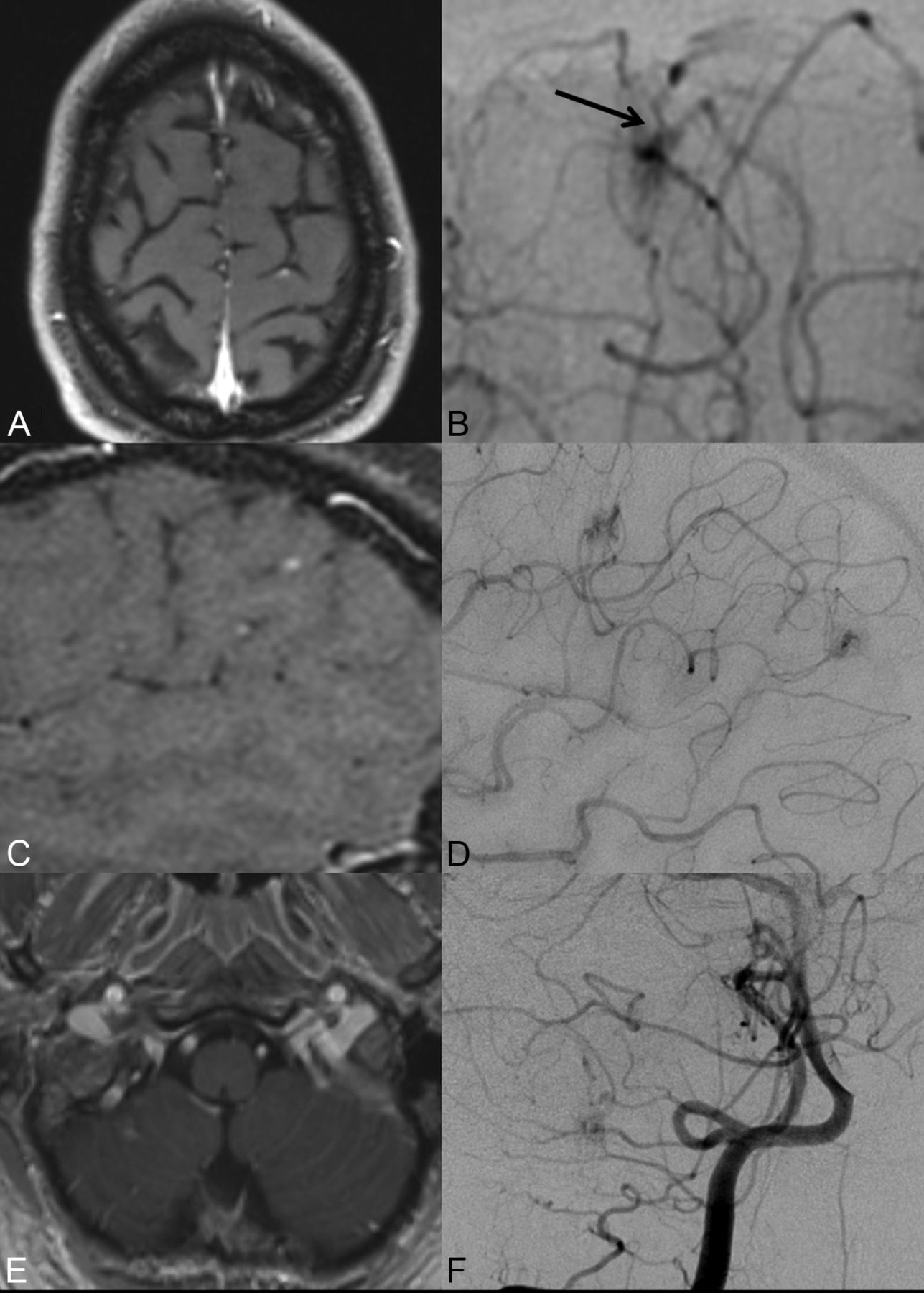
Of the 58 capillary vascular malformations, 50 (86.2%) were supratentorial and 8 (13.8%) were infratentorial. All measured <1 cm in maximal diameter. Twenty-four (41.4%) were in an eloquent location, 6 (10.3%) had a deep venous drainage, and 56 (96.5%) had a Spetzler-Martin score of ≤2. Representative examples of capillary vascular malformations are provided in Fig 2. These data are summarized in Table 3.

A, T1 contrast-enhanced MR image demonstrates a punctate focus of enhancement. The corresponding angiographic view (B) shows a capillary vascular malformation with a small draining vein. C, T1 contrast-enhanced MR image shows a punctate focus of enhancement in the parietal lobe in a patient with definite HHT. D, Cerebral angiography in this patient shows 2 capillary vascular malformations in the parietal lobe, one of which was occult on MR imaging. E, T1 contrast-enhanced MR imaging demonstrates a small focus of enhancement in the right cerebellar hemisphere. F, A corresponding cerebral angiogram demonstrates a capillary vascular malformation with a single feeding artery and draining vein.
Characteristics of AVMs by AVM Type
Prevalence and Characteristics of Nonshunting Cerebral Vascular Lesions
Fifty-two DVAs were noted in 45 patients (12.0%), with 4 patients having >1 DVA. The most common locations were in the frontal lobes (19, 36.5%) and the cerebellum (17, 32.7%). All DVAs were asymptomatic.
Twenty-eight cavernomas were noted 13 patients (3.5%), with 5 patients having multiple cavernomas. The most common locations for cavernomas were the frontal lobes (n = 12, 42.9%) and occipital lobes (n = 7, 25.0%). Only 1 cavernoma was symptomatic and was surgically removed.
Thirteen capillary telangiectasias were noted in 9 patients (2.4%). Two patients had >1 capillary telangiectasia. The most common location for capillary telangiectasia was the brain stem (n = 6, 46.2%). These data are summarized in Table 4. Representative examples of nonshunting vascular lesions are provided in Fig 3.
Nonshunting vascular lesions

A, T2-weighted MR image demonstrates a typical cavernoma. B, T1 contrast-enhanced MR image demonstrates a large developmental venous anomaly in the cerebellar vermis, with a typical caput medusa appearance. C and D, T1 contrast-enhanced MRIs demonstrate the typical appearance of capillary telangiectasias.
Eight patients (2.1%) had 16 cerebral aneurysms. Three patients (37.5%) had multiple aneurysms. Five aneurysms (31.3) were associated with AVMs, and 1 aneurysm (6.3%) bled. The mean aneurysm size was 3.8 ± 2.0 mm. Aneurysms were most commonly located in the territory of the internal carotid artery (50.0%). These data are summarized in Table 5. Representative examples of aneurysms are provided in Fig 4.
Characteristics of saccular aneurysms

A, 3D reconstruction of an MRA demonstrates bilateral carotid siphon aneurysms and a dysplastic right MCA. B, This patient has a 1.5-cm nidal AVM in the left MCA territory. C, Noncontrast head CT shows diffuse subarachnoid hemorrhage in a patient with HHT with an 8-mm ruptured anterior communicating artery aneurysm (D).
Clinical and Genetic Variables Associated with BAVMs
Patients with BAVMs were more likely to be women (75.0% versus 57.6%, P = .01) and have a positive family history for HHT (95.8% versus 84.8%, P = .04). Genetic mutational status was available for 18 patients with BAVMs and 105 without BAVMs. ENG mutations were present in 66.6% of the patients with BAVMs (12/18) and in 46.7% (49/105) of those without them. The overall prevalence of BAVMs in patients with ENG mutations was 19.7% versus 12.5% in patients with ACVRL1 mutations and 0% in those with SMAD4 mutations. There was no difference in the mean age of patients with and without BAVMs (P = .38) and no difference in the proportion of patients with pulmonary AVMs (P = .46) or gastrointestinal AVMs (P = .27). These data are summarized in Table 6.
Risk factors for AVMs and AVM multiplicity
Clinical Characteristics of Patients with Single-versus-Multiple BAVMs
As mentioned previously, multiple BAVMs were found in 26 patients, and 22 had a single BAVM. Among patients with multiple BAVMs, 7 had gene testing, of whom 6 (85.7%) had ENG mutations. Among patients with single BAVMs, 11 had gene testing, of whom 6 (54.5%) were positive for ENG mutations. Overall, multiple BAVMs were present in 9.8% (6/61) of patients with ENG mutations compared with 2.1% (1/48) of patients with ACVRL1 and 0% of those with SMAD4 mutations. No variables were associated with AVM multiplicity.
Discussion
Our study of 376 consecutive patients with a diagnosis of definite HHT found the prevalence of BAVMs to be 12.8%, with a relatively even split between capillary vascular malformations and nidus-type BAVMs. More than 80% of BAVMs were supratentorial. Only 3% had a nidus size of >3 cm, and < 20% had deep venous drainage. Approximately 10% of patients with BAVMs presented with rupture. Variables associated with the presence of a BAVM included female sex and a positive family history of HHT. Similar to prior studies, we demonstrated a higher prevalence of both single and multiple BAVMs among patients with ENG mutations. These findings are important because they provide further insight into the prevalence, risk factors, and characteristics of cerebral AVMs in the HHT population.
Large prospective screening studies have demonstrated BAVM prevalence rates between 10% and 20%, depending on the HHT population being screened.5⇓⇓⇓⇓–10 These are similar to rates in our study in which we found a 12.8% BAVM prevalence. In general, most studies have demonstrated a similar prevalence of BAVMs in male and female patients, unlike our study, which demonstrated a preponderance of women in the HHT group.7⇓–9,11⇓–13 In general, the prevalence of cerebral AVMs has been shown to be higher in patients with ENG mutations compared with those with ACVRL1 mutations.8,10 Lesion multiplicity is thought to be a hallmark of HHT. According to 1 recently published study, 44% of patients with HHT with cerebral vascular malformations had at least 2 different brain malformations.4 In our series, >50% of patients with BAVMs had multiple AVMs. On the basis of the high prevalence of cerebral AVMs in the HHT population, most experts agree that screening MR imaging is warranted for both adults and children.14
While several studies have examined the prevalence of AVMs in the HHT population, few studies have sought to characterize these lesions. In a study of 75 patients with 125 BAVMs, Krings et al4 found that nearly two-thirds of BAVMs were capillary vascular malformations. Similar to findings in our study, they found that these lesions were primarily supratentorial with a superficial location and were <1 cm. A report from the Bicêtre Hospital found that approximately 20% of AVMs were capillary vascular malformations, with a similar distribution in size and location compared with those in our study.15 Differences in the prevalence of capillary vascular malformations between studies are likely due to a combination of differences in imaging techniques (ie, they are more easily detected angiographically than on MR imaging) and indications for imaging, because these lesions are often detected incidentally and are not associated with hemorrhage, seizure, or headache.4
Capillary vascular malformations are distinct from capillary telangiectasia because they consist of a feeding artery, dilated capillary bed, and, generally, a single draining vein. Meanwhile, capillary telangiectasias consist of numerous thin-walled ectatic capillaries interspersed between normal brain parenchyma and lack an identifiable feeding artery, though they can sometimes have a draining vein. Capillary telangiectasias are typically angiographically occult and are located in the pons, while capillary vascular malformations are best appreciated angiographically and have a supratentorial location.
In our series, nidal-type AVMs represented the most common type of BAVM. More than 95% of these lesions had a small nidus, and approximately 50% were in an eloquent location. A vast majority were superficially located and had superficial venous drainage. These findings are similar to those in a number of studies that have demonstrated that >90% of nidal AVMs have a Spetzler-Martin score of ≤2 and are typically located in a superficial, supratentorial location with pial-based feeding arteries.4,15⇓–17 These lesions tend to measure 1–2 cm and tend to lack features such as arterial stenoses, associated aneurysms, multiple draining veins, venous ectasia, and venous reflux.4 Unlike capillary vascular malformations however, nidus-type BAVMs do not have a completely benign natural history because these lesions can rupture, as seen in our study.
Most interesting, we found a relatively high prevalence of DVAs (12.0%), capillary telangiectasias (2.4%), and cavernomas (3.5%). In the general population, the prevalence of DVAs is about 2%, while capillary telangiectasias and cavernomas are present in about 0.5% of patients. Most DVAs, capillary telangiectasias, and cavernomas are found incidentally. All 3 of these lesions typically have a benign natural history in both the HHT and general populations. While prior studies have suggested that patients with HHT have higher rates of telangiectasias and DVAs, an association between HHT and cavernomas has not been demonstrated, to our knowledge. One possible explanation for the higher rates of these lesions in patients with HHT compared with the general population is that capillary telangiectasias, cavernomas, and DVAs have all been linked to elevations in vascular endothelial growth factor (VEGF) expression.18⇓–20 Some authors have reported an association between cerebral AVMs and vascular anomalies such as DVAs and capillary telangiectasias; however, this is thought to be rare. The high prevalence of DVAs and BAVMs in the HHT population could potentially be problematic in the setting of a BAVM draining into a DVA. However, such a finding is rare and has been reported in only a few case reports.21
The rate of cerebral aneurysms in our study was 2%, which is similar to the rate reported in the general population.22 Approximately one-third of aneurysms in our series were associated with BAVMs. One recently published study demonstrated a higher rate of visceral arterial aneurysms in the HHT population, attributing this to alterations in the transforming growth factor–β signaling pathway.23 While some studies indicate that alterations in the transforming growth factor–β signaling pathway play a role in the pathogenesis of intracranial aneurysms, no study to date has demonstrated a higher prevalence of intracranial aneurysms in the HHT population when compared to the general population.24
Limitations
Our study has limitations. First, because this was not a prospective screening study, there are substantial limitations in the ascertainment of cases. Patients who present with symptoms such as headache, seizure, or focal neurologic symptoms may be more likely to have a neurovascular lesion than those who present for asymptomatic screening. While it is possible that we overestimated the prevalence of neurovascular lesions in the HHT population due to this limitation, the prevalence of cerebral AVMs in our study was similar to that reported in the literature. Another limitation is that we did not have information regarding genotypes for most patients. While both patients with HHT1 and HHT2 present with higher rates of BAVMs than the general population, most studies have demonstrated a higher rate of BAVMs in the HHT1 population. Another limitation is that not all patients with BAVMs underwent 4-vessel cerebral angiography. Cerebral angiography is significantly more sensitive than contrast-enhanced MR imaging and MRA in detecting smaller arteriovenous malformations and is a better way to characterize these lesions. However, lesions that are occult on MR imaging are probably more likely to be capillary vascular malformations, which are known to have a benign natural history.
Conclusions
Our study of 376 patients with suspected or definite HHT demonstrated a high prevalence of cerebral AVMs (BAVMs) and nonshunting vascular lesions, including DVAs, capillary telangiectasias, and cavernomas. Hemorrhage was the presenting feature in 10% of patients with BAVMs. More than 50% of patients with BAVMs had multiple cerebral AVMs, with the most common lesions being capillary vascular malformation–type BAVMs, followed by nidal-type BAVMs. Future research is needed to determine the predictors of BAVM formation and multiplicity in the HHT population and to better determine the natural history and optimum treatment options for these lesions.
Footnotes
Disclosures: Giuseppe Lanzino—UNRELATED: Consultancy: Covidien/ev3.* *Money paid to the institution.
References
- Received October 30, 2015.
- Accepted after revision January 28, 2016.
- © 2016 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Prevalence and Characteristics of Intracranial Aneurysms in Hereditary Hemorrhagic Telangiectasia
- Prevalence of Intracranial Aneurysms in Hereditary Hemorrhagic Telangiectasia: Report from a Single Reference Center
- British Thoracic Society Clinical Statement on Pulmonary Arteriovenous Malformations
- Regarding "Neurovascular Manifestations of Hereditary Hemorrhagic Telangiectasia: A Consecutive Series of 376 Patients during 15 Years"
- Reply: