
Article Figures & Data
Figures
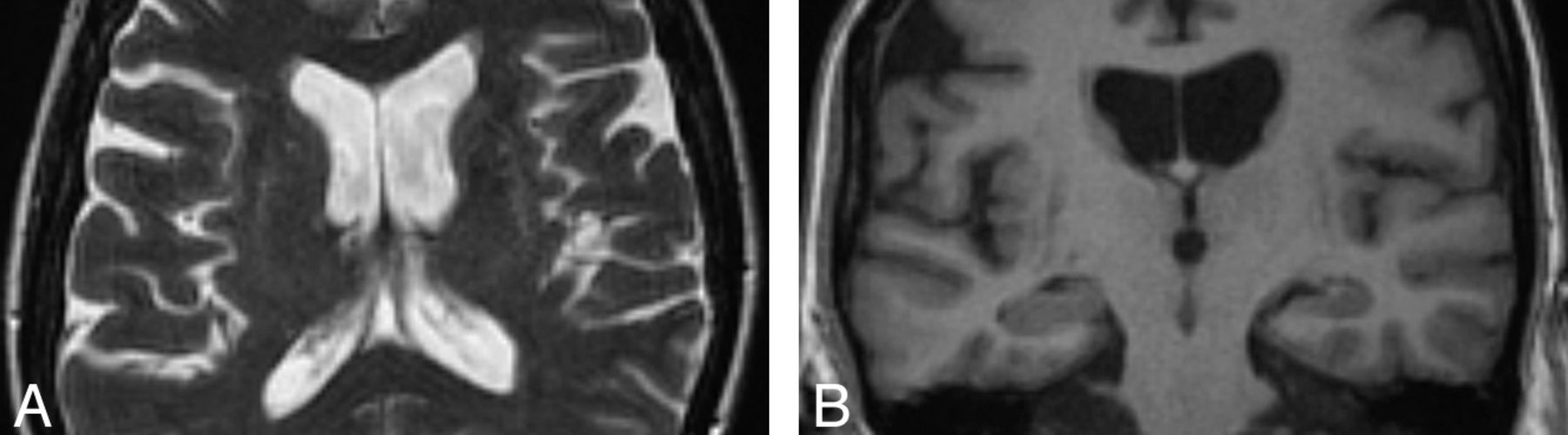
- Fig 1.
Axial T2-weighted MR imaging sequence at 1.5T in a patient with MSA-P (A) demonstrating hyperintense putaminal rims. The sign is 96% specific in differentiating patients with MSA from those with idiopathic Parkinson disease; however, it is only 56% sensitive according to 1 study.6 The corresponding coronal T1-weighted MR imaging sequence (B) shows that the putaminal rims are hypointense. The putaminal rim sign is nonspecific in the wider population—for example, it can be seen in Wilson disease or some spinocerebellar ataxia subtypes. It is also a normal finding at 3T.
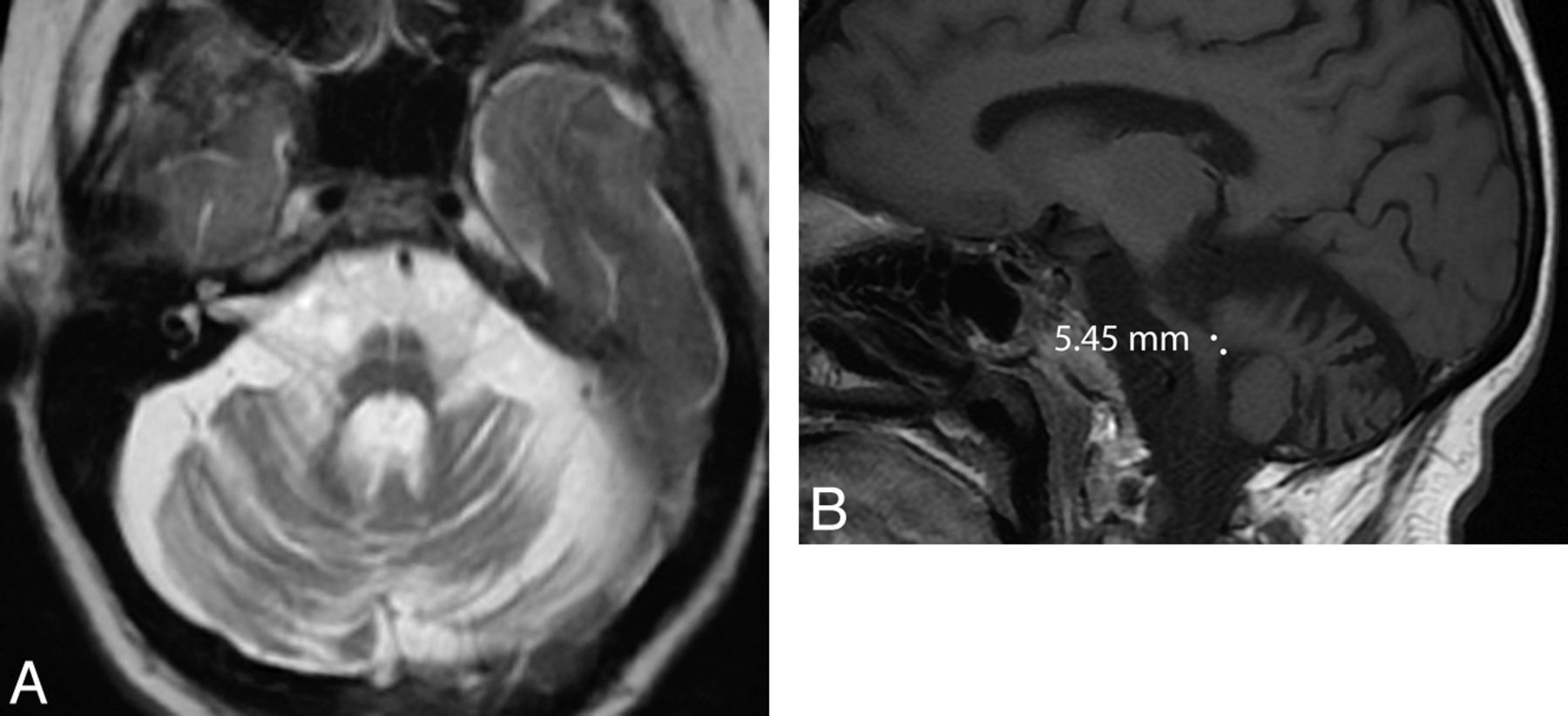
- Fig 2.
Axial T2-weighted MR imaging sequence in a patient with MSA with predominant cerebellar ataxia (A) demonstrating the “hot-cross bun” sign, which results from selective loss of myelinated pontine transverse fibers and raphe neurons. One study showed that the sign is 100% specific in differentiating patients with MSA from those with idiopathic Parkinson disease; however, it is only 50% sensitive.6 Marked pontine and cerebellar atrophy is also demonstrated. This olivopontocerebellar volume loss is shown on the sagittal T1-weighted sequences (B), where a middle cerebellar peduncle width <8 mm is demonstrated. All these signs are nonspecific in the wider population—for example, they can be seen in some spinocerebellar ataxia subtypes.
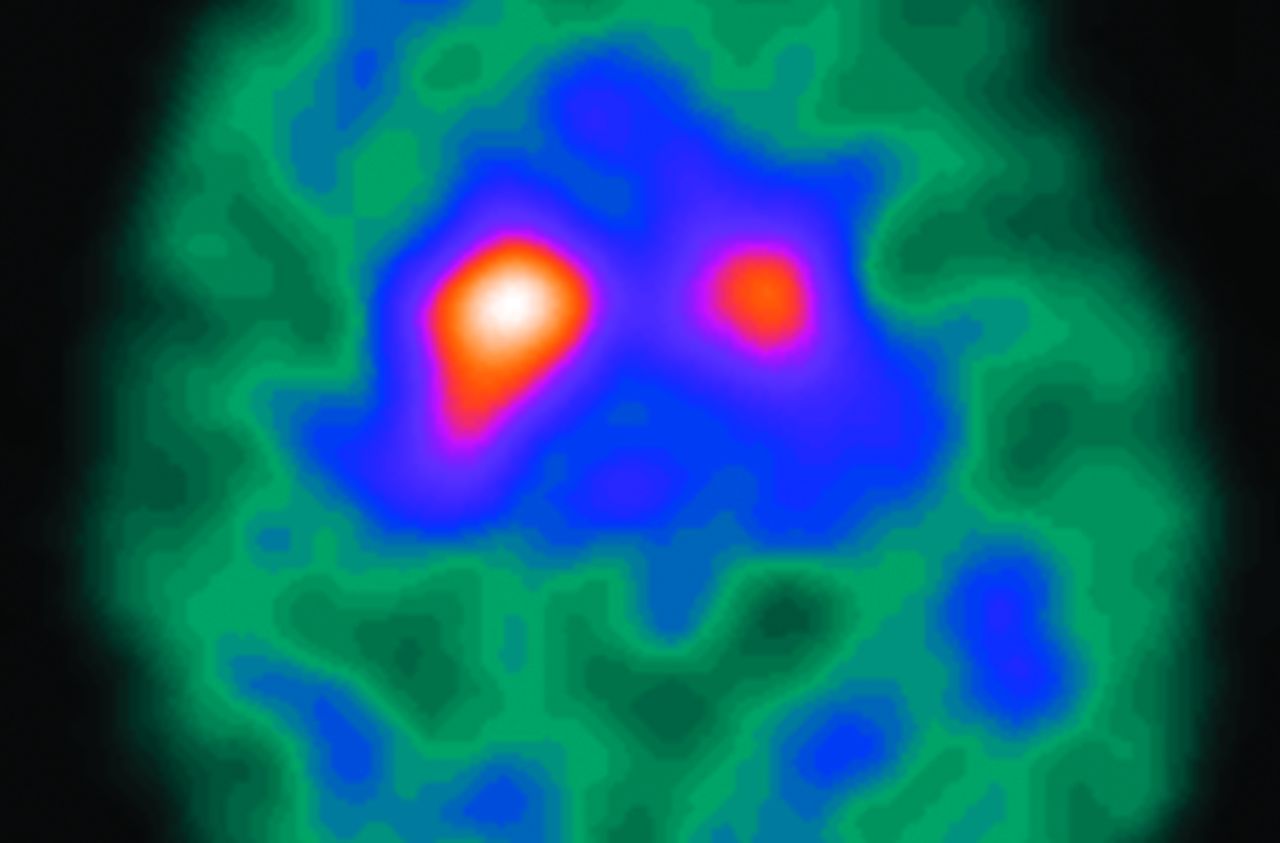
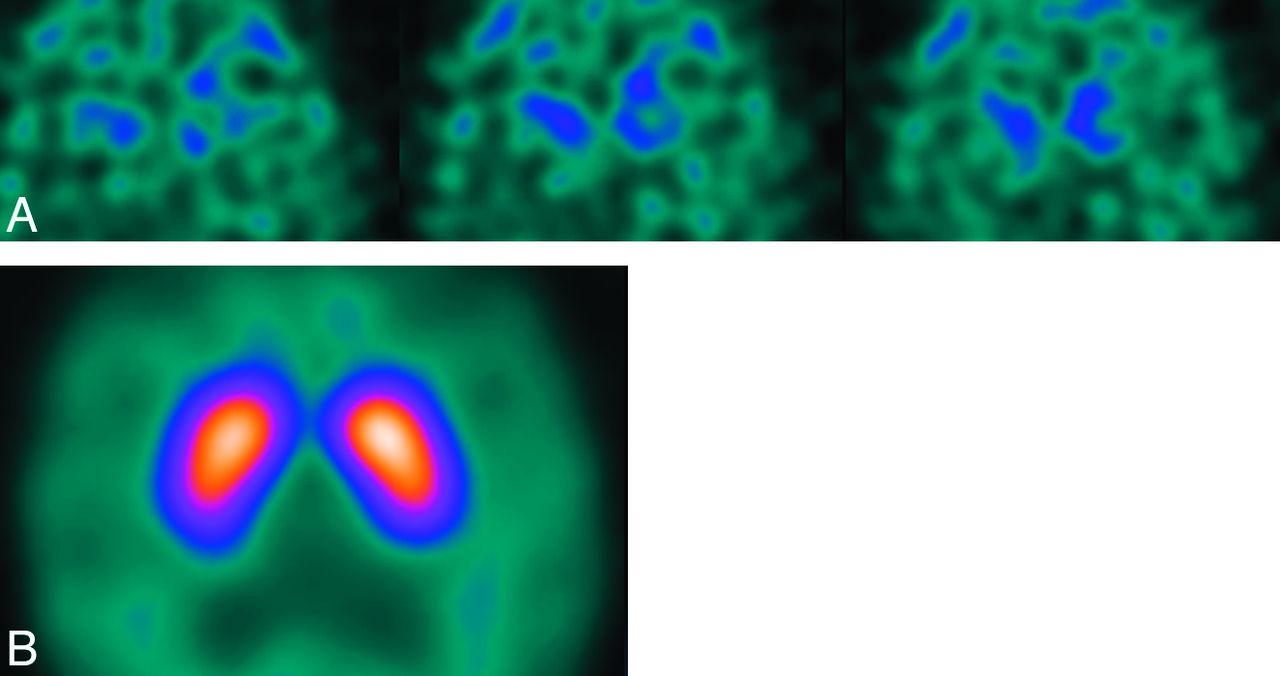
- Fig 3.
Axial 123I-FP-CIT DaT-SPECT image in a patient with MSA. Note that imaging appearances are similar to those in idiopathic Parkinson disease, with asymmetric reduction in putaminal uptake. It is, therefore, difficult to differentiate MSA and idiopathic Parkinson disease on the basis of DaT-SPECT imaging alone.
- Fig 4.
Axial T2-weighted MR imaging sequence in a patient with PSP (A) demonstrating increased midbrain signal intensity (which is only 60% sensitive and 70% specific compared with MSA) and an atrophic midbrain with an anteroposterior diameter of <17 mm (which is 23% sensitive and 96% specific compared with MSA).5 The signs are nonspecific in the wider population—for example, midbrain signal intensity can be seen in Wilson disease and a severely atrophic midbrain can be seen in CBD. The concave posterolateral borders of the atrophic midbrain give it a “morning glory” flower appearance. The corresponding sagittal T1-weighted sequence (B) shows tectal atrophy with a “hummingbird” appearance.
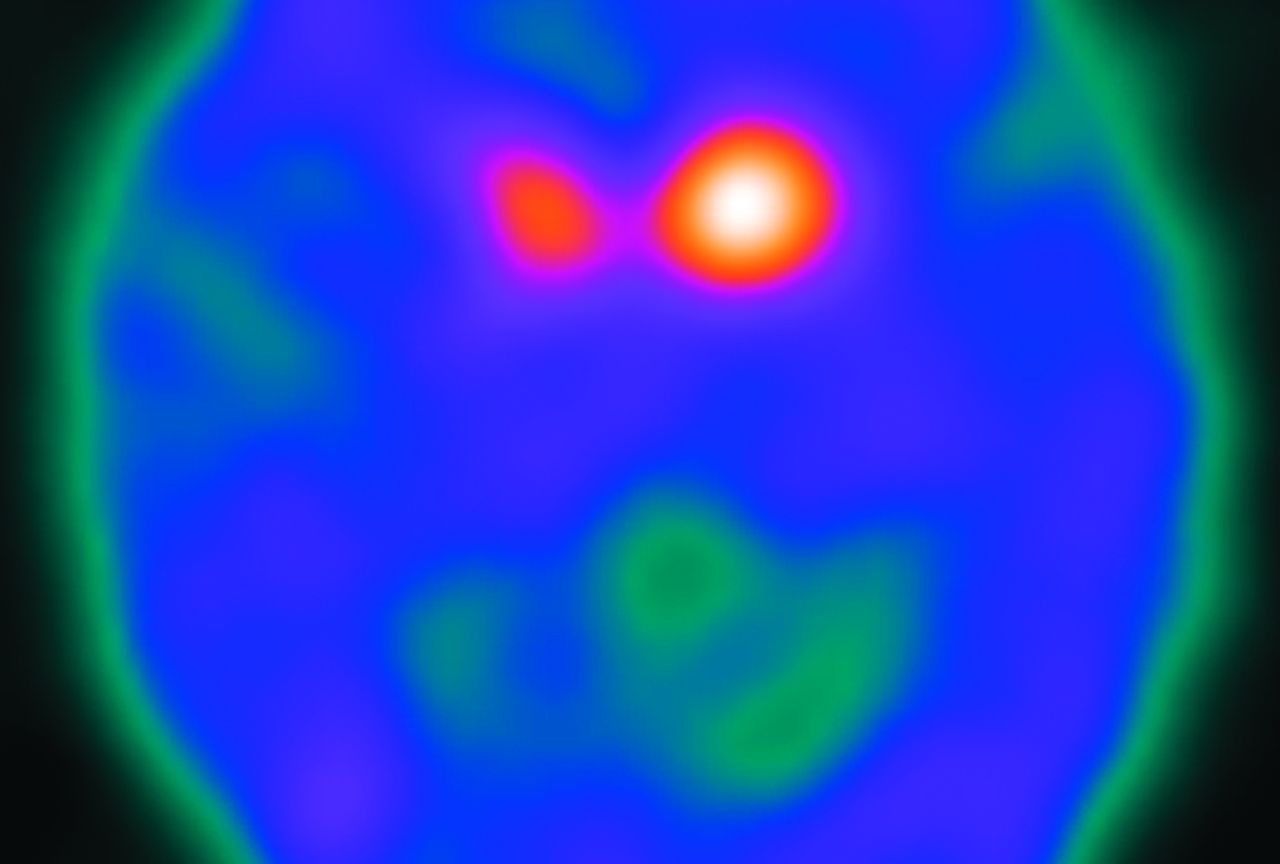
- Fig 5.
Axial 123I-FP-CIT DaT-SPECT image in a patient with PSP, depicting a bilateral reduction in putaminal uptake. Note that the imaging features are similar to those of idiopathic Parkinson disease and MSA.
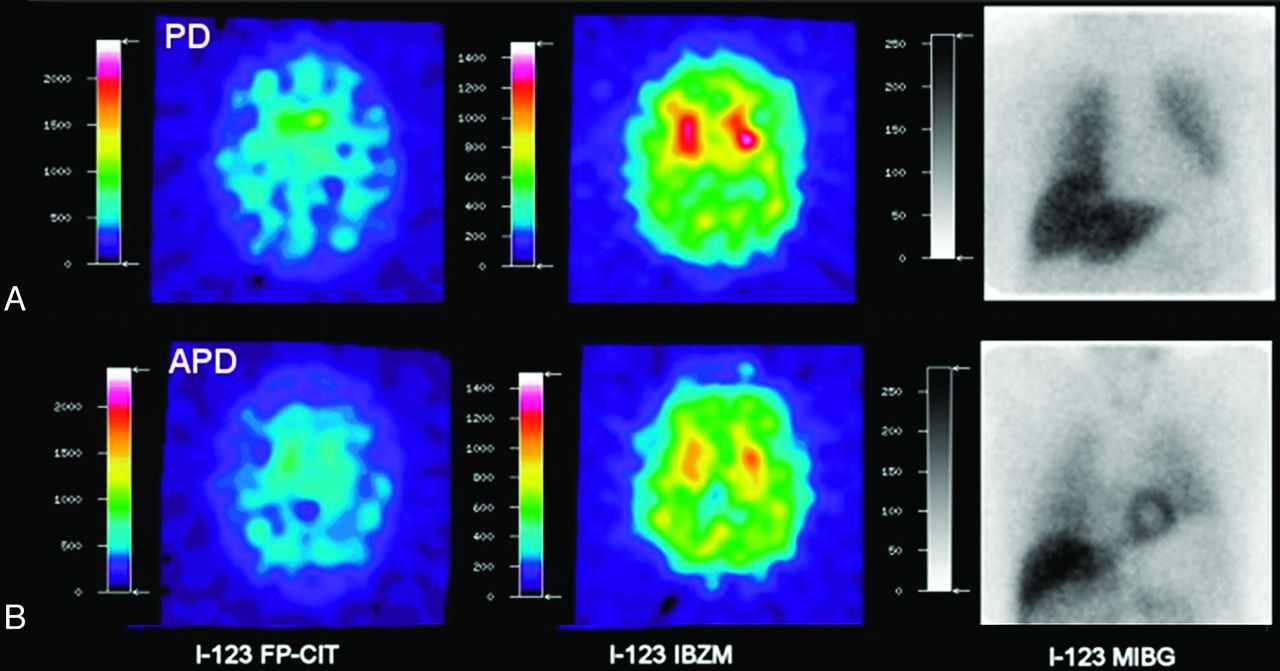
- Fig 6.
Axial 123I-FP-CIT DaT-SPECT, 123I-IBZM, and meta-123I-iodobenzylguanidine SPECT studies in idiopathic Parkinson disease (A) and atypical Parkinson disease (MSA or PSP) (B). Uptake patterns with all 3 radiopharmaceuticals are typical for idiopathic Parkinson disease with asymmetric striatal reduction using 123I-FP-CIT, normal dopamine D2 receptor binding with 123I-IBZM, and reduction in myocardial uptake due to adrenergic denervation with meta-123I-iodobenzylguanidine (A). B, Images demonstrate findings of MSA or PSP: reduced striatal uptake with 123I-FP-CIT and 123I-IBZM but normal myocardial uptake with meta-123I-iodobenzylguanidine. Image courtesy of Dr M. Südmeyer. This was originally published in: Südmeyer M, Antke C, Zizek T, et al. Diagnostic accuracy of combined FP-CIT, IBZM, and MIBG scintigraphy in the differential diagnosis of degenerative parkinsonism: a multidimensional statistical approach. J Nucl Med 2011;52:733–40. © by the Society of Nuclear Medicine and Molecular Imaging, Inc.
- Fig 7.
Axial T2-weighted MR imaging sequence in a patient with CBD (A) demonstrating asymmetric frontoparietal atrophy. The corresponding coronal FLAIR sequence (B) shows the asymmetric superior parietal lobules.
- Fig 8.
Axial 123I-FP-CIT DaT SPECT image in a patient with corticobasal degeneration. There is uniform striatal reduction in tracer activity with marked hemispheric asymmetry on the left. However, in many cases, imaging appearances can be indistinguishable from those in idiopathic Parkinson disease, MSA, or PSP. Image courtesy of Dr Roberto Ceravolo, Department of Neurosciences, University of Pisa, Italy.45
- Fig 9.
Axial 123I-FP-CIT DaT-SPECT images in a patient with dementia with Lewy bodies (A) and a patient with Alzheimer disease (B). Note that the DaT-SPECT study helped to distinguish the 2 causes of dementia with the patient with dementia with Lewy bodies exhibiting a Catafau and Tolosa2 type 3 pattern of abnormal striatal uptake; in contrast, the patient with Alzheimer disease demonstrates normal striatal uptake. Images from both patients have low gain as demonstrated by low background activity.
- Fig 10.
Axial 123I-FP-CIT DaT-SPECT (A) and axial MR imaging FLAIR sequence (B) of the brain in the same patient with vascular parkinsonism. Note that the DAT-SPECT study has normal findings with symmetric, intense uptake in the caudate nuclei and putamina. This effectively excludes a nigrostriatal degenerative cause of parkinsonism. Consistent with ischemic disease, the MR imaging demonstrates diffuse T2-weighted hyperintensities in the striatum and in the periventricular and subcortical white matter.
- Fig 11.
Axial 123I-FP-CIT DaT-SPECT image from a patient with schizophrenia on neuroleptic medication. The patient presented with extrapyramidal signs. If the patient's clinical signs were purely due to the side effects of neuroleptic medication, then the DaT-SPECT study findings would be normal. However, in this case, there is absent putaminal uptake bilaterally and asymmetric caudate nuclei uptake (Catafau and Tolosa2 type 2), indicative of coexistent idiopathic Parkinson disease, MSA, or PSP.
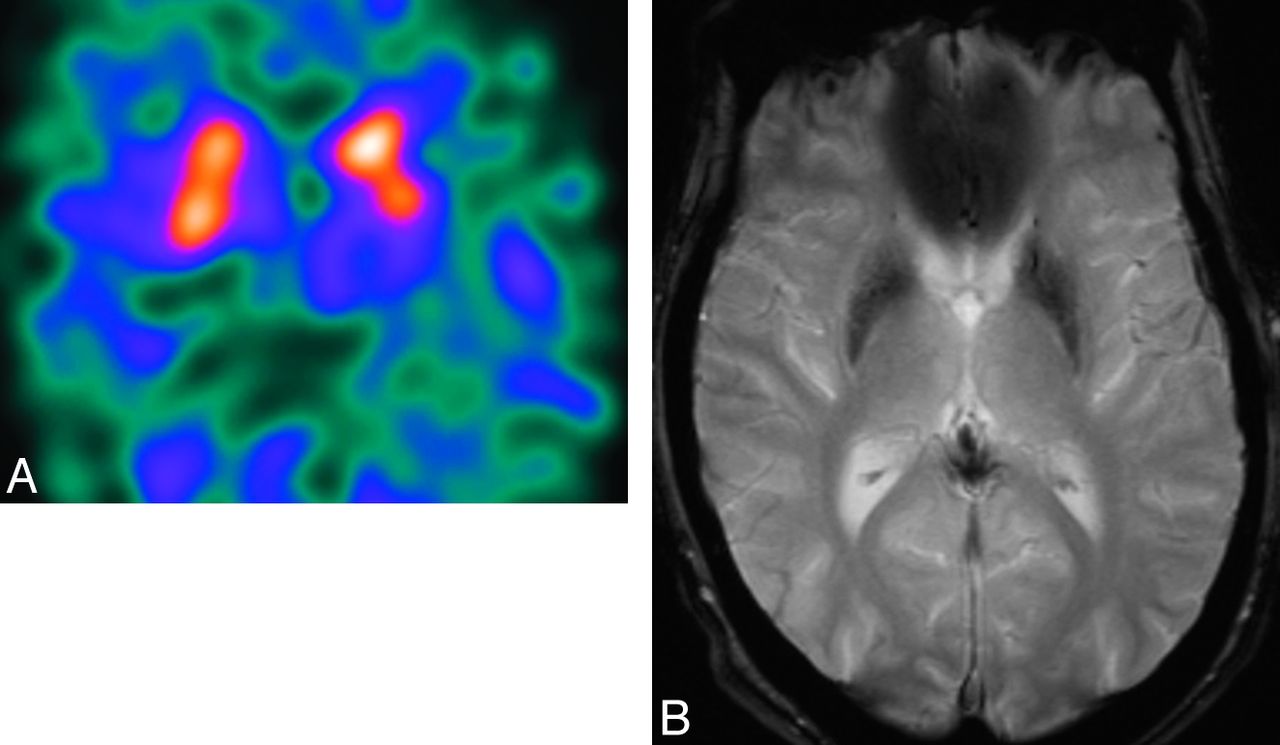
- Fig 12.
Axial 123I-FP-CIT DaT-SPECT image (A) and axial T2*-weighted MR imaging sequence (B) in the same patient with neuroacanthocytosis. The patient presented with parkinsonian features. Note the asymmetric reduction of 123I-FP-CIT uptake in the left putamen. MR imaging depicts marked hypointensity in the caudate nuclei and putamina, indicative of iron deposition, which is a feature of neuroacanthocytosis.












Tables
Distinguishing clinical features of the neurodegenerative and non-neurodegenerative causes of parkinsonism
Clinical Features of Parkinsonism (Bradykinesia, Rigidity, Tremor) Additional Helpful Clinical Features Neurodegenerative Parkinsonism Parkinson disease Yes Nil Multiple system atrophy Yes Pyramidal, autonomic, and cerebellar signs Progressive supranuclear palsy Yes Supranuclear gaze palsy, increased axial tone, bulbar palsy, early postural instability Corticobasal degeneration Yes Asymmetric cortical dysfunction Dementia with Lewy bodies Yes Fluctuating dementia, visual hallucinations, hypersensitivity to neuroleptic medications Non-neurodegenerative etiologies of parkinsonism Essential tremor Tremor Usually bilateral tremor that worsens on movement; tremor can affect head and voice Vascular parkinsonism Bradykinesia with at least one of resting tremor, rigidity, or postural instability Cerebrovascular disease diagnosed clinically or on CT/MR imaging; temporal relationship between cerebrovascular infarcts near or within the basal ganglia and acute/progressive development of parkinsonism; insidious onset of parkinsonism with bilateral symptoms at onset, presence of early shuffling gait, or cognitive dysfunction and extensive subcortical white matter lesions on MRI Drug-induced parkinsonism Yes Very difficult to distinguish clinically from neurodegenerative idiopathic Parkinson disease





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.