
Article Figures & Data
Figures
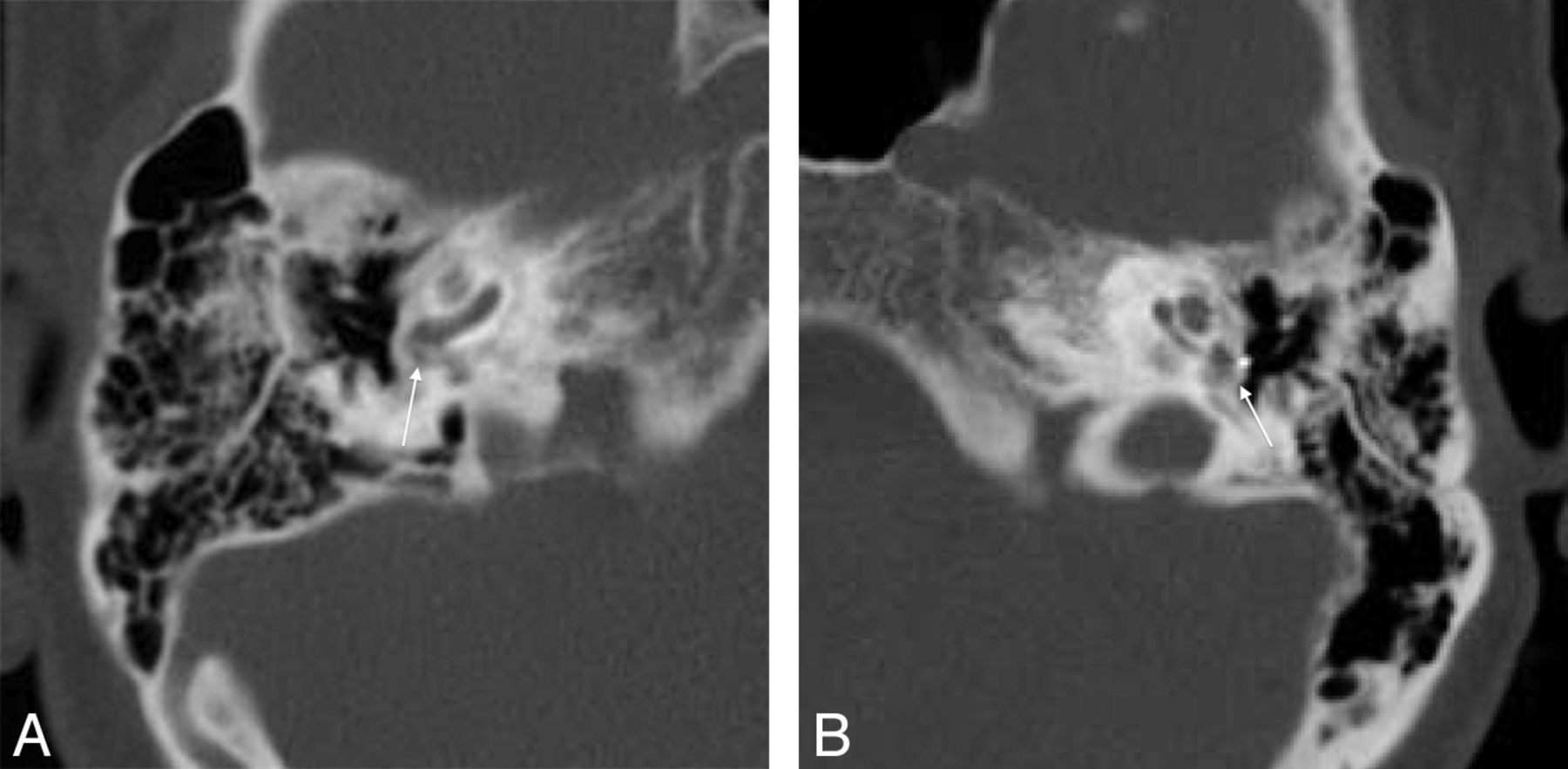
- Fig 1.
A, Axial CT in a 15-year-old girl with persistent conductive hearing loss poststapedectomy shows a small lucency in the left fissula antefenestrum (thin arrow), consistent with fenestral otosclerosis. Her piston prosthesis appeared short (thick arrow), without intravestibular penetration (surgically confirmed). B, Axial CT in a 56-year-old man with sensorineural hearing loss after stapedectomy shows extensive lucency surrounding the cochlea (arrows), consistent with cochlear otosclerosis.
- Fig 2.
A, Coronal CT in a 40-year-old woman with recurrent right conductive hearing loss after stapedectomy shows inferior dislocation of the prosthesis (arrow) with respect to the oval window. B, Coronal CT in a 15-year-old girl with CHL shows superior dislocation of the stapes prosthesis from the OW (arrow).
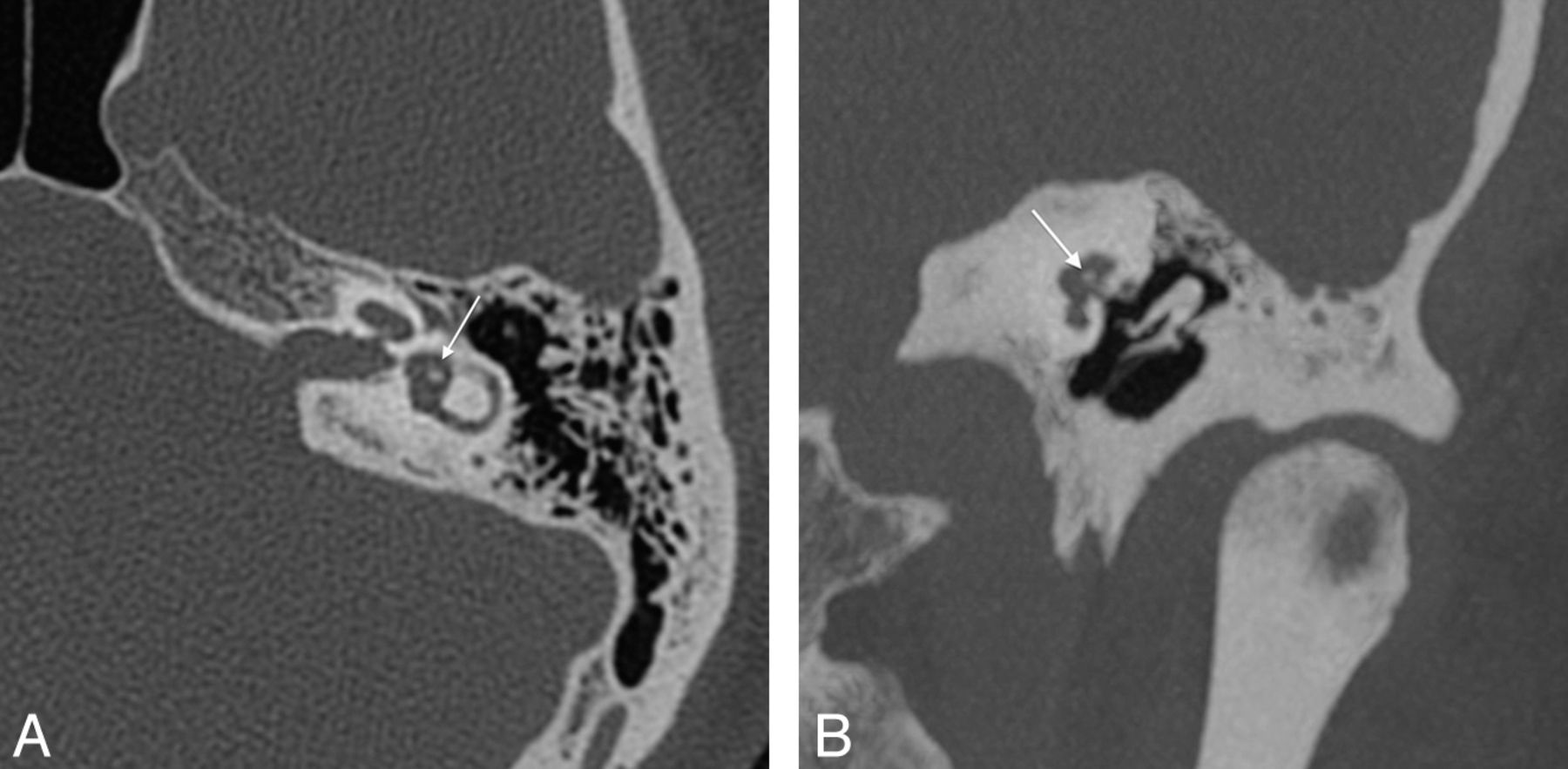
- Fig 3.
A, Axial CT in a 31-year-old woman with right conductive hearing loss after stapedectomy shows a gap (arrow) consistent with disconnected prosthesis. B, Coronal CT (same patient as in A) shows slender incus erosion and disconnection (arrow). This patient had intraoperatively confirmed disconnection and incus necrosis.
- Fig 4.
A, Axial CT in a 68-year-old man with recurrent mixed hearing loss shows findings suggesting the lateralized piston syndrome: prosthesis displacement inferior to the OW (arrow). Piston tip is encased in new otosclerotic bone. B, Coronal oblique multiplanar reformation (same patient as in A) shows incus erosion (arrow). Intraoperative findings confirmed scar tissue surrounding the stapes piston, causing prosthesis extrusion.
- Fig 5.
A, Stenver multiplanar reformation CT in a 55-year-old woman with mixed hearing loss shows findings of lateralized piston syndrome. The piston is in the oval window, but no vestibular penetration (thin arrow) is noted. Note piston lateralization to the tympanic membrane (thick arrow). B, Poschl MPR (same patient as in A) shows the piston traversing the expected location of the incus long process, which is eroded (arrow).
- Fig 6.
A, Axial CT in a 44-year-old woman with conductive hearing loss demonstrates no vestibular penetration (arrow) by the piston prosthesis. B, Coronal CT multiplanar reformation in the same patient as in A also shows no vestibular penetration (arrow), suggesting short piston. Intraoperative findings confirmed inadequate piston depth.
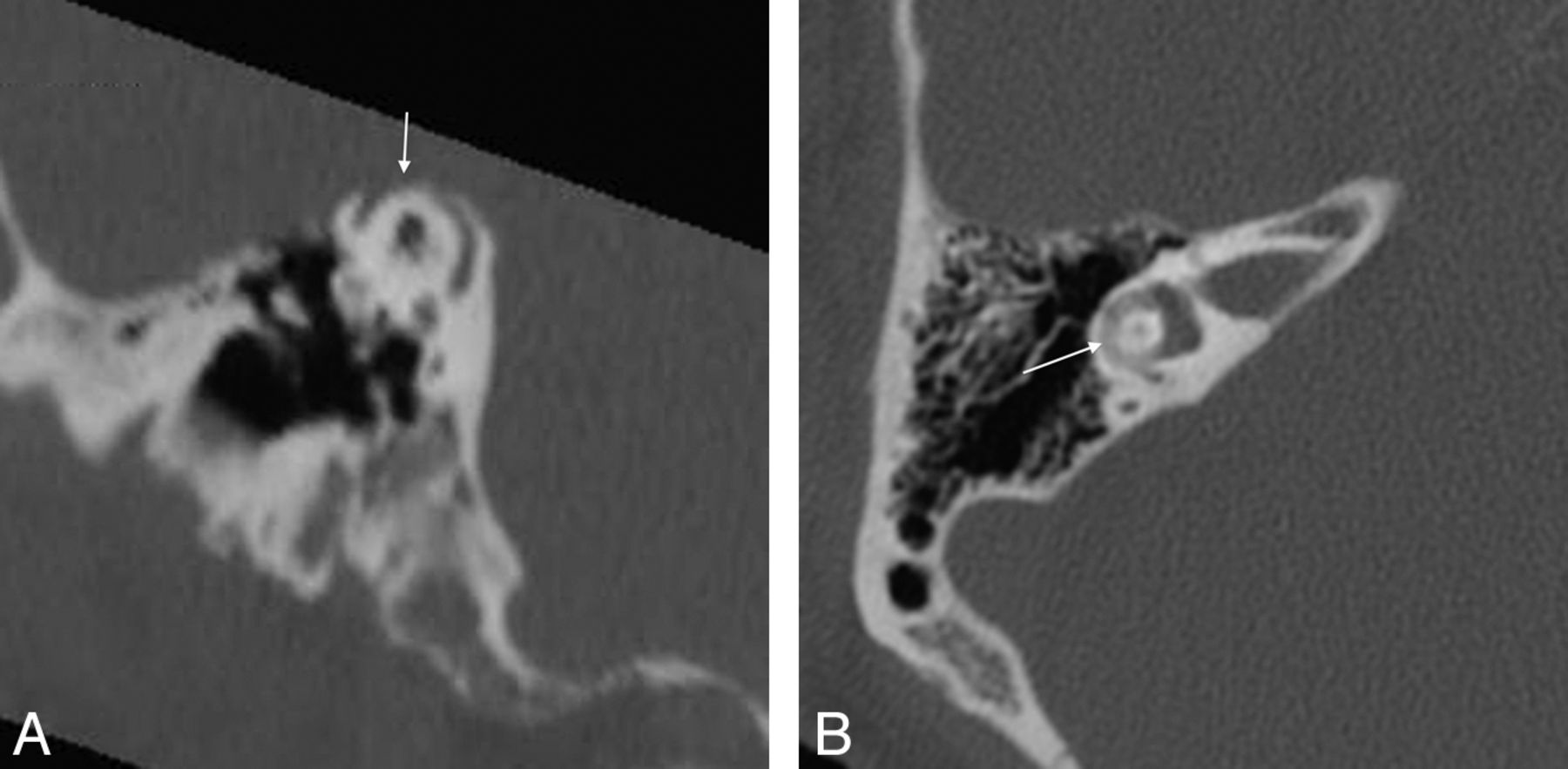
- Fig 7.
A, Axial CT in an 80-year-old man with sensorineural hearing loss shows deep intrusion into the vestibule (arrow). B, Coronal CT multiplanar reformation in a 68-year-old man with vestibular symptoms suggests deep intravestibular position of the stapes prosthesis (arrow). Long prosthesis and small labyrinthine fistula were confirmed intraoperatively.
- Fig 8.
A, Axial CT in a 56-year-old man with persistent mixed hearing loss after stapedectomy demonstrates heaped-up lucent bone formation at the right round window consistent with obliterative otosclerosis (OtoO) (arrow). This patient also had probable superior semicircular canal dehiscence (not shown). B, Axial CT in the contralateral ear in the same patient as in B also shows OtoO. Note tip of prior stapes piston embedded within otosclerotic new bone (arrow).
- Fig 9.
A, Axial CT in a 41-year-old man with vertigo and complete sensorineural hearing loss in the left ear after prior stapedectomy show focal hyperattenuation in the vestibule (arrow), consistent with intravestibular footplate dislocation. B, Coronal multiplanar reformation in the same patient as in A shows intravestibular footplate dislocation (arrow).
- Fig 10.
A, Poschl multiplanar reformation CT in a 67-year-old man with mixed hearing loss in the right ear after prior stapedectomy shows ipsilateral superior semicircular canal dehiscence (arrow) that probably explains surgical failure. B, Axial CT demonstrates ipsilateral labyrinthine ossificans (arrow) in the same patient as in A that might also have contributed to his surgical failure.










Tables
- Table 1:
Temporal bone CT findings compared with intraoperative findings and clinical presentation in patients with revision stapedectomy
Patient CT Oto Age, y Sex Presentation CT Surgery 1 B OtoF 55 F R MHL, vest R LPS with incus erosion, gas in vestibule? R LPS with incus necrosis, fistula not mentioned 2 B neg 44 F R SNHL, vest Neg R long piston 3 R OtoF 35 F L CHL, tinnitus L prosthesis dislocation from OW L long piston, loosening 4 B OtoC 68 M R MHL R LPS with disconnection, scar, incus erosion, OW dislocation R LPS with disconnection, scar, incus necrosis, OW dislocation 5 R OtoF 56 F R SNHL, vest R long piston R long piston, incus medialized 6 B OtoF 80 M L SNHL L long piston L CI (piston length unconfirmed) Clinical notes limited 7 B OtoC 56 M L MHL, vest L LO, B OtoC, B OtoO L OtoO prior surgery R MHL R CI limited notes; HL thought in part caused by OtoC 8 B neg 44 M L CHL L short piston L short piston 9 B OtoF 61 M R CHL Neg R OW dislocation, bone ingrowth 10 B neg 15 F R CHL R OW dislocation R OW dislocation, scar, OtoO 11 B OtoC 51 F R MHL R OtoO R OtoO prior surgery R CI; HL probably caused by OtoC 12 B neg 54 F R CHL R incus erosion R piston loose, incus necrosis, scar 13 R OtoF 30 F R CHL R incus erosion R stapes not crimped and scarred to incus with incus necrosis 14 B OtoF 31 F R CHL R incus erosion and disconnection, OtoO R incus erosion and disconnection, OtoO 15 R OtoF 67 F R CHL, vest Neg R nonmobile piston surrounded by scar 16 B neg 53 F R vest R long piston, incus erosion R long piston, scar, incus necrosis 17 R OtoF 52 F L vest L incus erosion, prosthesis disconnection, OW dislocation L piston medialized, disconnection, incus necrosis Note:—LPS indicates lateralized piston syndrome; CHL, conductive hearing loss; SNHL, sensorineural hearing loss; MHL, mixed hearing loss; R, right; L, left; B, bilateral; OtoF, fenestral otosclerosis; OtoC, cochlear otosclerosis; OtoO, obliterative otosclerosis; neg, negative; vest, vestibular symptoms; CI, cochlear implantation; OW, oval window; LO, labyrinthine ossificans; HL, hearing loss.
- Table 2:
Temporal bone CT findings in patients after stapedectomy with clinical confirmation only
Patient Age, y Sex CT Oto Presentation CT Findings 1 40 F B OtoF R CHL, tinnitus R prosthesis dislocation from OW 2 67 M B neg R MHL R SSCD, R LO 3 11 F B OtoF R CHL R short piston SNHL L SSCD (contralateral to operated ear) 4 41 M B neg B MHL, vertigo L intravestibular foreign body (footplate) R disconnection of prosthesis-incus, incus erosion, OW dislocation 5 58 M B OtoF L SNHL L long piston Note:—CHL indicates conductive hearing loss; SNHL, sensorineural hearing loss; MHL, mixed hearing loss; OW, oval window; SSCD, superior semicircular canal dehiscence; LO, labyrinthine ossificans; R, right; L, left; B, bilateral; OtoF, fenestral otosclerosis; neg, negative.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.