
Article Figures & Data
Figures
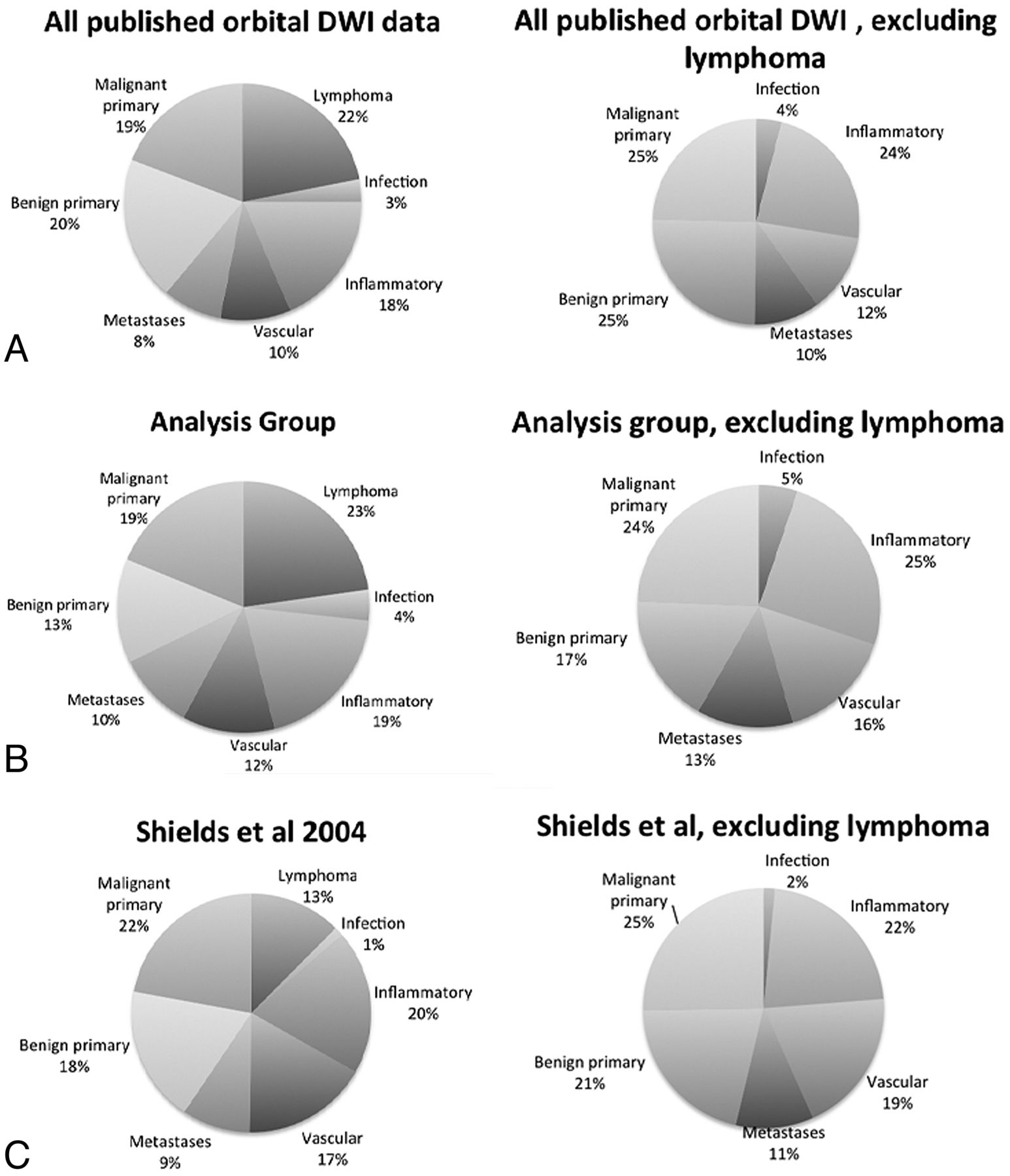
- Fig 1.
Lesion distribution by category. The left column shows the relative proportion of lesions encountered in all published studies of orbital DWI (A), in this analysis (B), and by Shields et al1 during a 30-year period (C). The published literature and our analysis group contain a higher proportion of lymphoma cases than would be predicted by Shields et al. Otherwise, the relative proportion of lesions across these 3 groups is similar, as is seen after exclusion of lymphomas (right column).
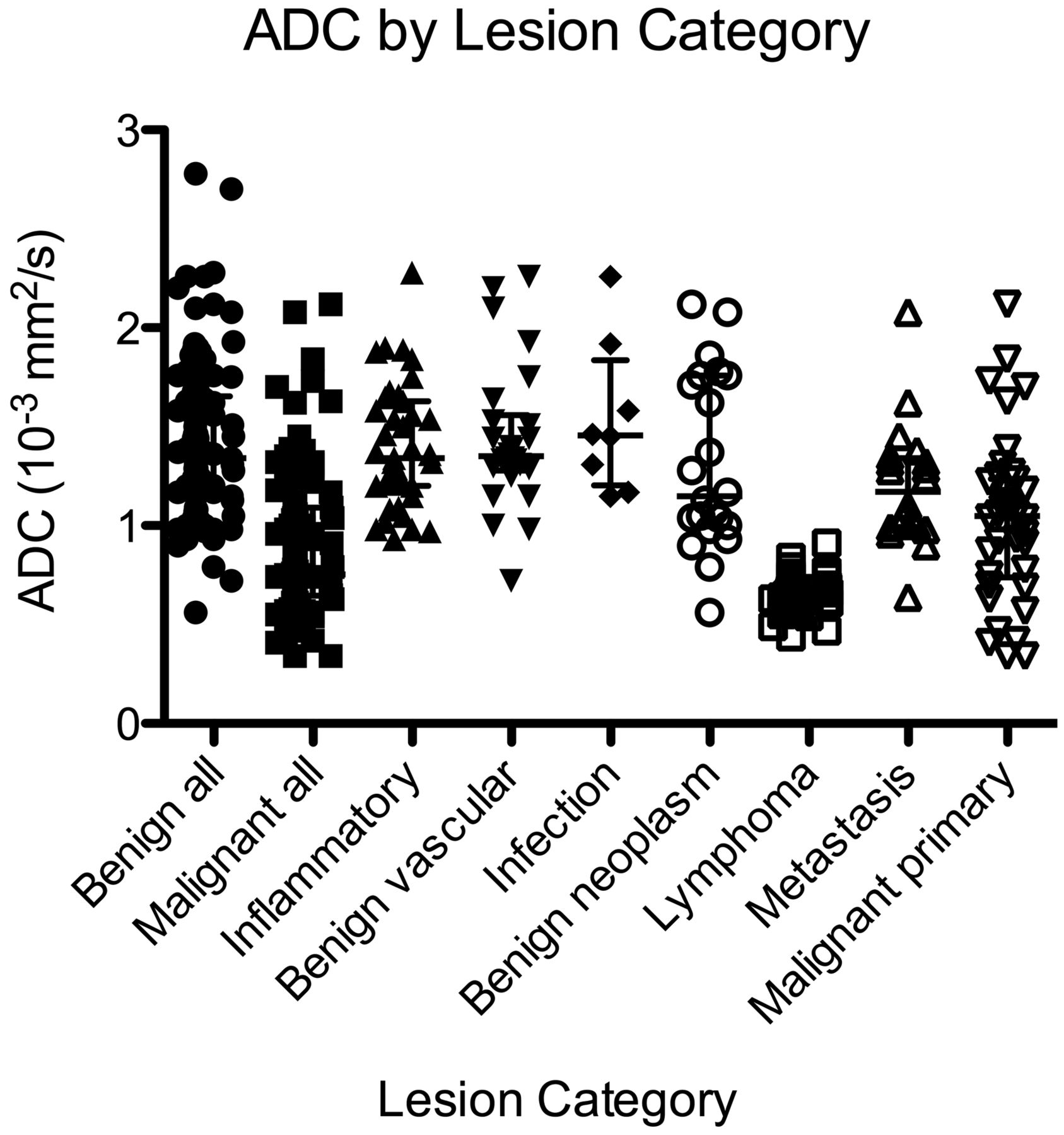
- Fig 2.
Scatterplot of ADC by lesion category shows consistently low ADC for lymphoma and a wide distribution of ADC for nonlymphoma malignancies.
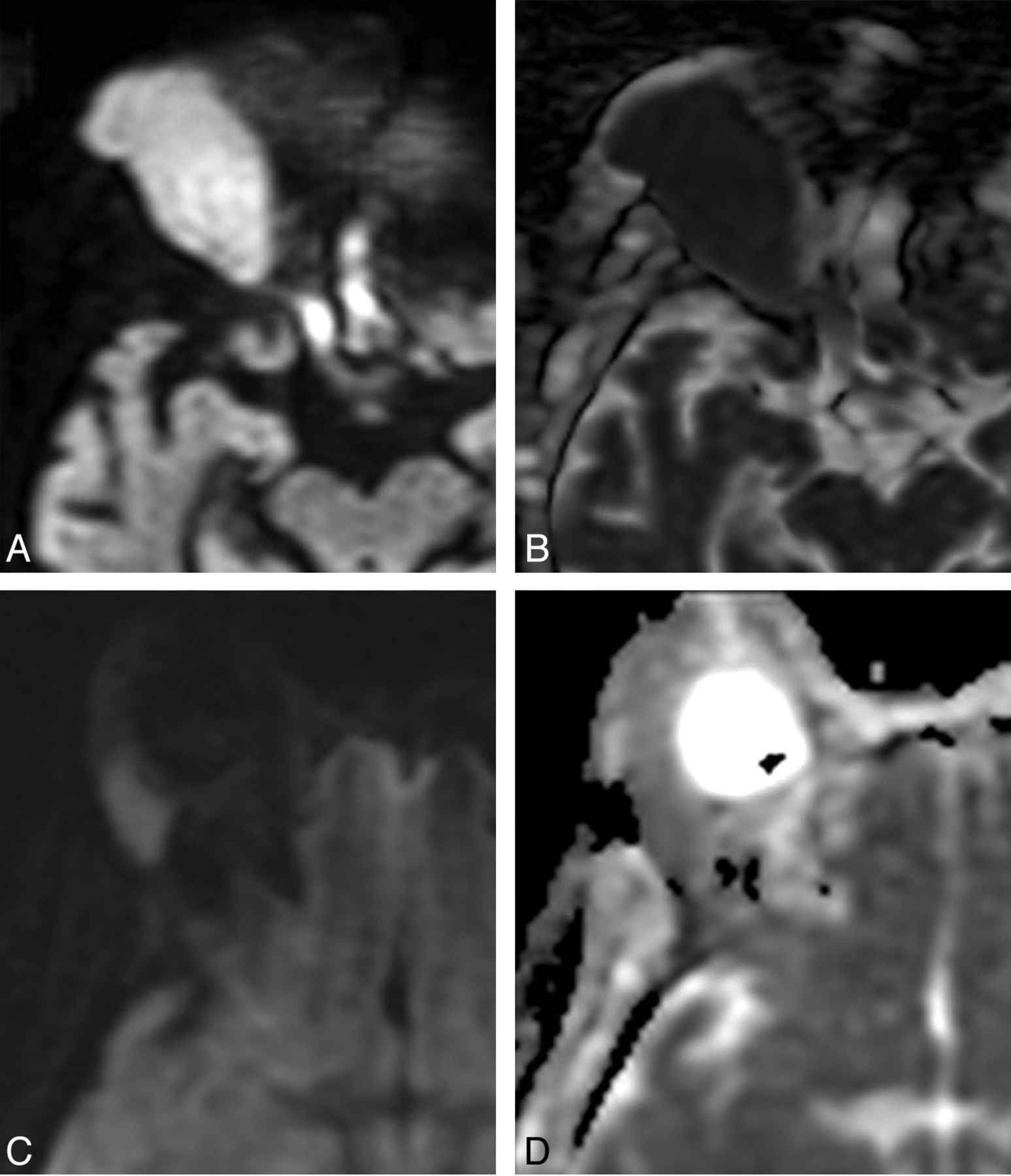
- Fig 3.
Comparison between orbital lymphoma (A and B) and orbital inflammatory disease (C and D). A, Axial DWI shows a right orbital mass with marked hyperintensity. B, Corresponding axial ADC map shows dark signal, indicating low ADC and hypercellularity typical of lymphoma. ADC of this lesion was 0.65 × 10−3 mm2/s. C, Axial DWI in a different patient shows a lacrimal gland mass with less intense signal compared with A. D, Corresponding axial ADC map shows intermediate signal, brighter than adjacent brain parenchyma, reflective of the lower cellularity seen in orbital inflammatory lesions. The ADC of this lesion was 1.09 × 10−3 mm2/s.
- Fig 4.
Receiver operating characteristic curve analysis of ADC for distinguishing benign from malignant masses (A) shows high specificities with increasing sensitivity up to 60%, at which point additional gains in sensitivity are offset by larger losses in specificity. When lymphomas are removed from the analysis (B), the performance of ADC diminishes.




Tables
- Table 1:
Distribution of lesions by category in published studies of DWI, analysis group of this study, and in the largest reported clinical series by Shields et al, 2004a
Pre-Exclusion Published Data of Orbital DWI Final Analysis Group Shields et al, 2004 Lymphoma 57 46 123 Metastasis 21 20 91 Malignant primary 50 38 219 Benign primary 51 27 182 Inflammatory 48 39 193 Vasculogenic 25 24 169 Infection 8 8 13 ↵a Any lesions from the Shields et al1 series that were likely to be excluded in studies of orbital DWI were removed. Capillary hemangioma was categorized as a benign primary tumor, reflecting current understanding. Nonmalignant lymphocytic or histiocytic processes were categorized as inflammatory disease.
Lesion (No.) ADC (10−3 mm2/s) (mean ± SD) Range Benign (98) 1.42 ± 0.41 0.72–2.78 Inflammatory (39) 1.40 ± 0.31 0.93–2.28 Cavernous hemangioma (ie, encapsulated venous malformation) (12) 1.23 ± 0.20 0.73–1.44 Optic nerve sheath meningioma (11) 0.99 ± 0.20 0.56–1.28 Other vascular (15) 1.58 ± 0.40 0.98–2.26 Other benign (22) 1.67 ± 0.51 1.00–2.78 Malignant (104) 0.90 ± 0.37 0.34–2.08 Lymphoma (46) 0.66 ± 0.09 0.44–0.91 Metastasis (20) 1.20 ± 0.31 0.64–2.08 Rhabdomyosarcoma (12) 0.72 ± 0.31 0.34–1.31 Carcinoma (9) 1.15 ± 0.12 1.04–1.39 Other malignant (17) 1.19 ± 0.47 0.34–2.12 - Table 3:
Descriptive statistics of orbital lesion ADC across the largest source datasets (ADC in units of 10−3 mm2/s)
All Lesions (n = 183) Sepahdari et al13 (n = 50) Politi et al17 (n = 90) Razek et al16 (n = 43) Benign lesion ADC (mean, 95% CI) 1.42 ± 0.41 (1.34–1.51) 1.36 ± 0.41 (1.22–1.51) 1.39 ± 0.42 (1.25–1.54) 1.53 ± 0.35 (1.37–1.67) Malignant lesion ADC (mean, 95% CI) 0.90 ± 0.37 (0.83–0.98) 1.02 ± 0.42 (0.80–1.24) 0.88 ± 0.36 (0.79–0.98) 0.80 ± 0.34 (0.65–0.95) Lymphoma ADC (mean, 95% CI) 0.67 ± 0.09 (0.64–0.69) 0.69 ± 0.16 (0.58–0.86)a 0.67 ± 0.07 (0.60–0.75) 0.67 ± 0.07 (0.60–0.73)a Inflammatory lesion ADC (mean, 95% CI) 1.40 ± 0.31 (1.30–1.50) 1.42 ± 0.37 (1.24–1.60) 1.45 ± 0.26 (1.29–1.60) 1.24 ± 0.13 (1.18–1.33)a Area under ROC curve (95% CI) 0.84 (0.79–0.90) 0.74 (0.58–0.89) 0.86 (0.79–0.94) 0.95 (0.87–1.0) ↵a The 25th-75th percentile range was reported due to a sample size too small to assume normal distribution.
- Table 4:
Sensitivity and specificity of various ADC threshold values for distinguishing benign from malignant lesions
ADC (10−3 mm2/s) Sensitivity (%) Specificity (%) Likelihood Ratio of Positive Results 0.72 40 99 39 0.82 54 97 17 0.93 60 96 14 1.03 67 85 4.3 1.13 77 77 3.4 1.23 80 66 2.3 1.33 89 54 1.8 1.42 92 41 1.6 1.52 93 34 1.4





{kind=link}
{kind=link}
{kind=link}
{kind=link}