
Article Figures & Data
Figures
- Fig 1.
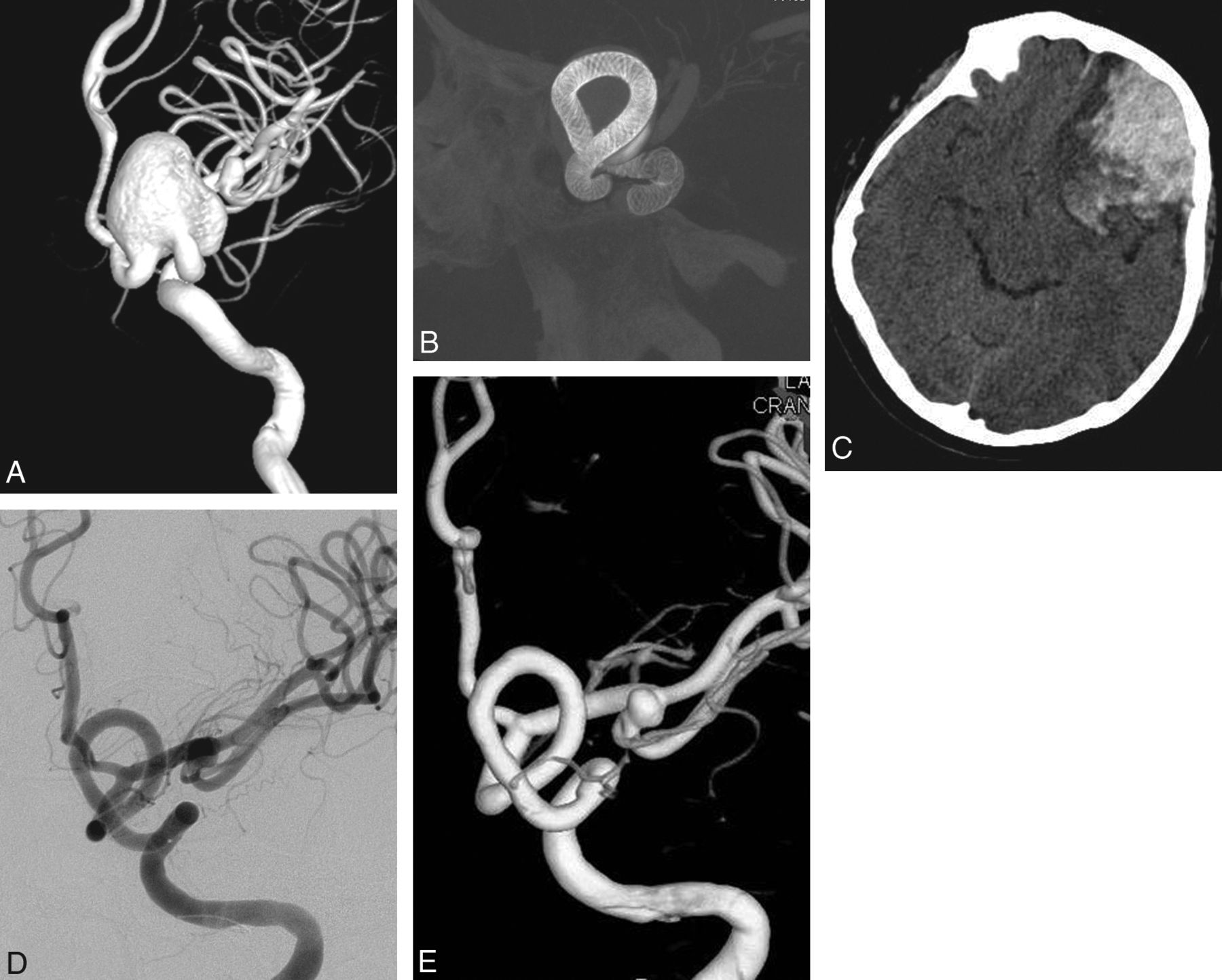
Preoperative 3D angiogram (A) shows a very wide-neck large ICA aneurysm. It could be reconstructed with several overlapping devices, creating a new vessel wall within the sac as seen on the perioperative DynaCT image (B). Postoperative CT obtained the same evening (C) reveals ipsilateral frontal intraparenchymal hemorrhage. 2D (D) and 3D (E) views of 6-month control angiography demonstrate the reconstruction of the parent artery and total occlusion of the aneurysm.
- Fig 2.
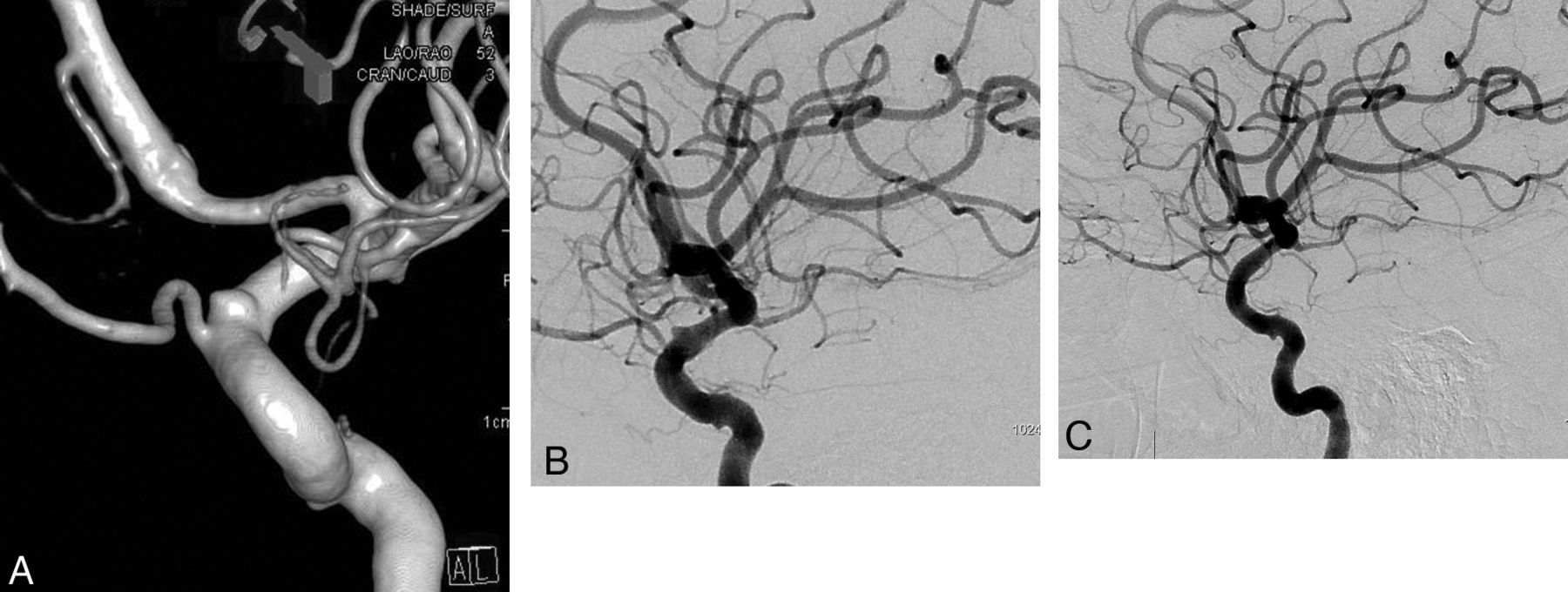
Lateral angiogram shows a giant dissecting ICA aneurysm (A). The intraoperative view demonstrates PEDs (sizes, 4 × 202 and 4.5 × 16 mm) opening to the normal size of the parent artery at the dissected segment (arrow in A) without necessitating balloon angioplasty. Note the contrast stagnation within the sac (B). Six-month control angiography (C) shows total occlusion of the aneurysm and reconstruction of the parent artery.
- Fig 3.
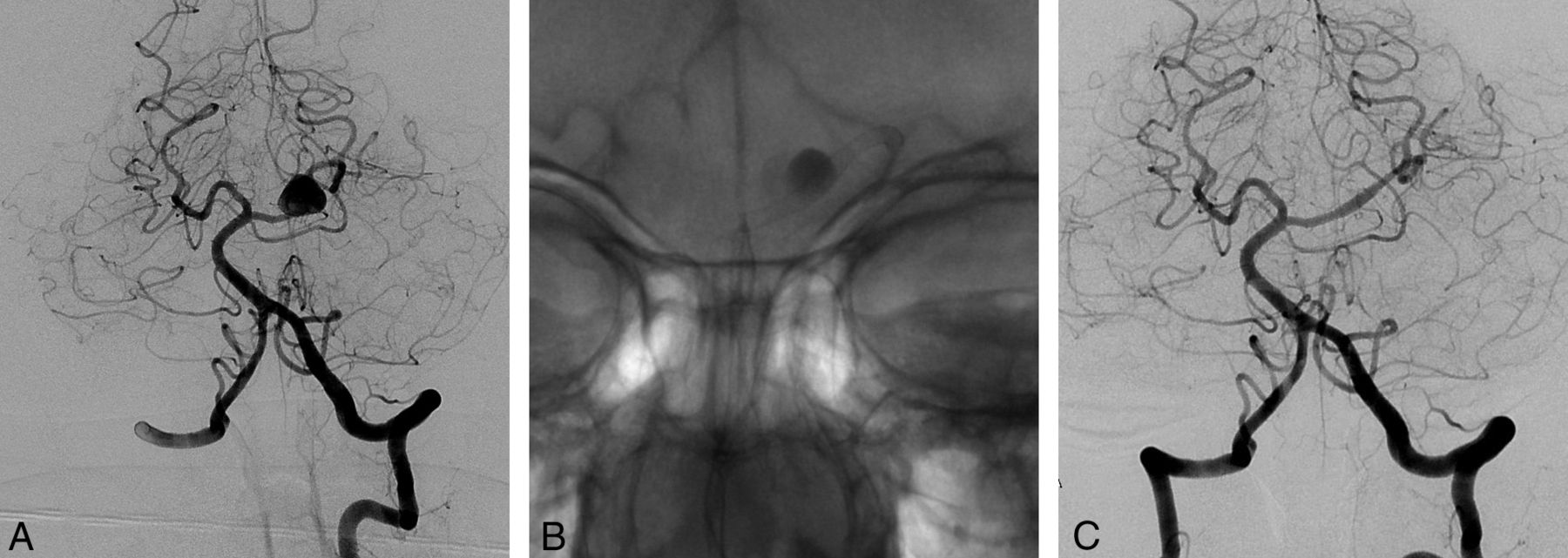
Left vertebral angiogram (A) demonstrates the left PCA aneurysm, which presented with left thalamic infarct (not shown). Immediate postoperative view (B) shows the single PED (2.5 × 20 mm) placed in the left PCA, resulting in contrast stasis within the sac. Control angiography (C) after 6 months confirms total occlusion of the aneurysm with the PCA preserved.
- Fig 4.
3D image (A) and lateral angiography (B) show a left paraophthalmic bleb aneurysm in a patient who had a subarachnoid hemorrhage 3 months earlier. Lateral angiogram 6 months after placement of a single PED of 3.75 × 12 mm (C) demonstrates complete occlusion of the aneurysm.
- Fig 5.
Right carotid angiogram (A) demonstrates a small carotid cave aneurysm in a patient who had an anterior communicating artery aneurysm previously treated with coiling following SAH. Six-month control angiography (B) shows occlusion of the aneurysm.
- Fig 6.
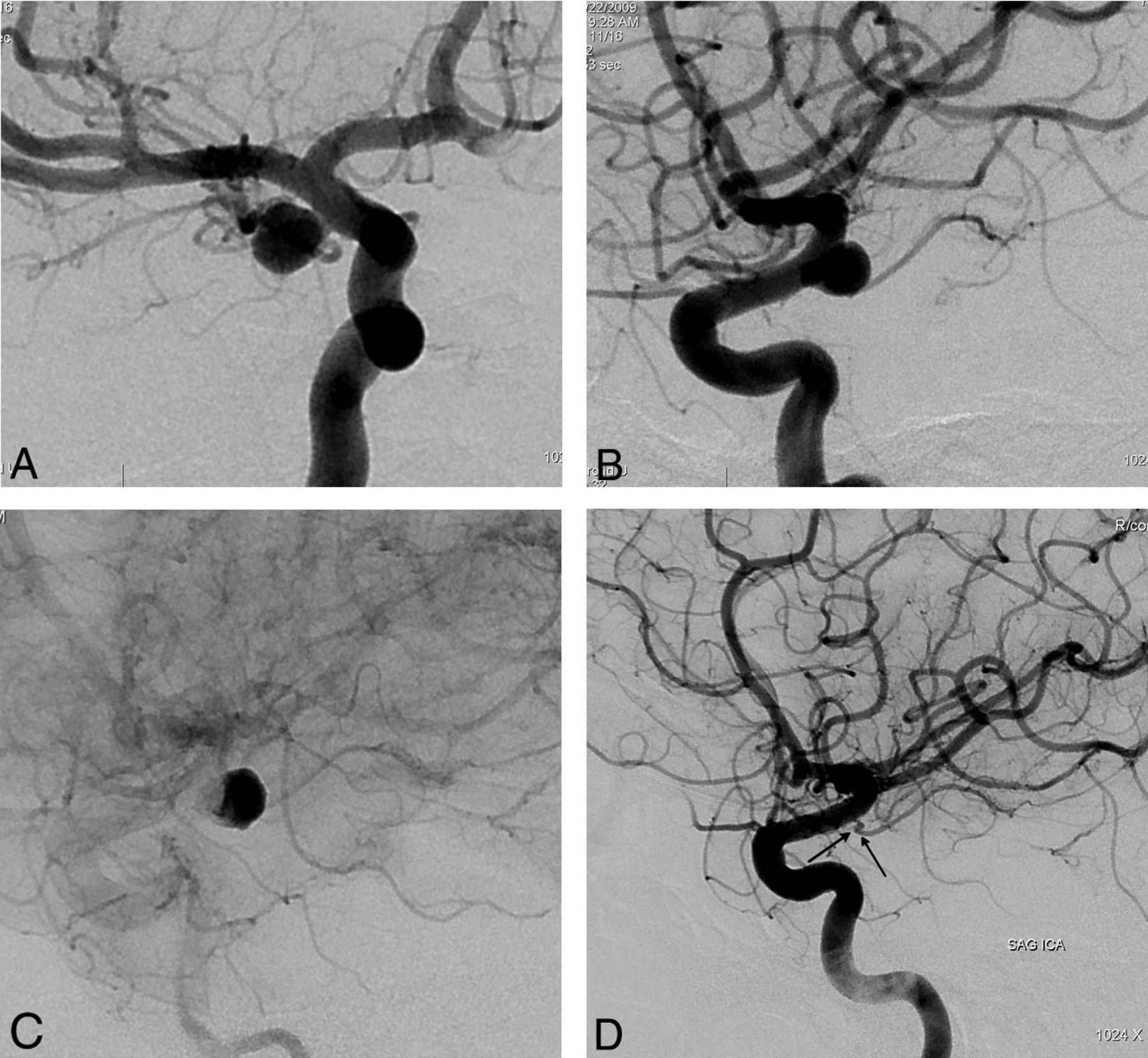
Preoperative 2D (A and B) angiograms show the ICA aneurysm in which the anterior choroidal artery is originating from the aneurysm at the neck. A single PED is placed covering the neck, causing stagnation of the contrast within the sac (C). Six-month control angiography (D) demonstrates total occlusion of the aneurysm with the anterior choroidal artery preserved (arrow).
- Fig 7.
Right internal carotid oblique angiogram (A) shows a right posterior communicating artery aneurysm (the ipsilateral P1 is aplastic and not shown) in a patient in whom previous endovascular attempts and clipping had failed, with surgical wrapping performed eventually. Two years after a single PED placement, the aneurysm is remodeled in the corresponding view (B).







Tables
Presentation No. of Patients % Incidentala 23 12 Headache 83 43.5 Subarachnoid hemorrhageb 31c,d 16.2 Previous SAH from another aneurysm 19 10 Visual findings due to mass effect 28d 14.7 Othere 8 4.2 Total 191d 100 ↵a Incidental group includes asymptomatic patients and patients with symptoms (excluding SAH) unrelated to the aneurysms treated with a PED (ie, index aneurysms).
↵b SAH from the aneurysm treated with a PED.
↵c Nine of these patients, 6 of whom were in the acute stage, were treated with the Pipeline as the first treatment; 22 patients had a PED in the retreatment.
↵d One of these patients had visual findings after the initial treatment and received a PED as a retreatment; this patient is cited in both groups.
↵e All symptoms (eg, ataxia, paresthesia, hemi-/quadriparesis, and so forth) other than those listed above, which may be due to mass effect and/or ischemia (such as perforator injury) and so forth.
- Table 2:
The previous treatments in the aneurysms that had Pipeline treatment for incomplete occlusion
Previous Treatment No. of Aneurysms/Patients Coiling with bare coils 18/17 Coiling with surface modified coils 2 Stent-assisted coiling 2 Bare stenting 2 Onyx 1 Silk flow diverter 2/1 Failed surgery 5 Surgical remnant/regrowth 2 Total 34/32 Localization No. of Aneurysms Ratio (%) Petrous ICA 6 2.4 Cavernous ICAa 28 11.2 Supraclinoid aneurysmb 134 53.4 PcomA aneurysms 21 8.4 AchoA aneurysms 28 11.2 ICA terminal bifurcation 3 1.2 M1 5 2 MCA bifurcation 2 0.8 Basilar arteryc 6 2.4 Vertebral arteryd 8 3.2 Distal aneurysmse 10 4 Total 251 100 Note:—AchoA indicates anterior choroidal artery.
↵a If the aneurysm involved both petrous and cavernous segments, it is included in this group, and this definition applies to 12/28 aneurysms in this group.
↵b The aneurysm is included in the supraclinoid group when it involves this segment, regardless of whether it extends to more than this segment proximally (eg, to the cavernous segment). The aneurysms at the posterior communicating and anterior choroidal artery origins and the terminal bifurcation are shown separately and are not included in this group.
↵c This group includes 1 superior cerebellar artery origin aneurysm and 2 aneurysms involving the vertebrobasilar junction in addition to 3 basilar trunk aneurysms.
↵d Three aneurysms at the origin of PICA are included in this group.
↵e This group includes all aneurysms distal to the MCA bifurcation, all anterior cerebral artery aneurysms excluding the ones located at the ICA termination, and any aneurysm distal to basilar termination (ie, posterior cerebral artery aneurysms).
Adverse Events No. of Patients Permanent Morbidity/Mortality Due to medication Intracranial hemorrhage 2 1 Aplastic anemiaa 1 No Hematuria (requiring change in medical treatment) 1 No GI bleeding (including the FU period) 2 No Associated with intervention Deep vein thrombosis 1 No Retroperitoneal hematomab 3 No Associated with aneurysm treatment Due to mass effectc 4 1 SAH (aneurysm rupture) 1 Nod In relation to PED Perioperative thromboembolic event 4 1) Mortality (jailed PCA occlusion) 3) Symptoms resolved totallye In-stent stenosisf 8 No Mild 5 No intervention Severe 3 PTAs performedg Ischemic event in the FU period 1e Total 27 (14.1%)e 2 (1%)/1 (0.5%) Note:—FU indicates follow-up; GI, gastrointestinal; PTA, percutaneous transarterial angioplasty.
↵a Occurred in the patient who had resistance to clopidogrel and was on ticlopidine.
↵b Included in the group of complications that are attributed to intervention, but antithrombocytic medication may also have contributed.
↵c Any new symptom or increase in the findings are taken into consideration; 3 had deteriorating vision loss, of whom 2 also had visual field defects. In 2 patients, the symptoms regressed to their preoperative degree in the follow-up and caused permanent additional morbidity in 1. The remaining patient had symptoms due to mass effect on the brain stem, aggravated after the treatment, but resolved in 4 weeks' time.
↵d This patient had subarachnoid hemorrhage 4 months after the treatment; imaging still showed filling of the aneurysm despite significant decrease. Initially she had had hemiparesis, but this resolved totally.
↵e One patient had an ischemic attack in the postoperative 4 months after he discontinued clopidogrel without consulting his doctor. The patient was medicated with IV heparin, and clopidogrel was loaded again. The symptom of monoparesis resolved totally. The same patient woke up from the general anesthesia with monoparesis but immediately became asymptomatic after volume loading and raising the blood pressure.
↵f Mild refers to any intimal thickening causing stenosis <50%. Severe refers to stenosis ≥50%.
↵g In 2 patients, stenosis was discovered in the control angiography but PTA was performed because the stenosis was considered significant (>70%). The remaining patient had attacks of dysphasia which resolved after PTA, with no permanent morbidity.
Degree of Occlusion Small Large Giant Total No. % Total occlusion (%) 136 (93.8%) 56 (87.5%) 27 (90%) 219b 91.6b–91.2c Still filling 9 8 3 20d 8.4% Total 145 64 30 239a 100 ↵a One patient with 1 aneurysm died after the treatment; 8 patients with 11 aneurysms (9 small and 2 large) have not yet undergone the 6-month control angiography. Therefore, a total of 12 aneurysms (4.8%) did not have control angiography.
↵b Including 1 patient who had subarachnoid hemorrhage in the fourth month and was retreated with additional PEDs for her remaining aneurysm filling.
↵c Represents the ratio of aneurysms that were occluded in the 6-month control without retreatment.
↵d Seven were retreated. Seven of the remaining showed further thrombosis with resultant aneurysm occlusion, and 6 are pending the next control after the discontinuation of the clopidogrel.
Series No. of Patients/AA No of AA W Previous TX Failurea (%) No of AA Treated W Adjunctive Coilingb (%) Morbidityc and Mortality Complete Occlusion at 6-Month DSA (%) Control Angiography (%) Retx No of AA (%) Peri-Post-Operative Intracranial Bleeding Perforator Infarct In-Stent Stenosis All %/Requiring TX % PAO Lylyk et al 200920,d 53/63 23/63 4/63 (6%) 0 93% 100% 0 0 0 10%/0 (37%) 0% PAO: 0 Szikora et al 201021,e 18/19 1/19 10/19 (53%) 5.6% 94.4% 94.7% 0 1/18f 0 0 (5.3%) 5.6% 5.6% PAO:5.6% Nelson et al 201123 31/31 12/31 16/31 (52%) 6.5% 93.3% 96.8% 0 1/31g 1/31 0 (38.7%) 0% 3.2% (3.2%) PAO:0 Fischer et al 201124 88/101 30/101) 3/101 (3%) 4% 52% 89% 8/101 4/88h 0 2.3%/0 (29.7%) 2% 7.9% 4.6% PAO:2.3% McAuliffe et al 201234 54/57 16/57 12/68 (18%) 0 85.7% 98.2% 2/57i 0 0 3.5%/0 (28.1%) 0% 3.5% PAO:0 Saatci et al 2012 191/251 34/251 11/251 (4%) 1% 91.2 % 95.2 % 8/251 3/191j 1/191 4.2%/1.6% (13.5%) 0.5% 3.2% 1.6% 0.5% PAO:0 Note:—AA indicates aneurysms; TX, treatment; W, with DSA; Retx retreatment.
↵a Refers to the aneurysms that underwent previous endovascular or surgical treatment, including the failed treatment, incomplete treatment, and recurrences.
↵b Refers to the aneurysms in which coiling was performed as an adjunctive treatment in the same session with PED placement.
↵c Temporary deficits not included.
↵d,e Six (d) and 9 (e) aneurysms of these series were also included in the PITA trial.
↵f Refers to the rupture of a coexisting aneurysm.
↵g Refers to an iatrogenic ICA rupture.
↵h Includes 1 aneurysm rupture and 3 parenchymal hemorrhages.
↵i Additional treatment required due to PED displacement in 2 aneurysms.
↵j Includes 1 aneurysm rupture and 2 parenchymal hemorrhages.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Excessive platelet inhibition following Pipeline embolization of intracranial aneurysms
- Prospective study on embolization of intracranial aneurysms with the pipeline device (PREMIER study): 3-year results with the application of a flow diverter specific occlusion classification
- First clinical multicenter experience with the new Pipeline Vantage flow diverter
- Recovery from Cranial Nerve Symptoms after Flow Diversion without Coiling for Unruptured Very Large and Giant ICA Aneurysms
- The utility of platelet inhibition testing in patients undergoing Pipeline embolization of intracranial aneurysms
- Predictors of the Effects of Flow Diversion in Very Large and Giant Aneurysms
- Outcome of intracranial flow diversion according to the antiplatelet regimen used: a systematic review and meta-analysis
- Outcome Study of the Pipeline Embolization Device with Shield Technology in Unruptured Aneurysms (PEDSU)
- Pipeline embolization device diameter is an important factor determining the efficacy of flow diversion treatment of small intracranial saccular aneurysms
- A Multicenter Pilot Study on the Clinical Utility of Computational Modeling for Flow-Diverter Treatment Planning
- Evaluating the safety and technical effectiveness of a newly developed intravascular flow isolator' stent for the treatment of intracranial aneurysms: study protocol for a first-in-human single-arm multiple-site clinical trial in Japan
- Antiplatelet therapy and the risk of ischemic and hemorrhagic complications associated with Pipeline embolization of cerebral aneurysms: a systematic review and pooled analysis
- Safety and efficacy of the Derivo Embolization Device for the treatment of ruptured intracranial aneurysms
- Pipeline Diameter Significantly Impacts the Long-Term Fate of Jailed Side Branches during Treatment of Intracranial Aneurysms
- Toward Better Understanding of Flow Diversion in Bifurcation Aneurysms
- Endovascular Treatment of Very Large and Giant Intracranial Aneurysms: Comparison between Reconstructive and Deconstructive Techniques--A Meta-Analysis
- Expanding the use of flow diverters beyond their initial indication: treatment of small unruptured aneurysms
- P2Y12 hyporesponse (PRU>200) is not associated with increased thromboembolic complications in anterior circulation Pipeline
- Use of flow diverters in the treatment of unruptured saccular aneurysms of the anterior cerebral artery
- Flow Diversion in Ruptured Intracranial Aneurysms: A Meta-Analysis
- Concomitant coiling reduces metalloproteinase levels in flow diverter-treated aneurysms but anti-inflammatory treatment has no effect
- Middle Cerebral Artery Bifurcation Aneurysms Treated by Extrasaccular Flow Diverters: Midterm Angiographic Evolution and Clinical Outcome
- Mid-term and long-term follow-up of intracranial aneurysms treated by the p64 Flow Modulation Device: a multicenter experience
- Efficacy and Safety of the Woven EndoBridge (WEB) Device for the Treatment of Intracranial Aneurysms: A Systematic Review and Meta-Analysis
- Republished: Pipeline embolization device thrombosis induced peri-construct collateral channels
- Intra-DIC (distal intracranial catheter) deployment of the Pipeline embolization device: a novel rescue strategy for failed device expansion
- Pipeline Embolization Device with or without Adjunctive Coil Embolization: Analysis of Complications from the IntrePED Registry
- Current Trends and Results of Endovascular Treatment of Unruptured Intracranial Aneurysms at a Single Institution in the Flow-Diverter Era
- Flow diversion treatment of complex bifurcation aneurysms beyond the circle of Willis: a single-center series with special emphasis on covered cortical branches and perforating arteries
- Preclinical Testing of a Novel Thin Film Nitinol Flow-Diversion Stent in a Rabbit Elastase Aneurysm Model
- Flow diversion of large internal carotid artery aneurysms with the surpass device: impressions and technical nuance from the initial North American experience
- Retrospective Analysis of Delayed Intraparenchymal Hemorrhage after Flow-Diverter Treatment: Presentation of a Retrospective Multicenter Trial
- In Vitro Evaluation of Intra-Aneurysmal, Flow-Diverter-Induced Thrombus Formation: A Feasibility Study
- Flow diverter device for the treatment of small middle cerebral artery aneurysms
- Intravenous C-Arm Conebeam CT Angiography following Long-Term Flow-Diverter Implantation: Technologic Evaluation and Preliminary Results
- Technology developments in endovascular treatment of intracranial aneurysms
- p64 Flow Modulation Device in the treatment of intracranial aneurysms: initial experience and technical aspects
- A New Aneurysm Occlusion Classification after the Impact of Flow Modification
- Effect of antiplatelet therapy and platelet function testing on hemorrhagic and thrombotic complications in patients with cerebral aneurysms treated with the pipeline embolization device: a review and meta-analysis
- Flow Diversion versus Standard Endovascular Techniques for the Treatment of Unruptured Carotid-Ophthalmic Aneurysms
- Hemodynamic analysis of fast and slow aneurysm occlusions by flow diversion in rabbits
- Pipeline embolization device thrombosis induced peri-construct collateral channels
- Focal, transient mechanical narrowing of a pipeline embolization device following treatment of an internal carotid artery aneurysm
- Evolution of Flow-Diverter Endothelialization and Thrombus Organization in Giant Fusiform Aneurysms after Flow Diversion: A Histopathologic Study
- Flow diverter stents for unruptured saccular anterior circulation perforating artery aneurysms: safety, efficacy, and short-term follow-up
- Periprocedural and mid-term technical and clinical events after flow diversion for intracranial aneurysms
- Long-Term Follow-Up Results following Elective Treatment of Unruptured Intracranial Aneurysms with the Pipeline Embolization Device
- A reappraisal of the Pipeline embolization device for the treatment of posterior circulation aneurysms
- Use of thromboelastography to tailor dual-antiplatelet therapy in patients undergoing treatment of intracranial aneurysms with the Pipeline embolization device
- Mechanical properties and fibrin characteristics of endovascular coil-clot complexes: relevance to endovascular cerebral aneurysm repair paradigms
- Small Pipes: Preliminary Experience with 3-mm or Smaller Pipeline Flow-Diverting Stents for Aneurysm Repair prior to Regulatory Approval
- Patency of the Anterior Choroidal Artery after Flow-Diversion Treatment of Internal Carotid Artery Aneurysms
- Endovascular treatment with flow diverters of recanalized and multitreated aneurysms initially treated by endovascular approach
- Cavernous Carotid Aneurysms in the Era of Flow Diversion: A Need to Revisit Treatment Paradigms
- Heterogeneous practice patterns regarding antiplatelet medications for neuroendovascular stenting in the USA: a multicenter survey
- Modifying Flow in the ICA Bifurcation: Pipeline Deployment from the Supraclinoid ICA Extending into the M1 Segment--Clinical and Anatomic Results
- Platelet function inhibitors and platelet function testing in neurointerventional procedures
- Focal, transient mechanical narrowing of a pipeline embolization device following treatment of an internal carotid artery aneurysm
- Effect of Structural Remodeling (Retraction and Recoil) of the Pipeline Embolization Device on Aneurysm Occlusion Rate
- A Single Pipeline Embolization Device is Sufficient for Treatment of Intracranial Aneurysms
- Novel application of a balloon-anchoring technique for the realignment of a prolapsed Pipeline Embolization Device: a technical report
- Flow diversion versus traditional aneurysm embolization strategies: analysis of fluoroscopy and procedure times