
Article Figures & Data
Figures
- Fig 1.
Congenital cholesteatoma. Coronal (A) and axial HRCT (B) scans demonstrate a round well-defined lesion (arrow) anterosuperior in the tympanic cavity, medial to the ossicular chain. Note the missing ossicular erosion. Based on the position of the lesion and the lack of bone erosion along with the clinical aspects, this is probably a congenital type.
- Fig 2.
Cholesteatoma of the petrous apex. Contrast-enhanced HRCT scans with a soft-tissue window (A) and a bone window (B) show an oval well-delineated, nonenhancing lesion (white arrows) with erosion of the posterior wall of the pyramidal segment of the internal carotid artery (thin black arrow) and the anterior wall of the jugular bulb (thick black arrow). C, DWI demonstrates diffusion restriction in the lesion (white arrow), supporting the diagnosis of a cholesteatoma.
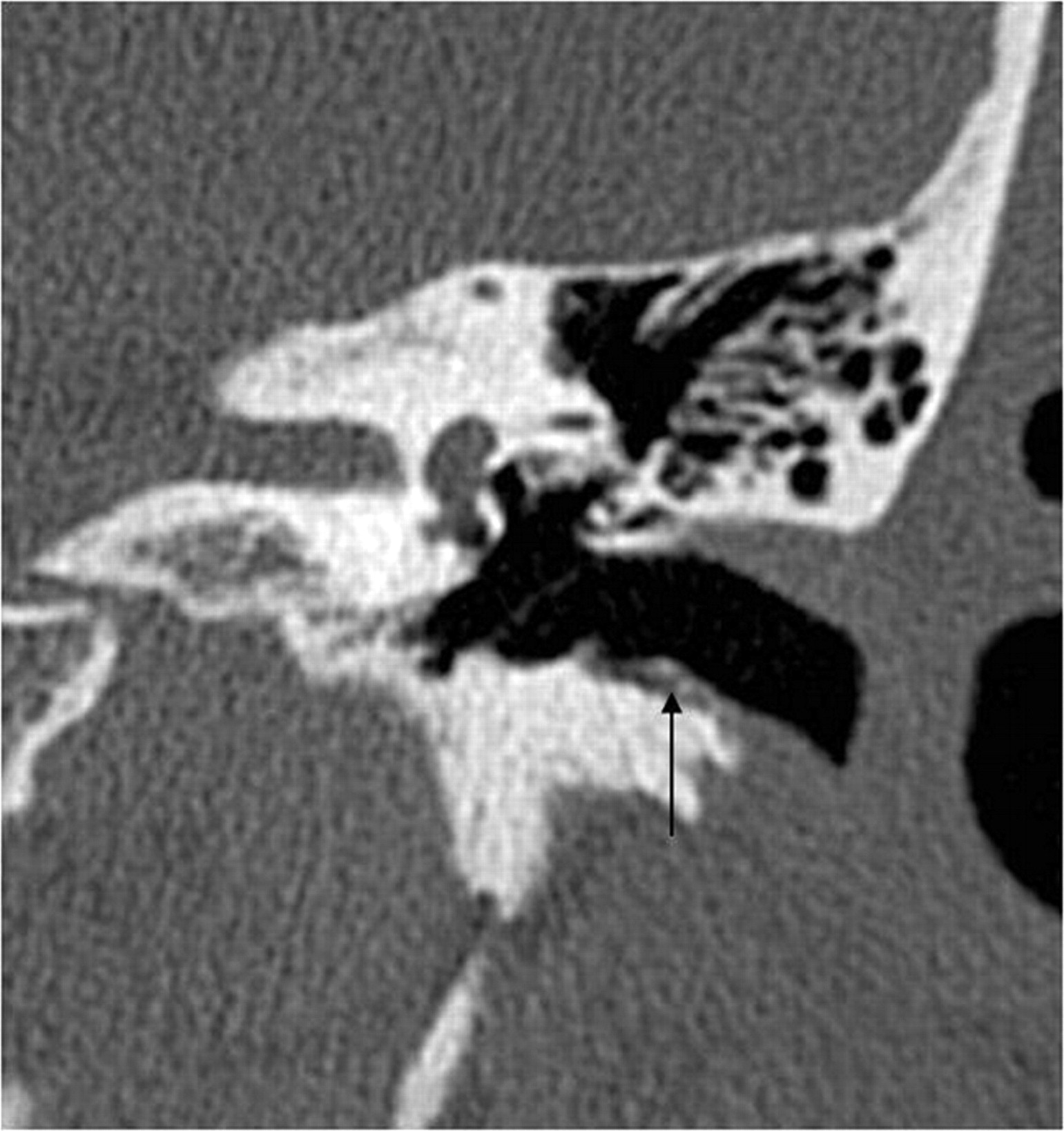
- Fig 3.
EAC cholesteatoma (arrow). Note the typical localization at the inferior wall of the EAC and the small bone fragments along the lesion.
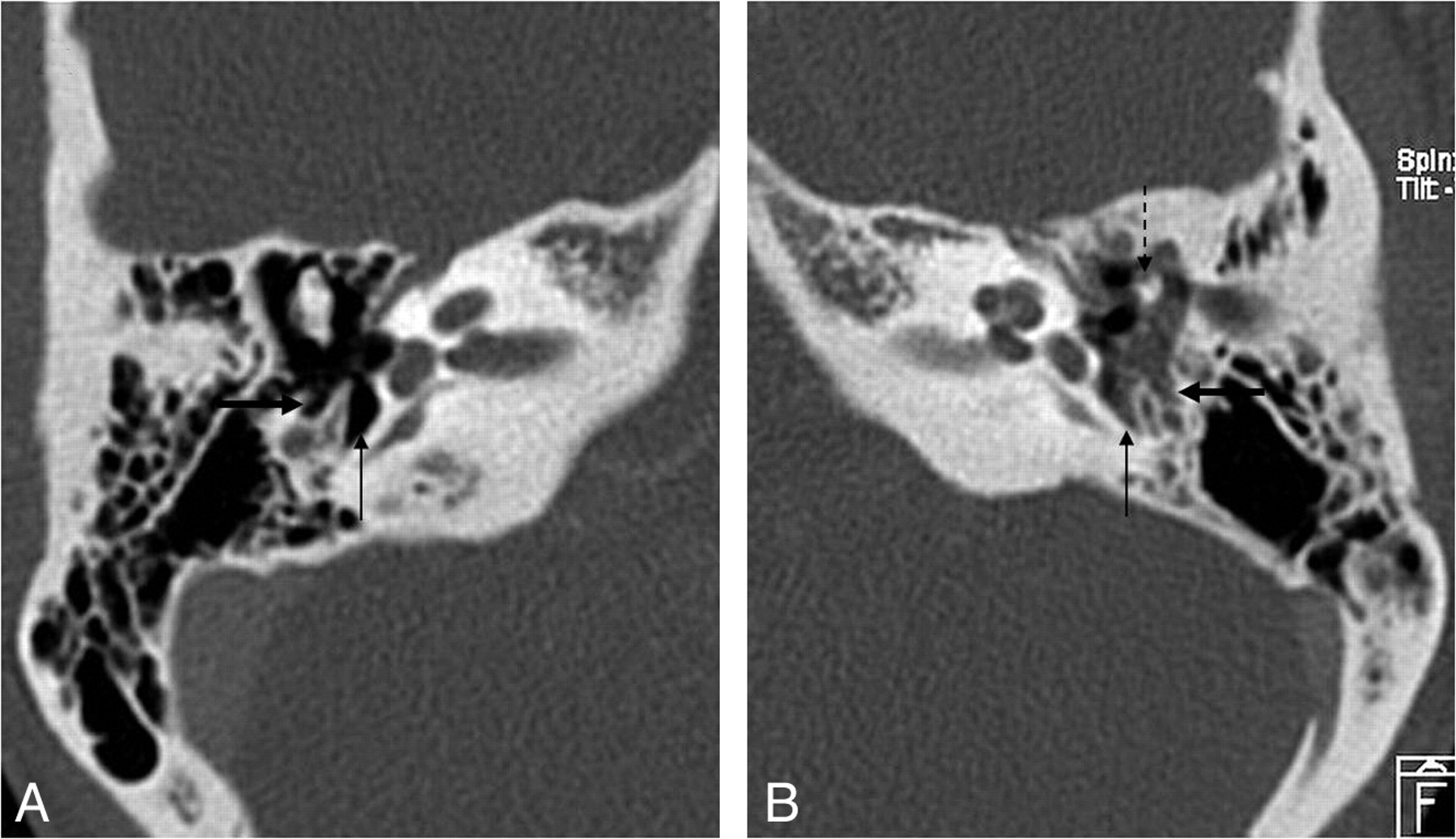
- Fig 4.
HRCT scan, coronal view. A, Pars flaccida cholesteatoma (arrow) filling the Prussak space. Notice the erosion of the scutum (dashed arrow). B, Prussak space is bordered by the pars flaccida of the TM (arrow) lateral, neck of the malleus (thick white arrow) medial, the short process of the malleus (white arrowhead) inferior, and lateral malleal ligament (dashed arrow) superior.
- Fig 5.
Pars tensa cholesteatoma. A, Coronal HRCT scan at the level of the cochlea shows the soft-tissue mass (black arrow) at the pars tensa of the retracted TM (white arrow). B, At the level of the vestibulum, the obliteration of the oval (dashed black arrow) and round (dashed white arrow) window niche is seen. Note the small bony fragments in the oval window niche, probably a sign of erosion of the stapes and the inferior wall of the tympanic segment of the facial canal.
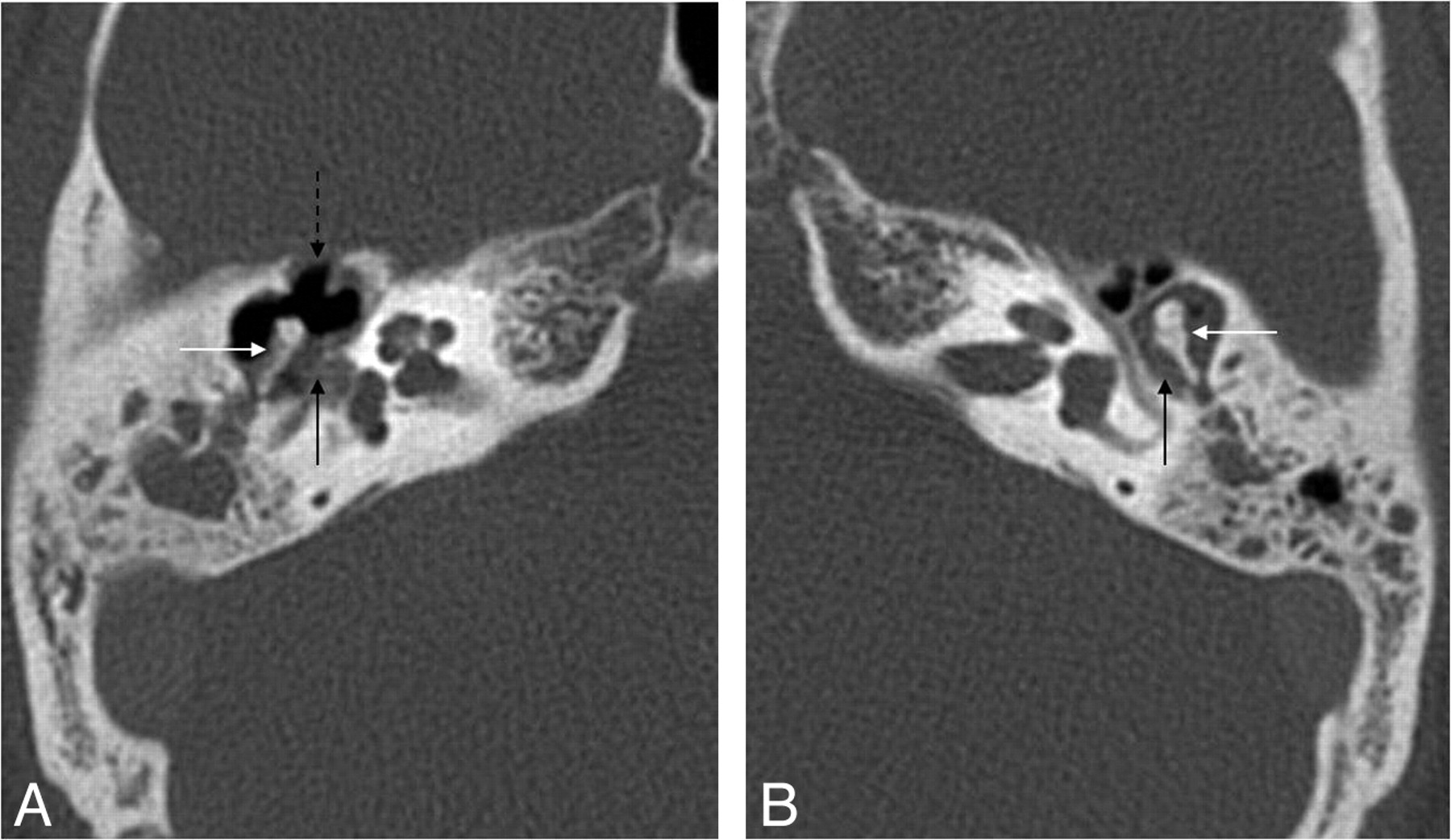
- Fig 6.
Pars tensa cholesteatoma. HRCT scans demonstrate the normal (air-filled) (A) and the obliterated (B) sinus tympani (arrow) and facial recess (thick arrow) due to a pars tensa (sinus) cholesteatoma. Note the ossicular erosion (dashed arrow) on B.
- Fig 7.
Mural cholesteatoma. Axial (A) and coronal (B) HRCT scans show the shell of the cholesteatoma in the epitympanum (black arrow) and the automastoidectomy cavity (thick arrow) without a history of surgery. Note the complete erosion of the ossicles, the fistula of the horizontal semicircular canal (dashed black arrow), and the wall erosion of the tympanic segment of the facial nerve canal (white arrow).
- Fig 8.
Intraoperative images show a typical pearly appearance of a cholesteatoma (arrow, A), in the aditus ad antrum, next to the posterior wall of the EAC (dashed arrow) and a more irregular cholesteatoma (thick arrow, B) accompanied by granulation tissue.
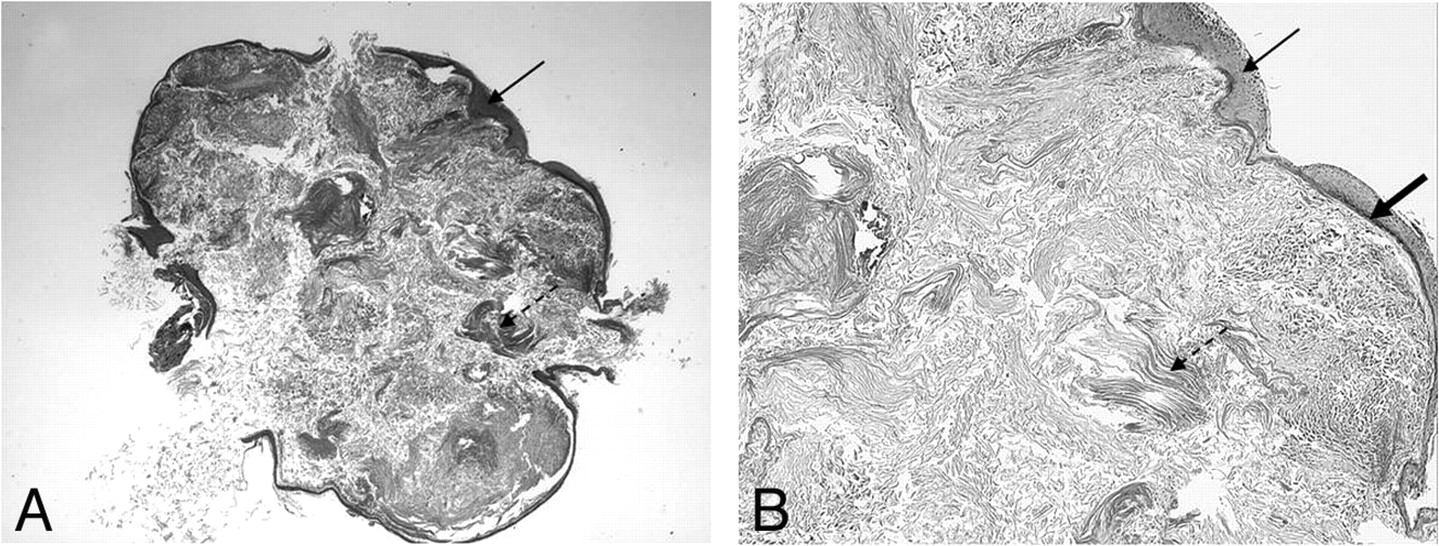
- Fig 9.
Histologic appearance of a cholesteatoma. Hematoxylin-eosin stain. Low-power view (original magnification ×25) (A) and high-power view (original magnification ×400) (B) demonstrate a cystic lesion covered by a strongly keratinizing stratified squamous epithelium (arrows). Within the cyst, there is abundant formation of desquamated keratin lamellas (dashed arrows). Note the prominent strongly hyperchromatic basal layer of the epidermis (thick arrow).
- Fig 10.
Patient with cholesteatoma on the right and chronic otitis media without cholesteatoma on the left. A, Axial HRCT scan shows the mass lesion (black arrow) in the tympanic cavity with ossicle erosion (white arrow) and erosion of the anterior wall of the epitympanum (dashed arrow). B, Axial HRCT scan demonstrates a mass lesion (black arrow) in the epitympanum, but no bony erosion (white arrow).
- Fig 11.
Recurrent cholesteatoma after surgery. A, Coronal HRCT scan shows the obliterated mastoidectomy cavity (white arrow). B, Coronal FIESTA image distinguishes the slightly hyperintense (to brain) cholesteatoma (thick white arrow on B, C, and D) from the strongly hyperintense granulation tissue (dashed arrow on B and C). C, Coronal contrast-enhanced MR image differentiates as well the nonenhancing cholesteatoma from the strongly enhancing granulation tissue. D, Coronal DWI with the intensive intralesional diffusion restriction supports the diagnosis. Note the susceptibility artifacts on the EPI-DWI (black arrow) on the right.











Tables
Initial Location Clinical History Status of TM (if middle ear) Congenital (2%)a Anywhere in the temporal bone No history Intact Acquired Middle ear Recurrent ear disease Primary (80%)a Apparently intact Secondary (18%)a Perforated -
a The percentage refers to the distribution of cholesteatomas in the middle ear.
-
- Table 2:
Classification of middle ear cholesteatomas based on location in relation to the TM
Initial Location Pathogenesis Pars flaccida (attic) Epitympanum, Congenital lateral to ossicles Primary acquired Secondary acquired Pars tensa (sinus) Mesotympanum, Congenital medial to ossicles Secondary acquired





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}