
Abstract
BACKGROUND AND PURPOSE: Limited data exists regarding the efficacy of percutaneous vertebroplasty for multiple synchronous and metachronous vertebral compression fractures. The purpose of this study was to evaluate whether the number of vertebral levels treated during percutaneous vertebroplasty procedures or the number of separate vertebroplasty procedures performed on a given patient affect clinical outcomes.
MATERIALS AND METHODS: We defined 3 patient populations in our retrospective study. Group 1 included 328 patients who underwent 1 single-level vertebroplasty procedure. Group 2 included 226 patients who underwent a single procedure in which 2 or more vertebral levels were treated. Group 3 included 101 patients who underwent 2 or more separate vertebroplasty procedures. Follow-up was performed between 1 week and 2 years postoperatively. Clinical outcomes were assessed through analysis of quantitative measurements of pre- and postoperative levels of pain with and without activity (0–10) as well as mobility improvement. The Kruskal-Wallis rank sum test was used to evaluate the differences among groups. Univariate and χ2 analyses were performed to show the proportion of underlying diseases in each group.
RESULTS: Mean pain improvement with/without activity at 2-year follow-up was 5.8/3, 4.9/3.7, and 5.4/3.1 in groups 1, 2, and 3, respectively; and mean mobility improvement in 2-year follow-up was 0.67, 0.63, and 0.65 for groups 1, 2, and 3, respectively.
CONCLUSIONS: There was no significant difference in pain relief and mobility improvement in patients treated for multiple synchronous or metachronous vertebral compression fractures in comparison with those treated for solitary isolated fractures.
Percutaneous vertebroplasty appears to be an effective minimally invasive procedure used to treat painful vertebral compression fractures. The procedure, originally used in patients with vertebral malignancies and hemangiomas, has been expanded in its therapeutic range to include osteoporotic fractures refractory to medical management. Many patients with vertebroplasty return after their initial procedure with new fractures.1-8 Treatment in these returning patients commonly involves cement injection into multiple vertebral levels in multiple separate procedures to address the synchronous and metachronous fractures inherent in osteoporotic spines.
The purpose of this study was to evaluate whether the number of vertebral levels treated during percutaneous vertebroplasty procedures or the number of separate procedures performed on each patient affected clinical outcomes. By doing so, we attempted to correlate the severity and extent of disease with therapeutic benefit of vertebroplasty.
Materials and Methods
Patient Selection
We conducted a retrospective review of consecutive percutaneous vertebroplasty procedures performed at our institution between February 1999 and February 2007 to define 3 patient populations. We have previously published global outcomes in this same cohort of patients as well as many subgroup analyses.6,9-23 We have never previously analyzed this same cohort of patients regarding the impact of the number of treated levels or treatment sessions on outcome. We defined these groups as:
Group 1: Patients who underwent 1 single-level vertebroplasty procedure.
Group 2: Patients who underwent a single procedure in which 2 or more vertebral levels were treated.
Group 3: Patients who underwent 2 or more separate vertebroplasty procedures.
Preprocedural Work-Up
Screening and preprocedural evaluation have been described in detail by Jensen et al24 and Maynard et al.25 Briefly, patients with subacute pain with corresponding fractures were considered appropriate candidates. Patients with fractures of uncertain age or with atypical pain patterns were treated if MR imaging or bone scanning demonstrated edema or increased activity, respectively.25
Procedural Technique and Materials
The vertebroplasty technique has been described in detail previously. Briefly, a unilateral or bilateral transpedicular approach is used to place the tip of an 11-gauge needle or needles in the ventral aspect of the vertebra. Using continuous lateral fluoroscopy, we inject barium-opacified polymethylmethacrylate until extraosseous extravasation or filling of the posterior aspect of the vertebra is attained.
Assessment
Clinical Outcomes.
Patients were assessed before the procedure regarding the degree of pain and limitations of mobility. Patients in group 3 were followed up separately for each procedure on postoperative day 1 and at 1 week, 1 month, 6 months, 1 year, and 2 years postoperatively. Procedural notes were also reviewed to evaluate procedural complications.
Pain.
Pain was assessed by using an ordinal scale, in which the patients were asked to rate their pain on a scale of 0–10, with 0 representing no pain and 10 representing the “most pain ever experienced.” Questions were posed as pain at rest and pain with activity. A Roland-Morris Disability Questionnaire score was obtained by experienced vertebroplasty nurses and neuroradiologists.
Mobility.
Mobility was assessed before the procedure by using a 4-point scale as follows: walking >1 block, walking <1 block, restricted (with the help of walker or walking around the home but not outside), and bedridden. We tracked the patients in all 3 groups as to whether there was improvement, no change, or decreased mobility after the procedure. We assigned the following numbers to calculate the quantity of mobility changes: improvement = 1, no change = 0, and decreased = −1.
Underlying Causes
We categorized the underlying causes for all vertebral fractures into 3 groups: trauma; neoplasm, to include multiple myeloma; and osteoporosis. Baseline pain and disability as well as severity throughout follow-up were compared among groups.
Statistical Analysis
Clinical Outcome.
The Kruskal-Wallis rank sum test was used to evaluate a statistically significant difference among the 3 groups in pre- and postoperative levels of pain and mobility. Because the P value was calculated for each follow-up time point (5 times), we performed a Bonferroni adjustment for P value, and <.01 was considered significant. When a P value < .01 was obtained, we used a 2-tailed Wilcoxon rank sum test to evaluate statistically significant differences between individual groups. Such an approach was performed on the pre- and postoperative levels of pain and mobility for the 3 groups in an attempt to preserve the operant form of the data. A χ2 test was performed to compare the proportion of underlying processes, including trauma, osteoporosis, and neoplasm, including multiple myeloma, among groups. Univariate analysis showed the differences in the severity of pain caused by underlying diseases in each group.
Results
Patient Population
We identified 655 patients (67% female) treated at 1195 vertebral levels during 791 vertebroplasty procedures. Demographic details of the groups are shown in Table 1.
Patient demographics
Preoperative Evaluations
Proportions of underlying processes in each group are shown in Table 2. Among patients with cancer, baseline pain was higher than among those without cancer in group 1. Among patients with osteoporosis, preoperative pain was less with activity in group 2 than among those patients without osteoporosis.
Proportion (%) of underlying disease in groups
Clinical Outcome
Table 3 shows the available number of patients at the various follow-up periods.
Number of available patients or (procedures) in each follow-up time point
Pain.
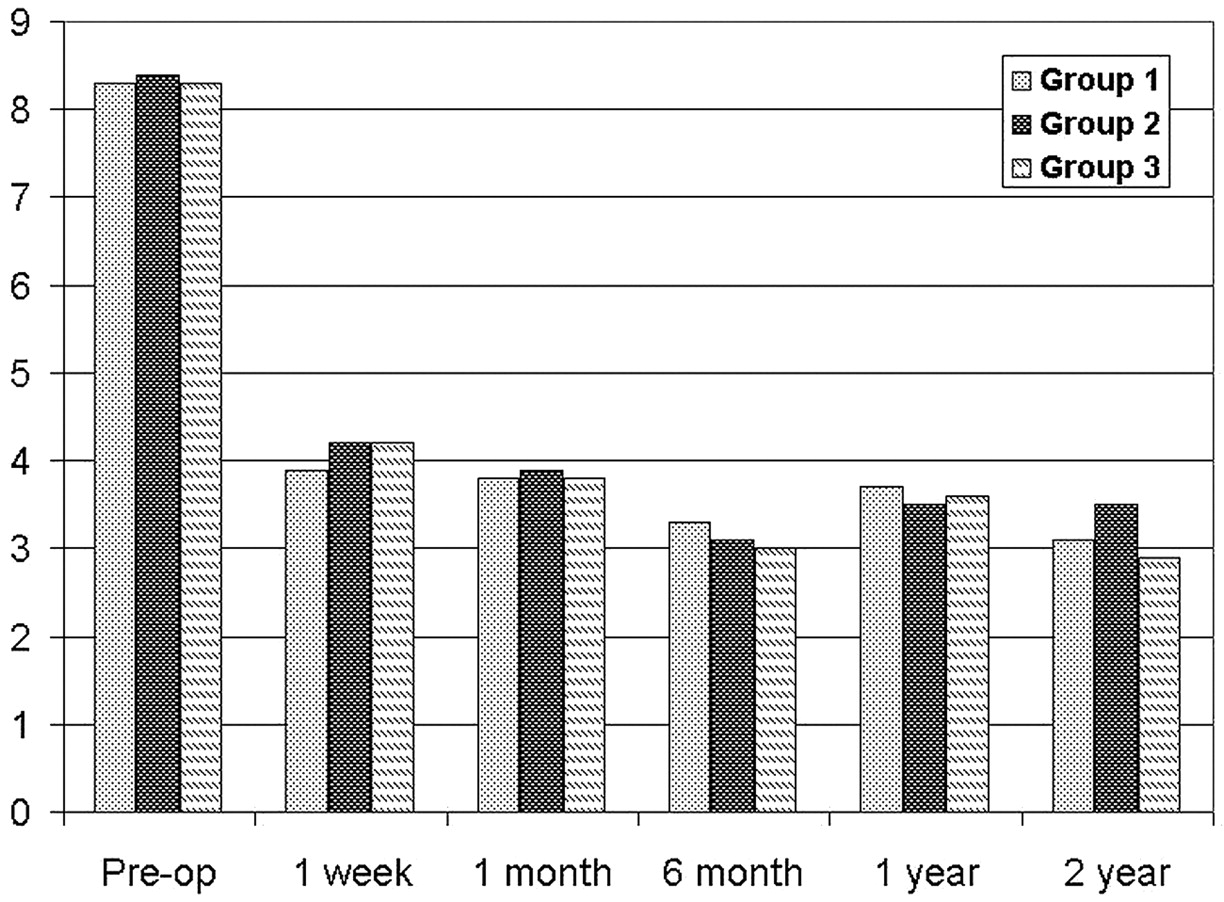
Figures 1 and 2 show the severity of pain with time, both at rest and with activity, respectively. Because we have published in previous articles for the entire cohort,6,20 we noted significant improvement in pain at all time points compared with preprocedural pain severity both at rest and with activity. There were no significant differences in pain severity among groups at any time point either at rest or with activity. At 6-month follow-up, there were no significant differences in the severity of pain as a function of underlying disease processes, including trauma, osteoporosis, or cancer.

Graph shows changes of pain scores (0–10) at rest. Pre-op indicates preoperative.

Graph shows changes of pain scores (0–10) with activity. Pre-op indicates preoperative.
Back-Pain-Specific Function.
Scores on the Roland Morris Disability Scale are shown in Fig 3. There were no significant differences among groups at any time point.

Graph shows Roland-Morris Disability pain scores. Pre-op indicates preoperative.
Mobility.
Figure 4 shows the improvement of mobility in all groups. Scoring assignments are the following: improvement = 1, no change = 0, and decrease = −1. There were no differences noted.

Graph shows mobility improvement during the time in different groups.
Complications
Immediate and long-term (in 2-year follow-up) complications are shown in Table 4. There were no significant differences between the 3 groups for incident fractures (P = .06).
Percentage of complications in the 3 groups
Group 3 Specifications.
Patients in group 3 underwent a median of 2 procedures (range, 2–7) with a median delay of 88 days (range, 1–2131 days) from the previous procedure. The mean time interval between procedures in group 3 was 257 days.
Power of the Study.
Our data had 80% power to detect an effect size of 0.014 for 1-month pain at rest and with activity and 0.014 for 1-month Roland-Morris Disability score.
Discussion
Vertebroplasty was initially applied in patients with well-documented single-level osteoporotic compression fractures.24 With increasing dissemination of the procedure, many groups now routinely treat multiple vertebral levels in a single session. Furthermore, many patients return for additional treatments at later time points for new-onset fractures. The aim of this study was to evaluate whether more extensive procedures, including treatment of multiple synchronous and metachronous fractures, were as effective as single-level procedures in relieving pain and improving mobility.
The results of this study indicate that outstanding pain relief is consistently achieved with percutaneous vertebroplasty, regardless of either the number of fractures treated in 1 procedure or the number of treatment sessions. Specifically, mean decrease in pain and improvement in back-pain-specific morbidity were similar across all groups described in this report. These data support the routine use of multilevel vertebroplasty as well as the routine application of vertebroplasty in patients returning with new-onset fractures.
Current medical literature offers numerous case series and retrospective studies that have reported overwhelmingly positive clinical responses to percutaneous vertebroplasty.1,2,6,26-30 The bulk of this research has centered around evaluations of the safety and efficacy of the procedure. Some series report clinical benefit in as many as 97% of patients,31 with the procedure producing exceedingly few clinically apparent complications.2,26,30,32-34 Other case series have focused on patient-selection criteria in an attempt to aid in maximizing the potential of vertebroplasty.35-38 To our knowledge, however, no literature exists that correlates clinical outcomes with extent or severity of disease. Specifically, none of these previous series has evaluated whether the efficacy of vertebroplasty is affected by the number of vertebrae treated in a given session. Similarly, previous studies have not evaluated whether patients returning for additional treatment sessions for new fractures derive the same benefit as those needing treatment only once.
Although this study represents an objective evaluation of the efficacy of vertebroplasty over a diverse patient population, it has several limitations. Its retrospective nature lacks the randomization of a prospective clinical trial. Also, as mentioned previously, selection bias may have affected the outcome of patients returning for multiple procedures.
The results of this study suggest that percutaneous vertebroplasty represents an effective treatment for vertebral compression fractures, regardless of the severity or extent of disease. Future studies would aid in furthering our understanding of the diversity of the patient population currently receiving benefit from the procedure. Prospective randomized trials may assist in clarifying the uncertainties that continue to surround the use of this technique with regard to prognostication of clinical outcomes. Similarly, long-term studies may aid in delineating the clinical benefit bestowed on these patients.
Conclusions
There were no significant differences in pain relief and mobility improvement in patients treated for multiple synchronous or metachronous vertebral compression fractures compared with those treated for solitary isolated fractures.
References
- Received July 16, 2008.
- Accepted after revision August 15, 2008.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}