
Abstract
BACKGROUND AND PURPOSE: A lingual abscess is difficult to diagnose in the absence of physical signs. MR imaging may provide an excellent and invaluable adjunct to clinical examination, but the literature is incomplete in defining the various MR imaging findings of abscess. The objective of this study was to determine the MR imaging features of tongue abscesses.
METHODS: Seven surgically proved tongue abscesses were evaluated with MR imaging. Four patients underwent MR imaging because of suspected tumor, and 3 patients, to show the extent and precise anatomic location of the lesion. Lesions were assessed with regard to the location, size, signal-intensity characteristics, and pattern of contrast enhancement.
RESULTS: Five lesions were located in the anterior tongue and 2, in the posterior tongue. The central parts of 4 anterior tongue abscesses were hypointense, surrounded by a hyperintense wall on T1-weighted precontrast images. On postcontrast images, marked wall enhancement was detected. On T2-weighted images, a markedly hyperintense central part surrounded by a hypointense rim was seen. In 2 of these patients, there was a hypointense halo surrounding the wall (target sign). In 3 patients, a perilesional hyperintense area that enhanced diffusely after contrast administration was detected on T2-weighted images. The smallest lesion located in the anterior tongue was hypointense on T1-weighted images and enhanced diffusely on postcontrast images. On T2-weighted images, a markedly hyperintense central part surrounded by a mildly hyperintense peripheral part was depicted. Posterior tongue lesions appeared as polypoid ill-defined masses and were hypointense on T1-weighted images and heterogeneously hyperintense on T2-weighted images. On postcontrast images, the lesion in 1 patient showed diffuse and heterogeneous contrast enhancement, whereas the lesion in another patient enhanced peripherally. The lesions were totally excised in 4 patients and drained with surgical incisions in 3 patients. No recurrence was detected on follow-up.
CONCLUSION: An abscess typically presents as a cystic lesion surrounded by an enhancing capsule formation, but lesions may also present as solid masses that enhance diffusely or peripherally.
Abscess of the tongue is a rare potentially life-threatening clinical entity. During the past 30 years, 50 cases of tongue abscess have been reported in the English literature, consisting mostly of single case reports.1 Accurate diagnosis of these treatable lesions has important prognostic and therapeutic implications. When diagnosed, these lesions are opened and drained.2 In the English literature, there are a few single case reports of MR imaging findings of tongue abscess. The purpose of this retrospective study was to determine the MR imaging findings of the 7 proved tongue abscesses encountered during the past 8 years.
Methods
Seven patients (4 men and 3 women; age range, 29–64 years; mean age, 46.4 years) with proved tongue abscess who underwent MR imaging examinations between September 1996 and March 2004 were included in the study. The presenting symptoms were pain and swelling in 2 patients, painful masses in 3 patients, respiratory distress in 1 patient, and dysphagia in 1 patient. Duration of symptoms was 2 days in the patient with respiratory distress and 3 months in the patient with dysphagia. On physical examination, in 2 patients, a sharply bordered and superficially protruding painful mass lesion was observed in the right part of the tongue. The overlying mucosa was intact and of normal color (cases 1 and 5). In 3 patients, a massive fluctulent asymmetric swelling of the tongue with boardlike indurations was observed (cases 2–4). In 2 patients, a mass lesion with smooth contours was detected in the midline, filling the vallecula. The overlying mucosa of the masses was intact and of normal color.
Fever (body temperature, >37.8°C) and leukocytosis (leukocyte count, >10 000/mm3) were present in only 2 patients. Three patients had poor oral hygiene and multiple caries. In 4 patients, oral hygiene was normal. Patient 1, previously described in a case report,3 had a history of alcoholism for more than 20 years. The remainder of the findings on physical examination and complete blood count were normal. None of the patients had trauma, bite wounds to the tongue, surgery, or tongue-piercing history. Diabetes or immunologic deficiency was not present. Two patients (cases 1 and 6) had used antibiotics before presentation, and 5 had not.
In 4 patients, the mass with a spindle-shaped overlying normal tongue mucosa and a small amount of surrounding healthy tissue was totally excised, with the patient under general anesthesia. Histopathologic examination revealed only chronic inflammatory changes. In 3 patients, surgical incision and drainage were performed using local anesthetic. All of the lesions were found to be in the tongue musculature.
The pus culture did not reveal any bacteria in 4 patients. In 2 patients, anaerobic bacteria, and in 1 patient, Streptococcus viridans grew on culture. All patients responded remarkably well and did not have any recurrences.
MR Imaging
From 1996 to 2004, all patients underwent MR imaging examinations with a 1.5T scanner (Philips Gyroscan ACS-NT and Philips Intera, Philips, Best, the Netherlands). Four patients underwent MR imaging because of suspected tumor, and 3 patients, to show the extent and precise anatomic location of the lesion. A head coil was used for the examination, and T1-weighted (TR/TE, 400–700/10–30) and T2-weighted (TR/TE, 3000–5000/70–110) fast spin-echo images were obtained in 3 orthogonal planes. Typical MR parameters were as follows: field of view, 18 cm for the axial plane and 20 cm for the sagittal and coronal planes; number of excitations, 2; matrix size, 256 × 256; section thickness, 5 mm; intersection gap, 1 mm; and echo-train length, 8–16. T1-weighted MR images were obtained before and after intravenous administration of gadopentate dimeglumine (Magnevist, Schering, Berlin, Germany) (0.1 mmol per kilogram of body weight).
The following features were assessed on the MR images: diameter and location of the lesion, signal intensity on T1- and T2-weighted images, the appearance of the abscess wall, pattern of gadolinium enhancement (rim enhancement around a central nonenhancing area or diffuse enhancement), the involvement of the opposite side of the tongue, and perilesional edema (surrounding areas of increased signal intensity on T2-weighted images). The signal intensity of the lesions was considered hypointense, isointense, or hyperintense relative to the signal intensity of the normal tongue in the same patient on T1- and T2-weighted images.
Results
Anterior Tongue Abscess
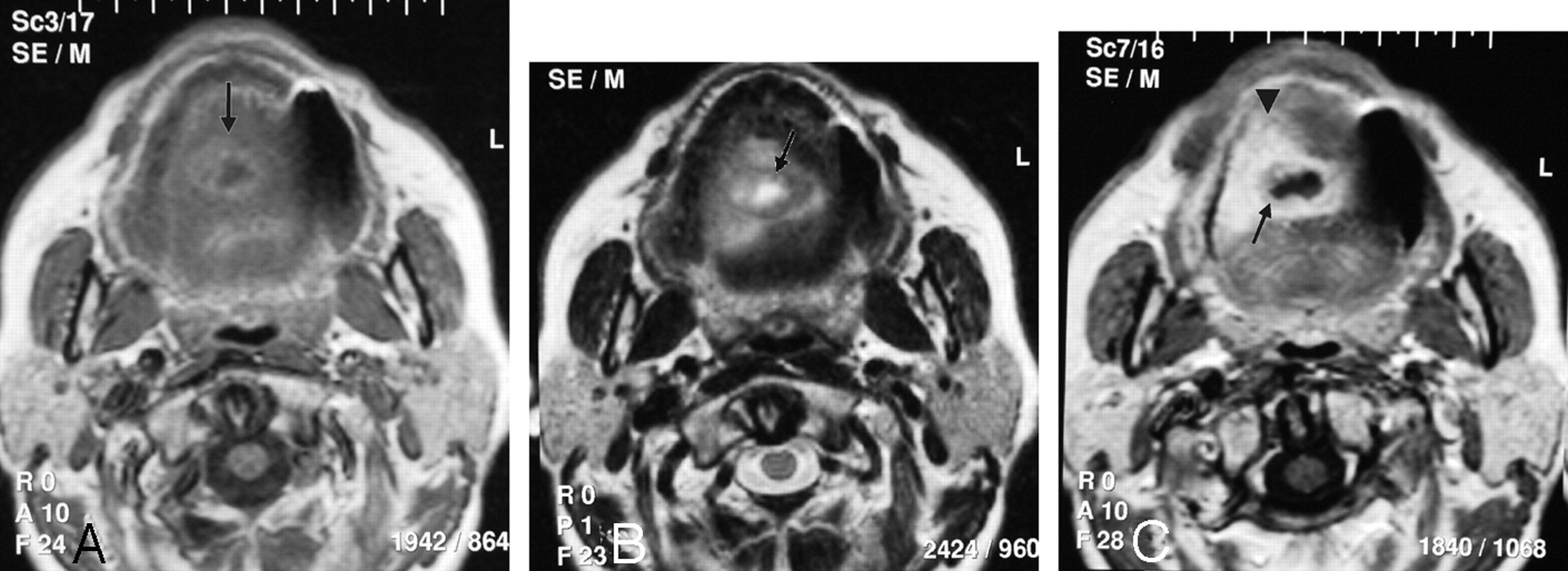
Five lesions were located in the anterior tongue. Three of the anterior tongue abscesses were located on the right and 2 on the left side of the tongue. The size of the abscess ranged from 1.2 to 3 cm (mean, 2.1 cm). On T1-weighted precontrast images, the central parts of 4 anterior tongue abscesses were hypointense, surrounded by a hyperintense wall, which ranged from 2 to 7 mm (Fig 1A). On T2-weighted images, the central part of these lesions was markedly hyperintense, surrounded by a hypointense rimlike wall structure (Fig 1B). In 3 of these 4 patients, there was a perilesional hyperintense area on T2-weighted images, which diffusely enhanced after contrast administration, indicating perilesional cellulitis (Fig 1C). Two lesions extended to the other half of the tongue by crossing the lingual septum. On postcontrast images, marked wall enhancement was detected in all the 4 patients. Two of these lesions had a hypointense halo surrounding the wall (target sign) (Fig 1C).

A 51-year-old woman with abscess in the right middle third of the tongue.
A, An axial T1-weighted unenhanced MR image shows a centrally hypointense lesion with a high-intensity peripheral rim.
B, An axial T2-weighted MR image reveals a lesion that is very hyperintense, with a low-intensity rim (arrow) and hyperintense perilesional edema (arrowhead).
C, A contrast-enhanced axial T1-weighted MR image depicts rim enhancement in the lesion, with enhancing perilesional tissue (arrowhead). A hypointense peripheral halo surrounding the wall is seen (arrow).
The smallest lesion located in the anterior tongue was hypointense on T1-weighted images and enhanced diffusely on postcontrast images. On T2-weighted images, the central part was markedly hyperintense, whereas the periphery of the lesion was mildly hyperintense. A surrounding wall was not present.
Posterior Tongue Abscess
Two lesions were located in the posterior tongue. They were seen as polypoid ill-defined masses filling the vallecula. The lesions were hypointense on T1-weighted images and heterogeneously hyperintense on T2-weighted images. On postcontrast images, 1 lesion enhanced peripherally (Fig 2). The other lesion showed diffuse and heterogeneous contrast enhancement.

A 55-year-old man with an inflammatory mass lesion in the posterior third of the tongue.
A, An axial T1-weighted unenhanced MR image shows a hypointense nodular mass lesion in the vallecula (arrow).
B, A contrast-enhanced axial T1-weighted MR image reveals marked enhancement with a nonenhancing central necrotic area (arrow).
C, An axial T2-weighted MR image reveals a lobulated hyperintense mass lesion with fine internal septations (arrowhead).
The MR imaging features of all the lesions are summarized in the Table.
MR imaging findings
Discussion
Tongue abscess is a very rare condition. Despite exposure to many potential pathogens, the tongue is comparatively immune to infection. Some of the reasons for this immunity include the constant mobility of the tongue, which helps the saliva produce a perpetual cleansing effect; its thick covering of keratinized mucosa, which is not easily penetrated by micro-organisms; the muscle tissue, which constitutes the chief bulk of its parenchyma, with its rich vascular supply; its rich lymphatic drainage; and the immunologic properties of saliva.3–5 When the host defense mechanisms are impaired, tongue abscess is more likely to occur. Breached surface barriers, foreign bodies, and immunodeficiency status predispose to tongue infections. The tongue mucosa may be breached pharmacologically by chemotherapeutic drugs or mechanically by trauma. After the first line of defense is breached and the host immune system is compromised, the tongue infection can be severe and recalcitrant.1 Foreign bodies also predispose to inflammatory response of the tongue and abscess formation, even in healthy individuals. The recent literature reports reveal association between tongue abscess and body piercing.6,7 The incidence of tongue abscess does not vary according to socioeconomic status, age, or sex. Quite often no specific cause can be identified.8
The etiology of a tongue abscess may differ depending on its location. The anterior two thirds of the tongue is known as the “oral tongue” and is the freely moving part that lies anterior to the circumvallate papillae. The posterior of the circumvallate papillae is the “tongue base” and is regarded as a part of the oropharynx.9 Most tongue abscesses are unilateral and located in the anterior two thirds of the tongue. In the posterior third of the tongue, abscesses most often originate as lingual tonsillar lesions, infected thyroglossal duct cysts, or extensions of apical infections from the first or second molars.10 Streptococcus and Staphylococcus species and anaerobes grow on culture. Mixed cultures are often seen. If the patient was previously treated with antibiotics, then no growth may be seen.8 Sands et al11 reported a case and reviewed the literature, identifying 12 cases. In this report, no specific etiologic agent could be identified in 10 of the 12 patients. In the present study, in 2 cases, anaerobes and, in 1 case, Streptococcus viridans grew on culture. In 4 cases, no microbiologic agent could be identified.
The symptoms of acute tongue abscess are swelling or a lump in the deep tissues of the tongue, pain radiating toward the ears, throbbing local pain, fever, difficulty in swallowing, voluntary fixation of the tongue because of pain, and, later, difficulty in breathing.1,3,12 Although with the help of these findings, the diagnosis of glossal abscess can be reached clinically, sometimes no specific sign or symptom is present, making diagnosis difficult. In our study, in 3 patients, abscess formation was clinically apparent. In the remaining 4 patients, there was no clinical or laboratory finding indicating abscess formation.
Differential diagnosis of acute tongue swelling includes a number of diseases such as tumor, cyst, infarction, edema, infection, hemorrhage, and metabolic (amyloidosis, hypothyroidism, acromegaly, B12 vitamin deficiency, and iron deficiency) and developmental processes.1 Several imaging techniques, including sonography, CT, and MR imaging, can be used to evaluate the tongue swellings.1,3,5,13–15 Sonographic depiction of a lingual abscess as a hypoechoic lesion surrounded by a hyperechoic ring has been reported,14 but sonography is not always feasible because when the tongue is swollen, the patient may experience discomfort or acute pain if it is pressed. Air interposition may reduce the visibility of the anterior portion of the tongue and oropharynx. Operator dependence is another drawback of sonography, and anatomic landmarks are not precise.3,5,14
The usefulness of CT in tongue abscess has been reported.8,13 Dental amalgam artifacts and beam-hardening artifacts are the main obstacles of CT, but with advanced CT scanners, it is possible to reduce these artifacts. With multisection CT, one can get excellent reformatted images. Although beam-hardening artifacts and amalgam artifacts are not seen on MR imaging, restorations, dental appliances, and motion may cause severe artifacts. MR imaging is also insensitive in the differentiation of malignant lesions and abscesses, but it clearly reveals the anatomy of the oral cavity with excellent soft-tissue detail and multiplanar capability.3–15 These features make MR imaging suitable for scanning the tongue and the floor of mouth, but the literature is incomplete in describing the various MR imaging features of tongue abscess.
Radiologic features of inflammatory processes vary: Some appear solid, some cystic. Mendez et al16 reported that sharp margins, perilesional edema, rim enhancement, and very high signal intensity on T2-weighted images suggest the diagnosis of a large hepatic abscess. Muñoz et al5 reported 1 lingual abscess located in the posterior tongue. The reported case had heterogeneous signal intensity on T1-weighted images and hyperintense signal intensity on T2-weighted images. After intravenous contrast injection, peripheral thick rim enhancement with edema and swelling was seen. In our study, the central parts of 4 lesions were hypointense on T1-weighted and hyperintense on T2-weighted images. This central part was surrounded by a wall that was hyperintense on T1-weighted and hypointense on T2-weighted images and enhanced diffusely after contrast injection. Our findings were in concordance with the findings reported by Muñoz et al, and the diagnosis was established. In 2 patients, a hypointense halo surrounding the wall (target sign) on postcontrast T1-weighted images and, in 3 patients, a perilesional hyperintense area on T2-weighted images that diffusely enhanced after contrast administration, indicating perilesional cellulitis, were also present. We assume that these findings are also important in establishing abscess diagnosis.
The hypointense rim seen in brain abscess is attributed to collagen, hemorrhage, or paramagnetic free radicals within phagocytosing macrophages. In the latter hypothesis, localized shortening of T1 and T2 relaxation times accounts for the signal intensity properties. Free radicals promote the formation of methemoglobin; therefore, hemorrhage and free radicals may play a role in the generation of the described signal-intensity characteristics.17 Also the “dark rim” sign seen in hepatic abscess is attributed to phagocytosing macrophages, which are distributed at the periphery of the abscess.18 These factors may also be responsible for the hypointense rim on T2-weighted images seen in our patients.
The smallest lesion located in the anterior tongue and 2 lesions located in the posterior tongue were diffusely hypointense on T1-weighted images. On T2-weighted images, the central part of the lesion located in the anterior tongue was hyperintense, surrounded by a peripheral mildly hyperintense area. On postcontrast images, diffuse enhancement was detected. Two lesions located in the posterior tongue were heterogeneously hyperintense on T2-weighted images. Gadolinium injection revealed a central nonenhancing portion in 1 of the lesions and heterogeneous marked enhancement in the images of 1 patient.
The distinction of lingual abscess from lingual cellulitis often cannot be made clinically. This distinction is important because abscesses will not resolve without proper incision and drainage, and incision into a cellulitic tongue accomplishes nothing.8 Therefore, imaging determines the correct line of treatment. MR imaging can distinguish these 2 clinical entities and thereby direct the treatment. The presence of a surrounding wall, perilesional edema on T2-weighted and postcontrast images, a halo on postcontrast images, and a central necrotic area are highly suggestive of abscess. When these features are not present, it is difficult to distinguish cellulitis from abscess.
Conclusion
Typically abscess presents as a T1 hypointense–T2 hyperintense lesion surrounded by a T1 hyperintense–T2 hypointense rim that enhances diffusely after contrast injection. The target sign and edema pattern are ancillary findings that suggest the diagnosis of abscess, but an abscess may also present as a masslike lesion that enhances diffusely or peripherally.
References
- Received May 16, 2005.
- Accepted after revision October 13, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.