
Article Figures & Data
Figures
- Fig 1.
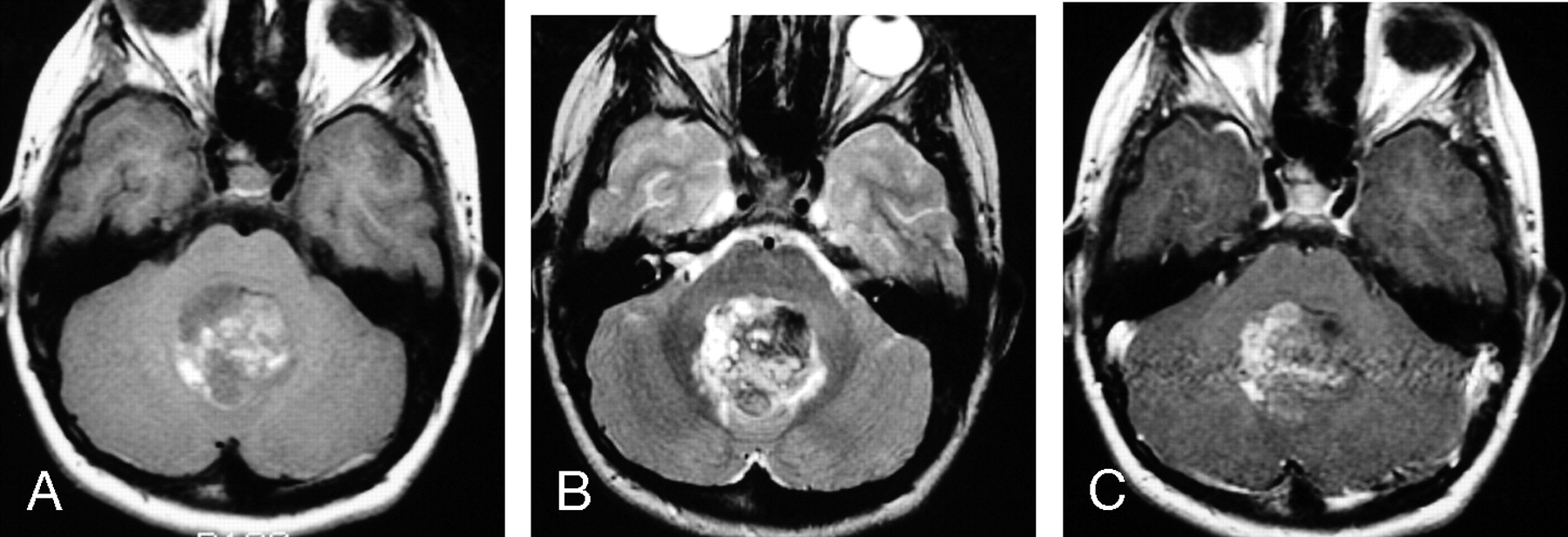
MR images of a 2-year-old girl with a germ-line mutation of the hSNF5/INI1 gene and AT/RT in the vermis extending into the fourth ventricle.
A, Sagittal (TR/TE, 520/10) MR image shows the tumor to have intermediate and low signal intensity. The tumor invades the dorsal brain stem.
B, Axial (TR/TE, 5700/90) MR image shows the tumor to have heterogeneous intermediate-to-slightly-high signal intensity that is slightly hyperintense relative to gray matter, as well as zones of high signal intensity representing cystic/necrotic regions. Abnormal high signal intensity is also seen in the dorsal pons and left middle cerebellar peduncle, consistent with tumor invasion.
C, Axial (TR/TE, 680/22) MR image shows the tumor to have solid-enhancing and nonenhancing cystic/necrotic components. Irregular enhancing margins of the lesion are seen at the dorsal pons and left middle cerebellar peduncle, consistent with tumor invasion. This patient died 1.6 years after diagnosis from locally recurrent and disseminated tumor.
D, Axial CT image shows the solid portion of the AT/RT to have attenuation slightly higher than that of gray matter. Low-attenuation cystic/necrotic zones and several tiny calcifications are also present.
- Fig 2.
MR images of a 10-year-old boy with AT/RT in the vermis, extending into the fourth ventricle.
A, Axial (TR/TE, 600/11) MR image shows the tumor to have mixed intermediate signal intensity as well as irregular zones of high signal intensity secondary to hemorrhage (methemoglobin).
B, Axial (TR/TE, 3500/108) MR image shows the tumor to have heterogeneous mixed low, intermediate, and high signal intensity.
C, Axial (TR/TE, 500/29) MR image shows contrast enhancement in less than two thirds of the AT/RT. This patient is alive without evidence of disease 9 years after surgery/initial diagnosis.
- Fig 3.
MR images of a 1.3-year-old boy with AT/RT in the right cerebral peduncle.
A, Axial (TR/TE, 600/10) MR image shows the tumor to have intermediate signal intensity.
B, Axial (TR/TE, 4000/105) MR image shows the tumor to have heterogeneous intermediate-to-slightly-high signal intensity, which includes zones that are isointense or slightly hyperintense to gray matter.
C, Axial (TR/TE, 700/22) fat-suppressed MR image shows prominent homogeneous contrast enhancement of the primary lesion as well as abnormal subarachnoid enhancement in the interpeduncular cistern and along the sulci adjacent to frontal lobes (arrows), representing disseminated leptomeningeal tumor. This patient died 4 months after diagnosis.
- Fig 4.
MR images of 3.4-year-old boy with a hemorrhagic AT/RT in the frontal lobe.
A, Sagittal (TR/TE, 520/10) MR image shows a hemorrhagic lesion in the inferior left frontal lobe.
B, Sagittal (TR/TE, 600/22) MR image shows edge enhancement of the lesion.
C and D, Sagittal (C) (TR/TE, 520/10) and axial (D) (TR/TE, 520/10) MR images obtained 7 months after A, -B show marked interval enlargement of the lesion, which has heterogeneous mixed low, intermediate, and high signal intensity involving the inferior portions of both frontal lobes.
E, Axial (TR/TE, 5700/90) MR image shows the tumor to have mixed low, intermediate, and high signal intensity, with evidence of edema in the surrounding brain tissue.
F, Axial (TR/TE, 600/22) MR image shows prominent heterogeneous contrast enhancement of the tumor with irregular lobulated margins. This patient underwent partial resection of the AT/RT, subsequently had disseminated leptomeningeal tumor, and died 3.3 years after surgery/initial diagnosis.
G, Axial CT image shows the lesion to have intermediate attenuation with multiple calcifications and zones of low attenuation.
- Fig 5.
MR images of a 4-year-old girl with a constitutional ring 22 chromosome and AT/RT involving the septum pellucidum, with extension into the lateral ventricles.
A, Axial (TR/TE, 450/18) MR image shows the tumor to have intermediate signal intensity with several small zones of low signal intensity.
B, Axial (TR/TE, 4000/105) MR image shows the tumor to have heterogeneous predominantly intermediate-to-slightly-high signal intensity that is isointense to gray matter, as well as small zones of high and low signal intensity.
C, Axial (TR/TE, 450/31) MR image shows irregular heterogeneous contrast enhancement of less than two thirds of the primary AT/RT. This patient had subtotal resection of the tumor and subsequently had locally recurrent disease and disseminated leptomeningeal tumor. She died 14 months after surgery/initial diagnosis.
- Fig 6.
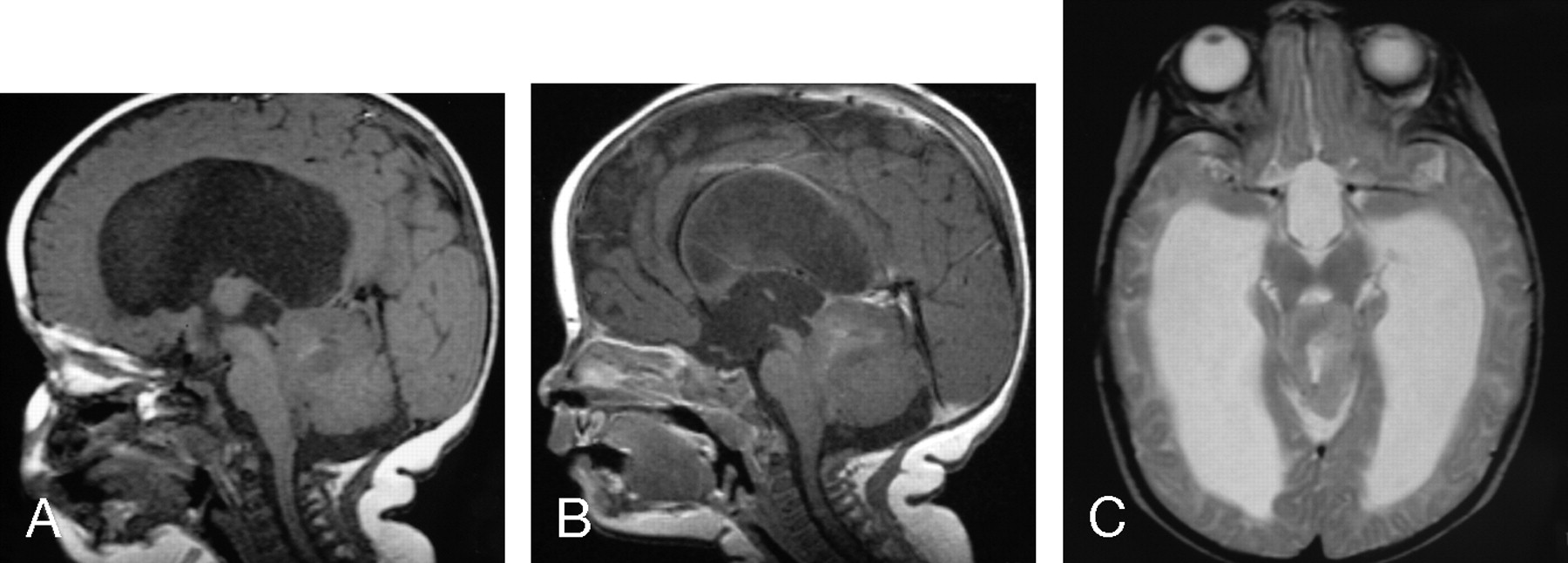
MR images of a 4-month-old female infant with a germ-line mutation of the hSNF5/INI1 gene with synchronous AT/RT, showing contiguous involvement of the pineal gland, dorsal midbrain, and upper cerebellum and a malignant rhabdoid tumor involving the left kidney.
A, Sagittal (TR/TE, 570/14) MR image shows the tumor to have predominantly intermediate signal intensity with several small zones of high signal intensity.
B, Sagittal (TR/TE, 750/22) MR image shows only minimal contrast enhancement in less than one third of the tumor.
C, Axial (TR/TE, 3710/105) MR image shows the tumor to have intermediate-to-slightly-high signal intensity that is isointense to gray matter, as well as a small zone of high signal intensity.
- Fig 7.
MR images of a 10-month-old female infant with an extra-axial AT/RT in the right cerebellopontine angle cistern, extending into the right internal auditory canal (arrows).
A, Axial (TR/TE, 550/14) MR image shows the tumor to have intermediate signal intensity with a zone of low signal intensity medially.
B, Axial (TR/TE, 600/22) MR image shows prominent enhancement of the solid portion of the lesion. This patient had subtotal resection followed by chemotherapy and died 1 month after surgery from sepsis related to immunosuppression from chemotherapy.
- Fig 8.
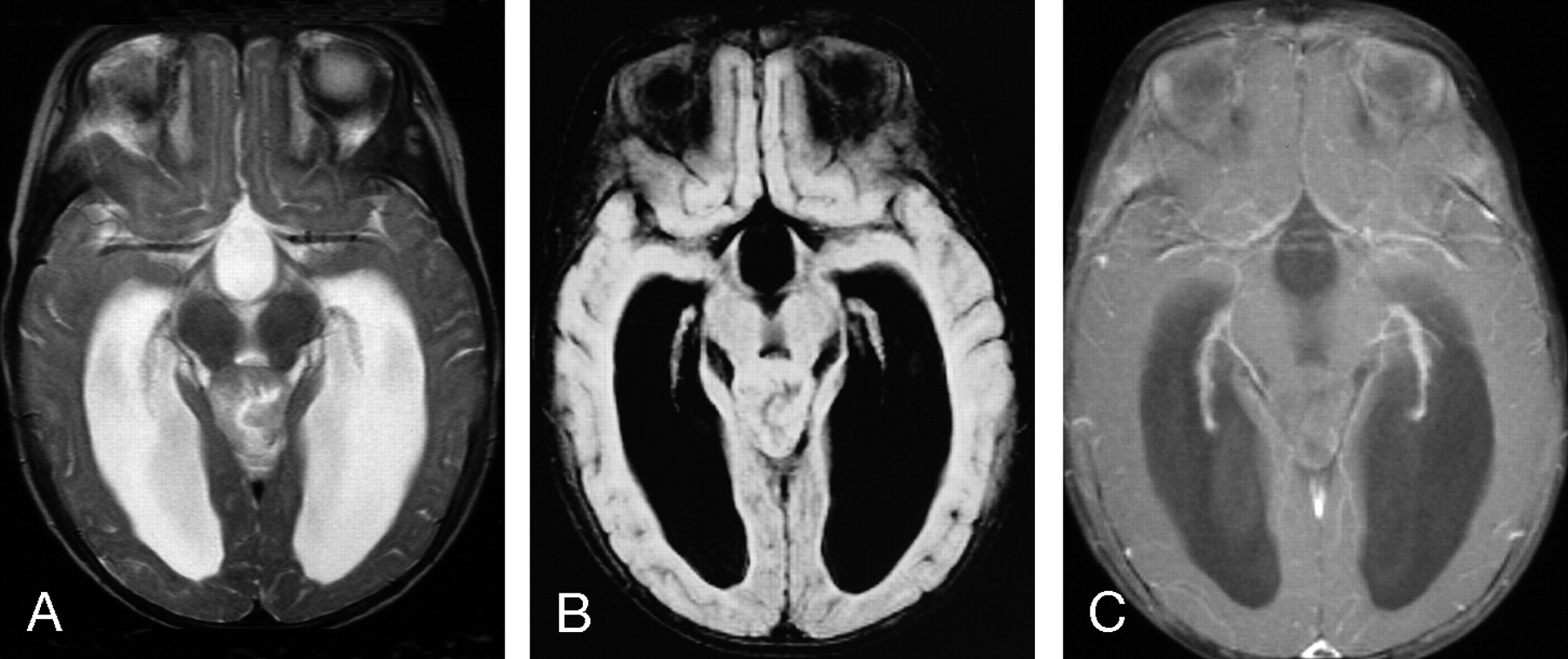
MR images of an 8-month-old female infant with AT/RT involving the pineal gland
A, Axial (TR/TE, 4000/105) MR image shows the tumor to have heterogeneous intermediate-to-slightly-high signal intensity with regions that are isointense and slightly hyperintense to gray matter, as well as a small zone of high signal intensity.
B, Axial FLAIR (TR/TE/TI, 9000/119/2200) MR image shows the tumor to have mostly intermediate signal intensity that is isointense to gray matter.
C, Axial (TR/TE, 800/20) fat-suppressed MR image with magnetization transfer shows no contrast enhancement of the primary lesion. This patient had subtotal resection of the primary lesion followed by chemotherapy. The patient had subsequent local recurrence and disseminated leptomeningeal tumor and died 7 months after initial diagnosis.
- Fig 9.
MR images of 4-year-old boy with AT/RT involving the vermis
A, Axial FLAIR (TR/TE/TI, 9000/119/2200) MR image shows the tumor to have mostly intermediate signal intensity that is isointense to gray matter.
B, Axial (TR/TE, 6000/99) MR image shows the tumor to have mostly intermediate-to-slightly-high signal intensity that is slightly hyperintense to gray matter, as well as small zones of high signal intensity.
C, Axial (TR/TE, 800/20) fat-suppressed MR image with magnetization transfer shows prominent slightly heterogeneous contrast enhancement of the tumor. This patient had gross total resection of the primary lesion followed by chemotherapy and has been disease-free for 4 years.
D, Axial DWI (b = 1000) shows the lesion to have high signal intensity.
E, Axial ADC map shows low signal intensity in the lesion, indicating restricted diffusion of water within the AT/RT.









Tables
Patient No./Age (y)/Sex Tumor Location Surgical Resection or Biopsy Disseminated Tumor at Diagnosis/MRI CSF Cytology at Diagnosis Postoperative Treatment Outcome 1/2/F Vermis Total − − R+C Dead 2/4/M Vermis Total − − R+C No evident disease 3/10/M Vermis Total − − R No evident disease 4/3.2/M Cerebellar hemisphere Subtotal − − R+C No evident disease 5/1.3/M Midbrain Biopsy + + C Dead 6/0.8/F Cerebello–pontine angle cistern Subtotal − − C Dead 7/5/M Frontal lobe Partial + − R+C Dead 8/3.4/F Frontal lobe Subtotal − − R+C Dead 9/4/M Frontal lobe Partial − − R+C Dead 10/4/F Septum pellucidum Subtotal − − R+C Dead 11/0.7/F Pineal Subtotal − − C Dead 12/0.3/F Pineal–midbrain–cerebellum Biopsy − − None Dead 13/0.8/M Pineal–midbrain–cerebellum Biopsy + + None Dead 14/6/F Vermis Total + − R+C Dead 15/15/M Frontal lobe Total − − R+C No evident disease 16/0.5/M Pineal Total − − C Dead 17/2.5/M Cervical–medullary junction Partial − − C Dead Note:—CSF indicates cerebrospinal fluid; R, radiation therapy; C, chemotherapy.
Antibody % Positive Epithelial membrane antigen 100 Vimentin 100 Actin 83 Cytokeratin 75 Desmin 23 Glial fibrillary acidic protein 87 Neurofilament protein 50 - Table 3:
Preoperative MR imaging data of 13 patients with atypical teratoid/rhabdoid tumors
Patient No./Age (y)/Sex Tumor Location Tumor Size (cm) Hemorrhage Cyst/Necrosis Long TR/Long TE (T2WI) FLAIR ADC Postgadolinium 1/2/F Vermis 3 ×3 .2 × 3.5 − + 1+ 3+/heterogeneous 2/4/M Vermis 4 × 4 × 3.4 − + 1+ iso Decreased 2+/heterogeneous 3/10/M Vermis 3.8 × 4 × 3.8 + + 1+ 1+/heterogeneous 4/3.2/M Cerebellar hemisphere 2.8 × 3.8 × 3 − + iso iso, 1+ 3+/heterogeneous 5/1.3/M Midbrain 1.2 × 1.3 × 1.2 − − 1+ 1+ 3+/homogeneous 6/0.8/F Cerebello–pontine angle cistern 3 × 3.2 × 3 − + iso 3+/heterogeneous 7/5/M Frontal lobe 6 × 6.5 × 9 + + iso iso 3+/heterogeneous 8/3.4/F Frontal lobe 5.2 × 4.8 × 6 − + iso iso Decreased 3+/heterogeneous 9/4/M Frontal lobe 4.2 × 7 × 6.5 + + iso 3+/heterogeneous 10/4/F Septum pellucidum 3.8 × 3.4 × 3.8 − + iso 1+/heterogeneous 11/0.7/F Pineal 2 × 2 × 2.5 + + 1+ iso Decreased none 12/0.3/F Pineal–midbrain–cerebellum 4 × 3 × 2.2 + + 1+ Decreased 1+/heterogeneous 13/0.8/M Pineal–midbrain–cerebellum 3.5 × 2.8 × 2.8 − + 1+ 3+/heterogeneous Note:—Signal intensity on T2WI and FLAIR refers signal of atypical teratoid/rhabdoid tumors relative to gray matter with iso (isointense) indicating the same as and 1+ and 2+ being progressively higher in signal. Apparent diffusion coefficient (ADC) of the atypical teratoid/rhabdoid tumors is listed relative to normal uninvolved gray matter. For postgadolinium contrast enhancement, none indicates no enhancement and 1+, 2+, and 3+ represent progressively greater degrees of enhancement.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Imaging Characteristics of CNS Neuroblastoma-FOXR2: A Retrospective and Multi-Institutional Description of 25 Cases
- Imaging Features with Histopathologic Correlation of CNS High-Grade Neuroepithelial Tumors with a BCOR Internal Tandem Duplication
- Radiomic Phenotypes Distinguish Atypical Teratoid/Rhabdoid Tumors from Medulloblastoma
- A Diagnostic Algorithm for Posterior Fossa Tumors in Children: A Validation Study
- Intracranial Meningeal Hemangiopericytomas in Children and Adolescents: CT and MR Imaging Findings
- Atypical Teratoid/Rhabdoid Tumors in Adult Patients: CT and MR Imaging Features