
Abstract
BACKGROUND AND PURPOSE: There may be some differences in the pathophysiology between men and women with Alzheimer disease (AD). This study was undertaken to explore the possible influence of sex on regional cerebral blood flow (rCBF) patterns in patients with AD.
METHODS: Single photon emission CT (SPECT) was performed in 30 men and 30 women with AD, and the SPECT data were analyzed by using 3D stereotactic surface projections.
RESULTS: There were no significant differences in age, duration of disease, years of education, cognitive deficits and patterns, and MR imaging findings (grade of brain atrophy and extent of white matter hyperintensity lesions) between the two groups. Both male and female patient groups showed decreased rCBF patterns in the parietotemporal lobe, posterior cingulate cortex, and precuneus, which are considered to be the characteristic SPECT findings of AD. There were, however, some differences in rCBF patterns: men had a more severe decrease of rCBF in the parietal and posterior cingulate cortex, whereas women had a more severe decrease of rCBF in the medial temporal region and frontal lobe.
CONCLUSION: These data provide evidence that patterns of rCBF deficits differ between the sexes, a finding that supports the concept of heterogeneity of the underlying pathophysiology of AD.
Alzheimer disease (AD) has a somewhat heterogeneous clinical picture and a complex disease with certain core features. Several studies have shown sex differences in cognition and behavior among patients with AD (1–5). These reports suggest that men and women may differ in the pathophysiologic changes in the brain caused by AD. Corresponding with these underlying differences, functional brain imaging using single photon emission CT (SPECT) and positron emission tomography (PET) may enable demonstration of some differences in regional cerebral blood flow (rCBF) and metabolism between men and women with AD. To date, however, few studies have examined sex differences in rCBF and metabolism in AD (6–9). We explored the influence of sex on rCBF patterns in patients with AD by using SPECT. To compare some of the differences in rCBF more easily, we analyzed SPECT data by using 3D stereotactic surface projections (3D-SSP) (10). 3D-SSP SPECT, a new image-processing and statistical program allowing pixel-by-pixel analysis of cerebral perfusion, provides a reliable and objective evaluation of the severity, extent, and localization of cortical perfusion abnormalities in patients with AD (11–14) and enables an intersubject comparison of functional brain images (13, 14). To determine whether there were differences in rCBF patterns between men and women with AD, we analyzed SPECT data by using 3D-SSP. The analysis by using the 3D-SSP technique revealed the possibility of detecting changes that are overlooked by conventional image analysis.
Methods
Patients
Ninety-nine consecutive outpatients with probable AD who underwent both SPECT and MR imaging at the Memory Disorder Clinic of the Department of Geriatric Medicine, Tokyo Medical University, between January 2001 and March 2003, were recruited for study. The clinical diagnosis of AD was based on the National Institute of Neurological and Communicative Disorders and Stroke–Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) criteria (15). Patients were excluded if they had any evidence of other neurologic or psychiatric disorders, cortical infarction, or structural brain disease other than cerebral atrophy or a single lacunar infarction or were older than 90 years old. They consisted of 30 men and 69 women whose mean age was 76.1 years ± 6.8 (range, 54–88 years). The mean score on the Mini-Mental State Examination (MMSE) (16) was 19.2 ± 3.7. Between-group comparisons were conducted by means of a pixel-by-pixel analysis of SPECT data by using the statistical program, 30 female patients with AD were sampled at random from the 69 female patients and were matched to the 30 male patients (1:1) on the basis of age and severity of cognitive disturbances as represented by their MMSE scores. Thirty similarly aged healthy control subjects included 12 men and 18 women, ranging in age from 58 to 84 years (mean age 75.1 years ± 6.4).
Informed consent for the SPECT studies was obtained from all control subjects. For patients, consent was given either by the patients themselves or their closest relative.
SPECT Imaging
All SPECT studies were performed by using a triple-head rotating gamma camera (PRISM 3000 XP, Picker, Cleveland, OH) with a fan-beam collimator that permits a spatial resolution of 6.8 mm at full width half maximum. The imaging was started 15 minutes after intravenous injection of 222 MBq (6 m Ci) of n-isopropyl-p-[123I] iodoamphetamine (IMP). The SPECT acquisition was undertaken in 24 steps (72 projections), and each step collected counts for 40 seconds. Reconstruction of the images was performed by filtered back projection using Butterworth and Ramp filters with attenuation correction (Chang, 0.09/cm). Matrix size and section thickness of the SPECT images were 128 × 128 mm and 4.3 mm, respectively. These protocols are used for routine studies at our institute.
3D-SSP Analysis
To measure the relative decrease of IMP uptake, a semiquantitative analytic approach that was originally developed for PET images by Minoshima et al (10), was adapted for the SPECT images as described elsewhere (11–14). Image analysis was performed on a personal computer equipped with a Windows 2000 operating system, in which the MS-DOS version of NEUROSTAT was implemented.
Each image set was realigned to the bicommissure stereotactic coordinate system (17). The difference in an individual’s brain size was removed by linear scaling, and regional anatomic differences were minimized by a nonlinear warping technique (18). As a result, each brain was standardized anatomically to match a standard atlas of the brain while preserving regional perfusion activity. Subsequently, maximal cortical activity was extracted to adjacent predefined surface pixels on a pixel-by-pixel basis by using a 3D-SSP technique (10). Datasets were normalized to the mean global activity. To quantify perfusion deficits, normalized brain activity of each patient was compared with that of 22 healthy control subjects by using pixel-by-pixel Z score analysis ([normal mean] –[individual value])/(normal SD). A positive Z score represents reduced rCBF in the patient relative to the control mean. To demonstrate regional patterns of rCBF alterations, two-sample t test values were calculated on a pixel-by-pixel basis between control subjects and men with AD and between control subjects and women with AD, and then transformed to Z values by a probability integral transformation. Furthermore, datasets of men with AD were compared with those of women with AD to determine differences in rCBF between the two patient groups.
MR Imaging
MR imaging was performed by using a 1.5-T whole-body imager with a transmit-receive head coil (Magnetom, Symphony; Siemens Medical Systems, Erlangen, Germany). The standardized MR imaging protocol consisted of axial T1-weighted spin-echo (TR, 450 ms; TE, 12 ms; section thickness, 5 mm; gap width, 1.5 mm; field of view [FOV], 250 ms; matrix, 256 × 256), axial T2-weighted fast spin-echo (TR, 3540 ms; TE, 106 ms; section thickness, 5 mm; gap width, 1.5 mm; FOV, 250 ms; matrix, 256 × 256), and coronal oblique T1-weighted spin-echo sequences (TR, 450 ms; TE, 12 ms; section thickness, 5 mm; gap width, 1.0 mm; FOV, 250 ms; matrix, 256 × 256). Lacunar infarctions were defined as well-demarcated small lesions (<15 mm in diameter) in the deep gray and white matter with a high signal intensity on T2-weighted images and corresponding low signal intensity on T1-weighted images. A rater (Y.T.) blindly assessed the presence of lacunar infarction, the extent and severity of hyperintense white matter lesions, ventricular and sulcal enlargement, and medial temporal lobe atrophy. White matter hyperintensities were classified as absent, punctate, early punctate, or confluent abnormalities according to the criteria of Fazekas et al (19). The rater scored the extent of ventricular and sulcal enlargement from 0 (normal size) to 3 (severe enlargement). Medial temporal lobe atrophy was scored 0 (absent) to 4 (severe atrophy) according to the subjective 5-point rating scale proposed by Scheltens et al (20).
Statistics
Values were expressed as mean ± SD. Statistical analysis was performed by using a Student t test, the Mann-Whitney U test, and the χ2 test. A P value of less than .05 was considered to indicate a statistically significant difference.
Results
No significant differences between the male and female patient groups were found in terms of age, duration of disease, years of education, or MMSE total score. In analyzing individual subtests of the MMSE, including orientation (10 points), memory (6 points), attention and calculation (5 points), language (8 points), and design copying (1 point), no significant differences were found between the two groups (Table 1). There were also no significant differences in the extent of white matter hyperintensities, presence of infarction, scores of sulcal and ventricular enlargement, and of medial temporal lobe atrophy between the two groups (Table 2).
Clinical characteristics of men and women with AD
MRI findings of men and women with AD
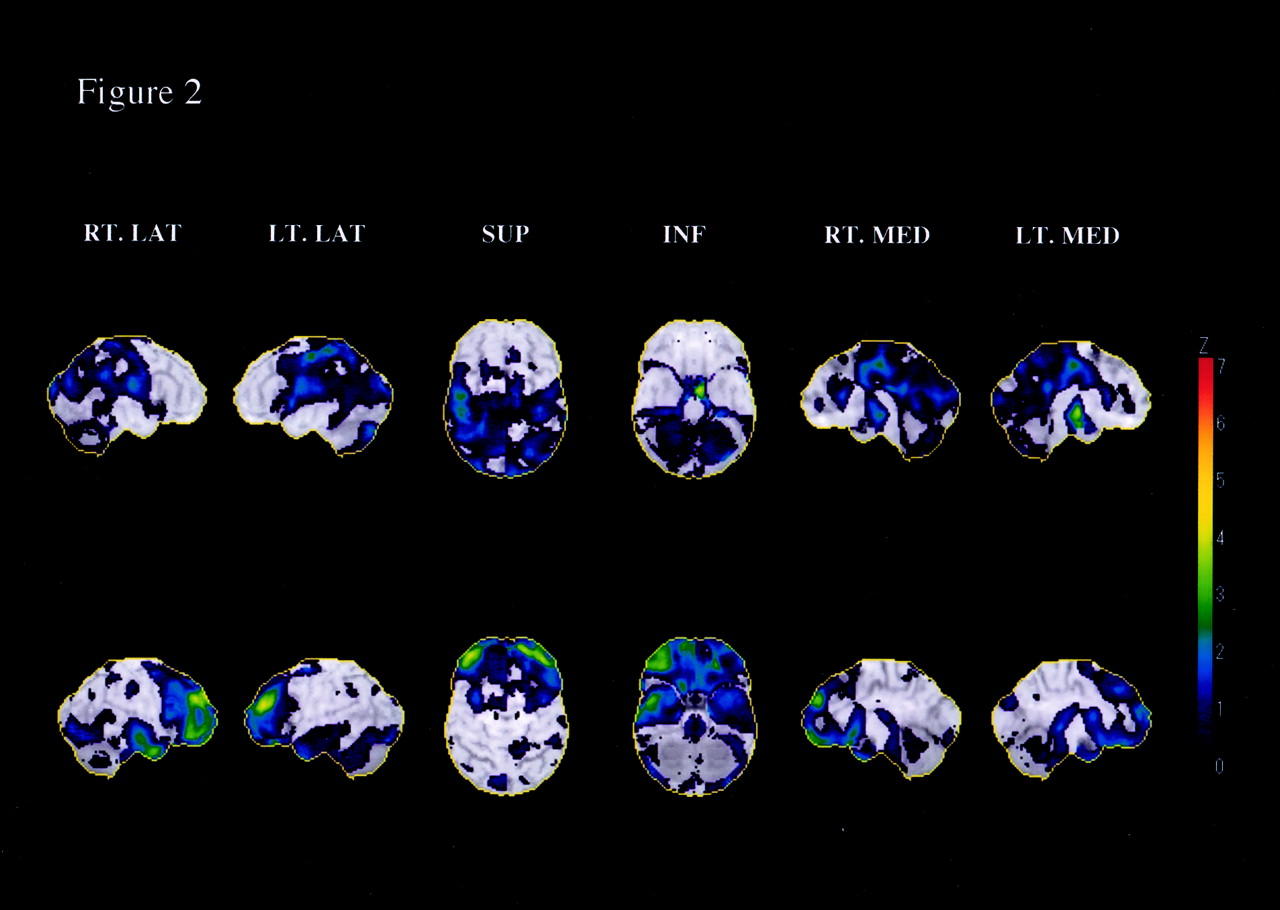
Figure 1 shows 3D views of decreased rCBF in the men with AD compared with that in control subjects and rCBF in women with AD compared with that in control subjects, respectively. Both AD groups showed significant decreases of rCBF in the parietotemporal regions, posterior cingulate cortex, precuneus, frontal association cortices, and the medial temporal lobe. The male patients, however, had a more severe reduction of rCBF in the parietal lobe and posterior cingulate cortex, whereas the female patients had reduced rCBF in additional areas, including the medial frontal lobe and medial temporal regions. Figure 2 shows 3D findings of decreased views of rCBF in men with AD compared with women with AD and in women with AD compared with men with AD, respectively. When a Z score >2 in each area on statistical maps is defined as significantly reduced rCBF, the men had a significantly greater decrease of rCBF in some areas of the temporoparietal lobe than did the women, while the women had a significant decrease of rCBF in some regions of the frontal and medial temporal lobes.

Statistical maps showing the relative decrease of rCBF in men with AD compared with that in control subjects (top) and in women with AD compared with that in control subjects (bottom).
Although both patient groups show a notable decrease of rCBF in the parietotemporal lobes, posterior cingulate cortex, cinguloparietal transitional area, and frontal association cortices, men have a more severe reduction of rCBF in the parietal lobe and posterior cingulate cortex, and women have reduced rCBF in additional areas, including the frontal lobe and medial temporal regions. The color of the outer contour corresponds to a Z score of 7.

Statistical maps showing the relative decrease of rCBF in men with AD compared with that in women with AD (top) and in women with AD compared with that in men with AD (bottom).
Men have a more severe decrease of rCBF in the parietooccipital and medial parietal lobes, whereas women have a more severe decrease of rCBF in the lateral, medial and orbital frontal lobes, and medial and inferior temporal regions. The color of the outer contour corresponds to a Z score of 7.
Discussion
We found that both male and female patient groups had decreased rCBF in the parietotemporal lobe, posterior cingulate cortex, and precuneus, which were considered to be characteristic patterns of flow reduction in AD. Men, however, had a more severe decrease of rCBF in the parietal and posterior cingulate cortex, whereas women had a more severe decrease of rCBF in the medial temporal region and frontal lobe. The two groups did not differ in terms of demographic variables such as age, duration of the disease, years of education, cognitive deficits and patterns, brain atrophy, white matter changes, or infarction, which may potentially influence patterns of rCBF deficits. Our results suggest that sex may also somehow modify the rCBF deficits of AD patients.
Various studies have examined sex differences in the pathophysiology of AD, including neuropsychological performances (1–5), brain structure as measured by MR volumetry (21, 22), rCBF and metabolism by using SPECT and PET (6–9), and phosphorus metabolism by using MR spectroscopy (23). Some differences in cognition and behavior were pointed out between men and women with AD. Researchers have shown that women perform significantly worse than do men in some memory tests and language abilities (1–5). These findings may be related to several factors, including hormonal status, exogenous environmental risk factors and living situations, and different patterns of neural organization that could influence cognition and language. In the present study, we found no significant differences in patterns of cognitive impairments, assessed by the MMSE, between men and women with AD. Therefore, we did not conclude that our findings may be associated with patterns of neuropsychological deficits. With regard to this point, however, correlative studies with functional imaging and more detailed neuropsychological tests will be needed in the future.
To our knowledge, few studies have examined sex differences in rCBF patterns. In a visual inspection of SPECT scans from 104 patients with AD, Nitrini et al (6) showed that parietotemporal hypoperfusion was more frequent in men than in women. Another qualitative SPECT study demonstrated that unilateral left hemispheric defects were found more often in women than in men, which indicates greater heterogeneity in rCBF of women than men (7). A preliminary report examining the effects of demographic factors on SPECT findings in subjects with AD also found that lower MMSE scores and male sex significantly predicted parietotemporal hypoperfusion (8). Although those studies are methodologically different from ours in terms of data analysis (qualitative analysis versus statistical imaging analysis), our findings are in agreement with previous studies. Because random selection of the 30 female patients in the present study may bias our results, SPECT data of the remaining 39 women were compared with those of control subjects and men with AD (data not shown); however, we had similar results showing that women had less reduced rCBF in the parietotemporal and posterior cingulate cortex than men. Therefore, our unexpected findings are likely to reflect underlying pathophysiological differences between men and women more than chance effects.
In healthy adults, subtle differences in rCBF and metabolism have also been found between the sexes. The findings of these studies have been inconsistent with respect to regional brain areas, probably influenced by such variables as imaging technique, the tracer used, data analysis, and the characteristics of healthy volunteers (eg, age, education, and handedness). It was shown that rCBF and metabolism in parietal and cingulate regions were more decreased in men than in women (24–26). Women were shown to have decreased rCBF and metabolism in the frontal, temporolimbic, and hippocampal regions by some studies (25, 27–29), but the findings contrast with those of other studies (24, 26, 30). It is interesting to mention that the sex differences in healthy adults found by some, but not all, previous reports seem to be somewhat similar to rCBF differences between men and women with AD.
The mechanism by which sex differences in rCBF patterns of AD may occur remains to be fully explained. A recent study from a large sample of 729 brains in which autopsy was performed suggests that AD-related abnormalities such as neurofibrillary tangle and senile plaque is affected by a complex interaction between the aging process, sex, and genetic risk factors (ApoE 4) (31). In contrast, another autopsy study of 138 cases indicated that the risk for Aβ deposits and development of senile plaque is similar in both sexes (32). As the authors of the study mentioned, however, it is possible that sex differences may exist in the way neurons and glia react to the accumulation of Aβ. Eventually, these differences may lead to variability in the clinical expression and rCBF deficits of AD between men and women. On the other hand, various studies have suggested some modulating effects of estrogen on the nervous system. Beneficial effects of estrogen in lowering the risk of AD have been suggested by epidemiologic, clinical, and basic scientific research (33, 34). In a study of ovarian hyperstimulation in normal women, estrogen levels directly correlated with increases in rCBF (35). Ohkura et al (36) reported that patients with AD who were treated with oral estrogen show an increase in rCBF. These studies suggest an influence of estrogen status on rCBF patterns. It is not clear whether sex differences in rCBF deficits may relate to a lack of activational effects of estrogen in postmenopausal women or some other sex difference, but this warrants further investigation.
Conclusion
Men with AD had a more severe decrease of rCBF in the parietal and posterior cingulate cortex, whereas women with AD had a more severe decrease of rCBF in the medial temporal region and frontal lobe. The fact that a typical distribution pattern of reduced perfusion was less prominent in women than in men indicates that the sensitivity of SPECT for the diagnosis of AD is reduced in female patients. Our findings may point to the heterogeneity of AD according to sex.
Acknowledgments
We thank J. Umeda and H. Hirose, of the Department of Nuclear Medicine of Tokyo Medical University, for their support and technical assistance. We are also grateful to Professor J. Patrick Barron, of the International Medical Communications Center of Tokyo Medical University, for his review of the manuscript.
References
- Received October 7, 2003.
- Accepted after revision December 20, 2003.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}