
Article Figures & Data
Figures
- Fig 1.
Patient 8. Bifrontal and right parafalcine SDE.
A. Axial T1WI (650/14) shows slight hypointensity in the SDE (arrows).
B, Axial T2WI (6000/99) shows intermediate signal intensity in the bifrontal collections (arrows) and hyperintensity in the right parafalcine collection (arrowheads).
C, Coronal contrast-enhanced T1WI (800/20) with MT shows irregular capsular enhancement of the collections (arrows).
D and E, Axial DWI (4000/110, b = 1000 s/mm2) and ADC map show reduced water diffusion in the SDE.
- Fig 2.
Patient 1. Right SDE and left RSE.
A, Axial T1WI (650/14) shows intermediate signal intensity in the right SDE and hypointensity in the left RSE.
B, Axial T2WI (6000/99) shows high signal intensity in both subdural collections. Strands of intermediate signal intensity (arrows) are noted in the right SDE.
C, Axial contrast-enhanced T1WI (800/20) with MT shows peripheral enhancement of both subdural collections. The enhancement is thicker in the right SDE (arrows) than in the left RSE (arrowheads).
D, Axial DWI (4000/110, b = 1000 s/mm2) shows mixed high (arrows) and low signal intensities in the right SDE.
E, Corresponding ADC map shows mixed low (arrows) and high signal intensities in the right SDE, indicating heterogeneous water motion. Increased water motion is noted in the left RSE.
- Fig 3.
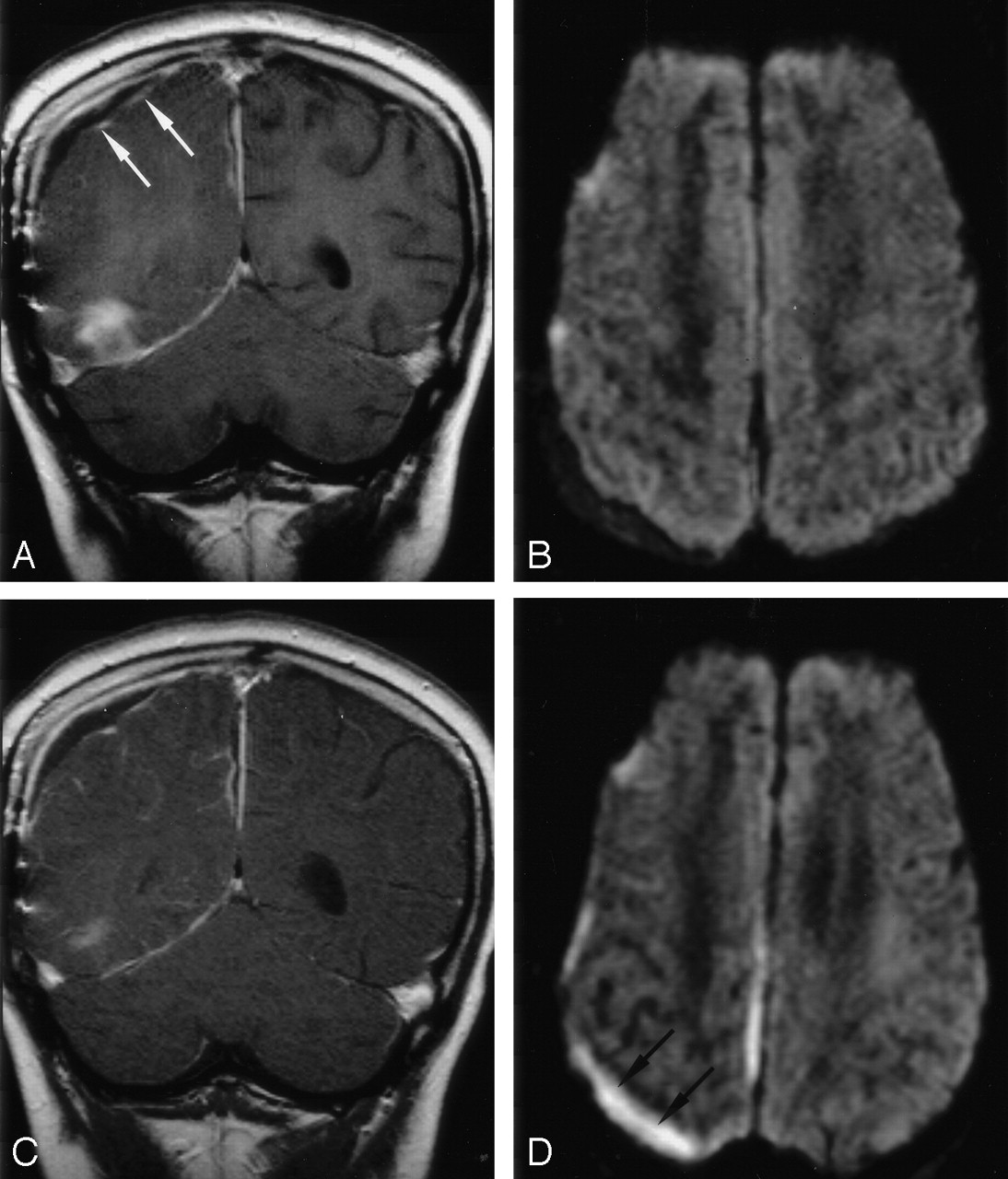
Patient 7. Follow-up DWI show superimposed infection of a right RSE in this 10-year-old boy with right temporal and parafalcine SDEs.
A, Coronal contrast-enhanced T1WI (800/20) with MT shows capsular enhancement (arrows) of the right parietal subdural collection and the anterior aspect of the right temporal base SDE.
B, Axial DWI (4000/110, b = 1000 s/mm2) shows increased diffusion in the collections.
C, Follow-up coronal contrast-enhanced T1WI (800/20) with MT shows no substantial change in the capsular contrast enhancement of the collection.
D, Follow-up axial DWI (4000/110, b = 1000 s/mm2) shows increased signal intensity in the collection (arrows) and the interhemispheric fissure, suggesting superimposed infection.



Tables
Patient (No)/ Sex/Age Source of Infection Clinical Findings at Admission*/Duration, d WBC Count, ×103/dL Pathogen Treatment 1/M/4 mo Meningitis Fever; irritability; stiff neck/15 4.4 Escherichia coli (CSF) Antibiotics, burr hole drainage 1/M/14 y Sinusitis S, E, M Fever; swollen, painful L eye/4 12.6 Moraxella species (sinus) Antibiotics, FESS, orbital drainage 3/F/13 y Sinusitis F, S, E, M Fever; headache; slurred speech, R extremity weakness/14 17.4 Group A Streptococcus (subdural collection) Antibiotics, Craniotomy 4/M/5 wk Meningitis Fever; vomiting/4 24.9 Pasteurella multocida (CSF) Antibiotics 5/M/16 y Sinusitis F, S, E, M Fever; swollen, painful L eye, photophobia, impaired gaze; seizure/4 12.6 Streptococcus milleri species (subdural collection) Antibiotics, FESS, craniotomy, preseptal drainage 6/M/13 y Meningitis Fever; hallucinations/4 30.6 Peptostreptococcus anaerobius, Prevotella melaninogenica (CSF) Antibiotics, FESS 7/M/10 y Right mastoiditis Fever; headache; seizure/10 6.1 Streptococcus equiinus, Micrococcus species (subdural collection) Antibiotics, Craniotomy 8/F/17 y Sinusitis F Fever; headache; L extremity weakness/3 13.4 S milleri species (subdural collection) Antibiotics, FESS, craniotomy 9/F/8 y Sinusitis S, E, M Fever; seizure, R hemiparesis, R facial palsy/5 19.8 Streptococcus mitis (blood) Antibiotics, FESS, craniotomy 10/M/13 y Sinusitis F, S, E, M Fever; headache; painful neck; photophobia/7 22.1 Veillonella species, Propionibacterium granulosum (sinus) Antibiotics, FESS, anticoagulants Note.—Patient 6 died; all others recovered. E indicates ethmoid; F, frontal; FESS, functional endoscopic sinus surgery; M, maxillary; and S, sphenoid.
* Systemic and neurologic signs.
Patient (No.) Location of SDE Initial MR Study* ADC, ×10−3 mm2/s Associated Abnormalities Duration between Initial and Follow-up MR Studies, d Clinical Features at Follow-up MR Imaging Follow-up MR Study* T1WI T2WI Enhanced† DWI Enhanced† DWI 1 R FP Hypo Mild hyper Thick, linear Hyper, hypo 0.892 L RSE (thin, linear)† 21 Fever Thick, linear Hyper, hypo 2 L F Hypo Hyper Thick, linear Hyper NA L orbital cellulites 16 Fever Thick, linear Hyper 3 L FP Iso Hyper Thick, irregular Hyper NA NA NA NA NA NA 4 B FPO Iso Mild hyper Thick, linear Hyper 0.644 NA 12 Fever, seizure Thick, linear Hyper 5 L F Iso Hyper Thick, linear Hyper 0.306 L orbital cellulites NA NA NA NA 6 Mid F base Hypo Hyper Thick, linear Hyper NA NA NA NA NA 7 R pF, R PO, R T Mild hypo Iso Thick, linear Hyper 0.642 R RSE (thin, linear)† infected later 5 Fever Thick, linear Hyper 8 B F, R pF Iso Mild hyper Thick, linear Hyper 0.698 NA 23 Fever, chills Thick, linear Hyper 9 L FP, L pF Iso Mild hyper Thin, linear Hyper 0.438 NA 6 Fever, R hemiparesis Thin, linear Hyper 10 L CPA Hypo Hyper Thick, linear Hyper 0.608 Cavernous sinus infection 10 Afebrile, leukocytosis (blood) Thick, linear Hyper Note.—B indicates bilateral; CPA, cerebellopontine angle; F, frontal; FP, frontoparietal; FPO, fronto-occipitoparietal; Hyper, hyperintense; hypo, hypointense; Iso, isointense; NA, not available or not applicable; pF, parafalcine; PO, parieto-occipital; T, temporal; T1WI, T1-weighted image; and T2WI, T2-weighted image.
* Signal intensity relative to that of gray matter.
† Morphology of the enhancing membrane.
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Subdural and subarachnoid empyema as a complication of an acute meningococcal meningitis
- Subdural empyema in bacterial meningitis
- Role of imaging in the diagnosis of acute bacterial meningitis and its complications
- The clinical challenge of recognizing infratentorial empyema
- Unusual findings in cerebral abscess: report of two cases.