
Abstract
BACKGROUND AND PURPOSE: Percutaneous vertebroplasty is known for its pain-relieving effect. Our purpose was to evaluate its effect on the kyphosis angle, wedge angle, and height of the fractured vertebral body.
METHODS: We reviewed digital radiographs of 73 vertebral bodies in 53 patients before and after vertebroplasty. We measured the spinal kyphosis angle and the wedge angle of the fractured vertebral body. Ratios of the height of the anterior border, center, and posterior borders of the collapsed vertebra to the height at the posterior border of an adjacent normal vertebral body were measured. Gain from vertebroplasty and the restoration percentage (gain divided by loss) were calculated for each parameter.
RESULTS:The kyphosis angle, wedge angle, anterior height, center height, and posterior height significantly improved after vertebroplasty. The mean reduction in the kyphosis angle was 4.3°, and the wedge-angle reduction was 7.4°. The mean wedge-angle reduction in fractured vertebral bodies containing gas was 10.2°. Restoration percentages for the kyphosis angle and wedge angle were 19% and 44%, respectively. Gain in the height of the fractured vertebral bodies was 16.7% for the anterior border, 14% for the center, and 7% for the posterior border. Restoration percentages for the height of the vertebral body were 29% for the anterior border and 27% for the center.
CONCLUSION: Vertebroplasty increases the height of the fractured vertebra and reduces the wedge and kyphosis angles. These effects are most remarkable in fractured vertebra containing gas.
Percutaneous vertebroplasty is a therapeutic method in which the vertebral body is percutaneously filled with acrylic cement for pain relief. Galibert et al (1) performed the first percutaneous vertebroplasty procedure to treat an extensive hemangioma in the C2 vertebral body. Vertebroplasty was initially used for the treatment of spinal tumors, such as angiomas, metastases, and multiple myelomas (2); however, osteoporotic vertebral collapse has gradually been accepted as an indication for percutaneous vertebroplasty (3, 4).
Kyphoplasty, or percutaneous balloon kyphoplasty, is a technique to create cavities within the fractured vertebral body and to elevate the endplates by inflating balloons inside the vertebral body, followed by fixation of the fracture with bone cement. Some have assumed that kyphoplasty offers the additional advantage of realigning the spinal column and regaining height in the fractured vertebra; these benefits may help decrease the pulmonary and gastrointestinal complications and early morbidity related to compression fractures (5–7).
The effect of vertebroplasty in pain relief has been discussed extensively. Nevertheless, the kyphosis-correction and height-restoration effects of percutaneous vertebroplasty have rarely been reported (8, 9). In this study, we determined these effects of percutaneous vertebroplasty.
Methods
Patients
Between June 2000 and November 2002, we performed 84 percutaneous vertebroplasty procedures in 121 vertebral bodies in 66 patients. Digital imaging files for both prevertebroplasty and postvertebroplasty thoracolumbar spinal radiographs were retrieved from the picture archiving and communication system (PACS) for analysis. Patients with prevertebroplasty thoracolumbar radiographs from other hospitals without digital files in our PACS were excluded from analysis. In those patients undergoing more than one session of vertebroplasty, we analyzed only the vertebral bodies treated in the first session. All radiographs were obtained with the patient in the left lateral decubitus position and within 14 days before and after vertebroplasty. Finally, the radiographs of 73 vertebral bodies in 53 patients (34 women, 19 men; mean age, 75.5 years) obtained before and after vertebroplasty were available for measurement. All patients, except for one with steroid-induced osteoporosis, were older than 60 years.
Thirty-six patients underwent vertebroplasty for one vertebra; 14 patients, for two vertebrae; and three patients, for three vertebrae. In all patients, fractures were attributed to osteoporosis, without evidence of a neoplasm, on the basis of the clinical data and the imaging presentation. Vertebroplasty was performed within 6 months from the onset of pain in 48 patients and between 6.5 months to 3 years in five patients
Patient Selection for Percutaneous Vertebroplasty
Inclusion criteria included the following: a painful vertebral compression fracture refractory to medical therapy, depiction of the fracture on plain radiographs, and tenderness elicited at the spinous process corresponding to the fractured segment.
Before vertebroplasty, whole-body bone scanning was performed in all patients. The images showed corresponding uptake at the fractured level. If a neurologic deficit was observed, a CT scan or MR image was obtained to determine the presence of any associated problems, such as spinal cord compression, disk herniation, spinal stenosis, spondylolisthesis, or nerve root compression. Only osteoporotic patients without evidence of a tumor were included in this study.
In our institution, exclusion criteria for vertebroplasty were the following: 1) compromise of the spinal canal by more that 20%, as a result of retropulsed fragments; 2) collapse of the vertebral body with a height loss of more than 90%, so that there was no place for a needle to enter the vertebral body between the endplates; and 3) an old fracture with long-standing back pain of longer than 1 year (with the exception of vertebral bodies containing gas or movement at the fractured vertebral body on flexion and extension lateral views).
Technique of Percutaneous Vertebroplasty
One of the authors (M.M.H.T., assisted by C.-J.W. and F.-C.C.) performed percutaneous vertebroplasty by using a transpedicular approach with the patient under local anesthesia. A method modified from that of Jensen et al (4) was used. The patient was placed in prone position on the examination table used for biplane angiography. We put pillows under the patient’s upper chest and lower abdomen for comfort and to reduce the wedge angle of the fractured vertebral body (Fig 1). We maintained a small gap between the top of the table and the anterior wall of the patient’s body at the level of the fracture during vertebroplasty, unless the wedge deformity of the vertebral body under treatment had been corrected by the prone positioning. We used an 11-gauge bone marrow biopsy needle (Hakko Electric Machine Works Co., Nagano, Japan) to puncture the collapsed vertebral body through either one of the pedicles and advanced the needle to the anterior third of the vertebral body under fluoroscopic guidance. Vertebroplasty was performed via unilateral puncture through the pedicle for 71 vertebral bodies and via bipediculate puncture for two vertebral bodies. Bone cement was prepared by mixing the copolymer powder with sterile barium sulfate to enhance its radiopacity (15:6 by weight), followed by the addition of the monomer liquid for polymerization (OsteoBond; Zimmer, Warsaw, IN). We manually injected the bone cement into the vertebral body under direct fluoroscopic control. We immediately terminated the injection of bone cement when one of the following signs was observed: 1) cement reaching the posterior fourth of the vertebral body; 2) radiopaque bone cement in intervertebral, epidural, or perivertebral veins; or 3) significant leakage into the disk space. After the procedure, the patient was maintained in the prone position for approximately 30 minutes and turned to the supine position for another 30 minutes before mobilization.

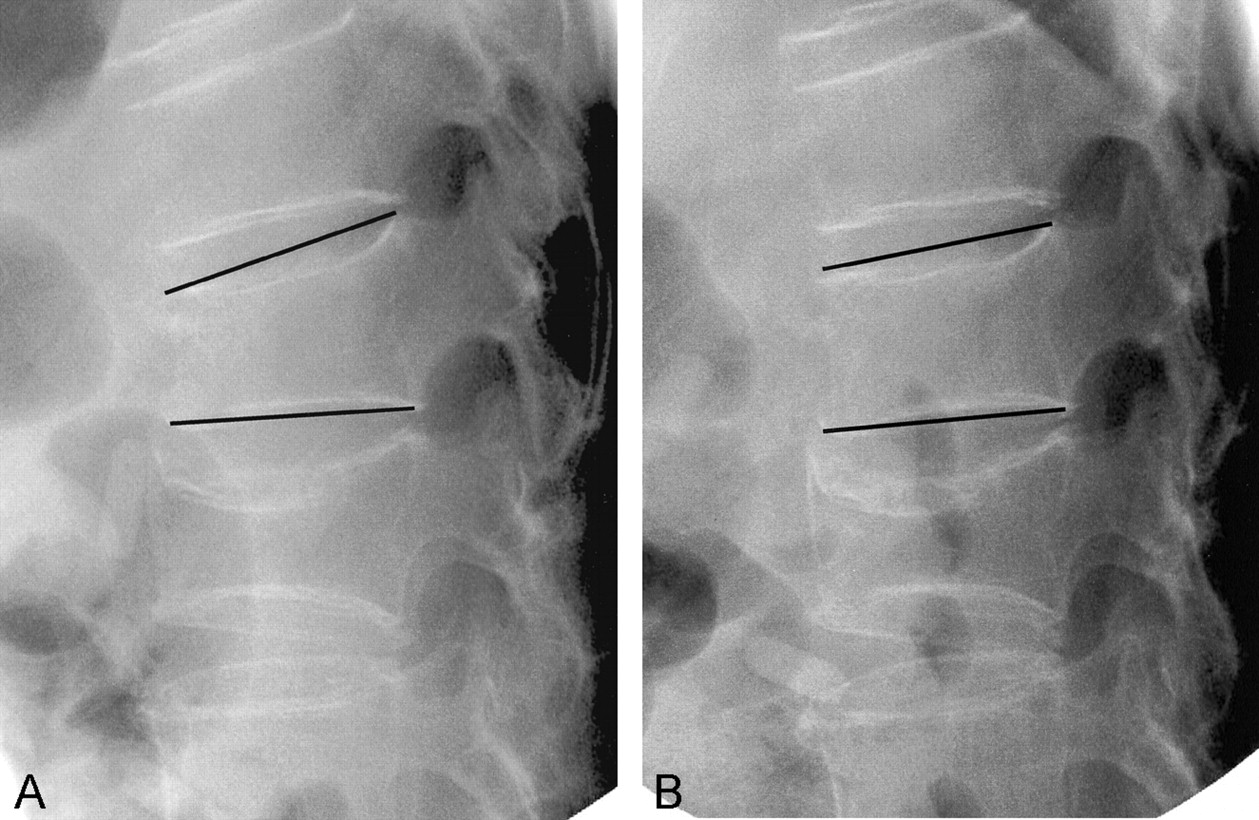
Horizontal beam lateral view of a patient before (A) and after (B) padding with pillows under the upper chest and lower abdomen. The patient has severe back pain and tenderness at the L1 level. The wedge angle of the L1 vertebral body (marked) is 15 degrees before padding, and 7 degrees after padding. The anterior, midline, and posterior vertebral height of L1 increased by 4.7 mm, 3.3 mm, and 0 mm, respectively. L2 is an old fracture. No change in height or wedge angle at L2 level is found before and after padding.
Data Acquisition and Analysis
Digital files of the patient’s prevertebroplasty and postvertebroplasty radiographs were retrieved for the measurement of the following: 1) kyphosis angle; 2) wedge angle of the collapsed vertebral bodies; 3) height of the anterior, center, and posterior aspects of the collapsed vertebral body; and 4) height of the posterior border of an adjacent normal vertebral body. All of these measurements were performed by using the PACS imaging display software (SmartView, Taiwan Electronic Data Processing Corp, Taipei County, Taiwan). The kyphosis angle was determined by using the Cobb method on a lateral view of the spine. The wedge angle was defined as the angle between the superior endplate line and the inferior endplate line of the fractured vertebral body (Fig 2). To correct the possible differences in the magnification ratio on the radiographs acquired before vertebroplasty and those acquired after, we calculated the ratio of the height of the collapsed vertebral body at the anterior border, at the center, and at the posterior border on the lateral view to the height of the posterior border of an adjacent normal vertebral body as a reference (Fig 2). We selected the same vertebral body for measuring the posterior border on the lateral radiographs obtained before and after vertebroplasty. A trained research assistant (L-C.W.) performed these measurements. Maps of the angles and lines used for measurement were stored and then confirmed by two neuroradiologists (C.-B.L., J.-F.L.).

Measurement of the collapsed vertebral body and reference line. Height of a collapsed vertebral body was measured at the anterior border (A), center (C), and posterior border (P). The height of the posterior border (NP) of an adjacent normal vertebral body was measured for reference. The wedge angle (θ) in this case is 28 degrees before vertebroplasty (A) and 11 degrees after vertebroplasty (B).
Intraobserver and interobserver reproducibility of these measurements was evaluated by using intraclass correlation coefficients. We tried to avoid any biases that could have occurred in the post-treatment measurements by ignoring the focal protrusion of bone cement and by discussing the measurements between authors to establish a consensus.
The effects of the changes in the kyphosis angles, wedge angles, and height ratios before and after vertebroplasty were statistically analyzed by using a paired-sample t test.
We carefully examined the prevertebroplasty radiographs and found that gas was present in 39 vertebral bodies in 34 patients (designated as the gas group) and absent in 34 vertebral bodies of 19 patients (designated as the non-gas group) (Table 1). We statistically compared the effects of correcting the kyphosis and restoring the height of the vertebral body with vertebroplasty in respect to the presence of gas. For this analysis, an independent-samples t test was used.
Number of vertebral bodies treated and number containing gas
Loss-and-Gain Relationship and Restoration Percentage
To address whether the extent of kyphosis correction and vertebral-height restoration (gain) after vertebroplasty was related to the extent of initial vertebral-body collapse (loss), we analyzed these parameters before and after vertebroplasty by performing linear regression. The loss-and-gain relationship was expressed as the gain-to-loss ratio, or the restoration percentage (Table 2). The restoration percentage indicated the percentage of recovery from the initial loss.
Terms and formulas for loss and gain for different parameters
To illustrate the wedge angle of a fractured vertebra, the loss from fracture was the wedge angle before vertebroplasty (pre): (wedge angle)pre.
Gain from vertebroplasty in the wedge angle was the wedge-angle reduction, represented as follows: (wedge angle)pre − (wedge angle)post, where post indicates wedge angle after vertebroplasty.
Thus, the restoration percentage of the wedge angle was obtained from the following: [(wedge angle)pre − (wedge angle)post]/(wedge angle)pre.
Similarly, the loss of height at the anterior border of the vertebral body due to the fracture was represented as follows: 1 − (A/NP)pre, where A is the height of the anterior aspect of the collapsed vertebral body, and NP is height of the posterior border of an adjacent normal vertebral body.
The gain in height at the anterior border of the vertebral body from vertebroplasty was represented by the following: (A/NP)post − (A/NP)pre.
Thus, the restoration percentage of the height at the anterior border of the vertebral body was calculated as follows: [(A/NP)post − (A/NP)pre]/[1 − (A/NP)pre].
Terms used for the calculation of the loss, gain, and restoration percentage of the other parameters are shown in Table 2.
Results
Reproducibility of the Measurements
Intraobserver and interobserver reproducibility was measured by means of intraclass correlation coefficients. Intraobserver reproducibility was high for the height of the vertebral body, the kyphosis angle, and the wedge angle. For these parameters, the intraclass correlation coefficients (L-C.W.) were 0.98, 0.98, and 0.88, respectively. Interobserver reproducibility was 0.94 (between L-C.W. and J.-F.L.) and 0.94 (between C.-B.L. and L-C.W.) for the heights of the vertebral body, 0.97 (between L-C.W. and J.-F.L.) and 0.99 (between C.-B.L. and L-C.W.) for the kyphosis angle, and 0.92 (between L-C.W. and J.-F.L.) and 0.80(between C.-B.L. and L-C.W.) for the wedge angle.
Effect on the Kyphosis Angle and Wedge Angle
Reduction of the kyphosis angle after vertebroplasty was found in 45 of 53 patients (85%). Reduction of kyphosis by more than 5° was found in 26 of 53 patients (49%). The reduction in the kyphosis angle after vertebroplasty was statistically significant (P < .001) for all 53 patients, for the non-gas group (n = 19), and for the gas group (n = 34), with values of 4.3° ± 5.4, 2.4° ± 4.1, and 5.3° ± 5.8, respectively (Table 3). The reduction of the kyphosis angle after vertebroplasty was greater in the gas group than in the non-gas group, but the difference were not statistically significant (P = .064) (Table 4).
Parameters before and after vertebroplasty and gain after vertebroplasty
Comparison of gain in parameters for gas and nongas groups
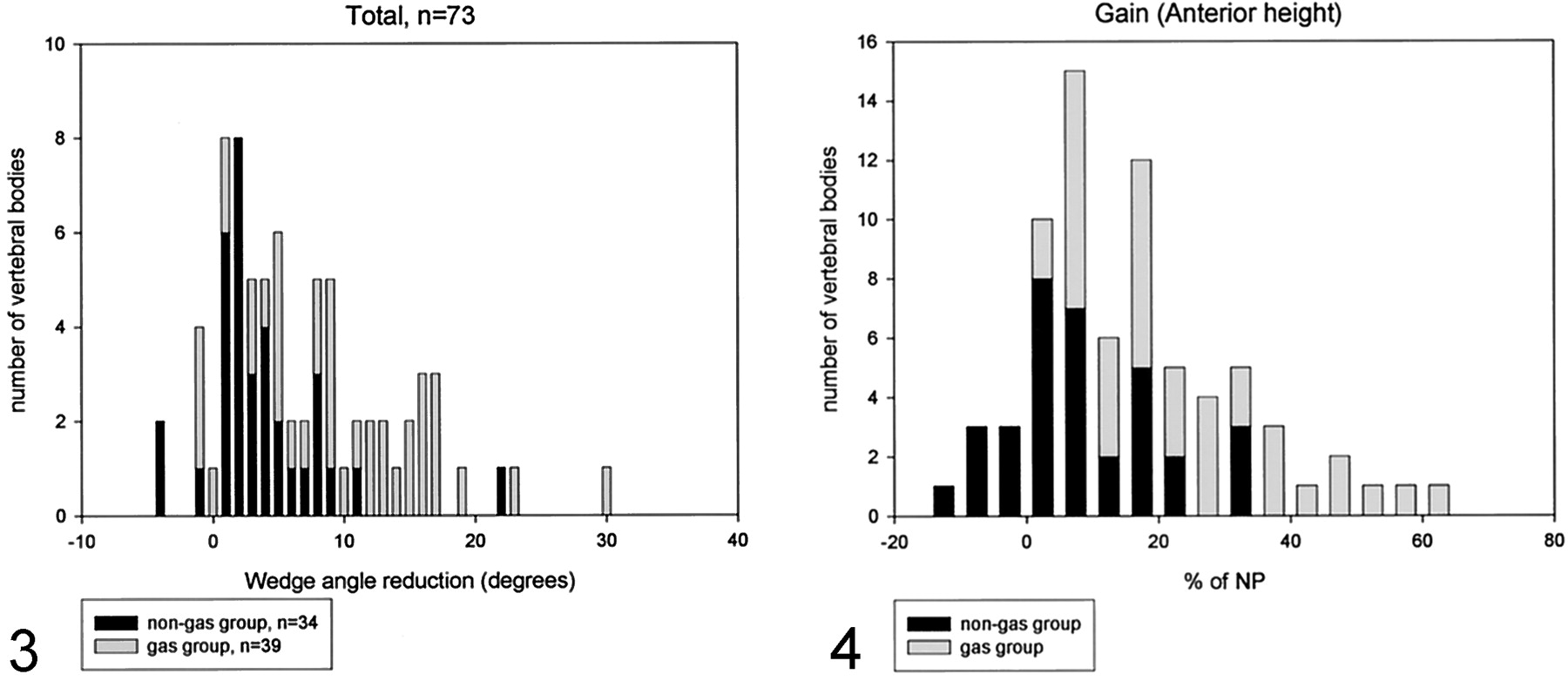
Reduction in the wedge angle after vertebroplasty was shown in 67 of 73 vertebral bodies (92%). Reduction of the wedge angle by more than 5° was found in 40 of 73 vertebral bodies (55%). The reduction of the wedge angles was statistically significant (P < .001) for all 73 vertebral bodies, for the non-gas group (n = 34), and for the gas group (n = 39), with values of 7.4° ± 6.7, 4.1° ± 4.6, and 10.2° ± 7.0, respectively (Table 3). The wedge angle reduction was more remarkable in the gas group than in the non-gas group (P = .022) (Table 4, Fig 3).

Wedge angle reduction in 73 vertebral bodies. Most vertebral bodies in the gas group were on the right-hand side of the x-axis; therefore, the gas group had more wedge angle reduction.
Fig 4. Gain of the anterior height from percutaneous vertebroplasty in 73 vertebral bodies. The gain is more remarkable in the “gas” group (P = .001).
Gain in Vertebral-Body Height with Vertebroplasty
Table 3 shows the vertebral height at the anterior border, center, and posterior border before and after vertebroplasty, the differences before and after vertebroplasty, and the P values. All of these parameters showed a significant change when values before vertebroplasty were compared values after vertebroplasty by using a paired sample t test (Table 3, Fig 4).
We also investigated whether the posterior vertebral height was affected in compression fracture before vertebroplasty by determining the value for 1 − (P/NP), where P is the height of the posterior aspect of the collapsed vertebral body, and NP is height of the posterior border of an adjacent normal vertebral body. Our data showed a mean decrease of 20% in the vertebral height at the posterior border. Collapse of the posterior part of vertebral bodies was more remarkable in the gas group than in the non-gas group (24% and 17%, respectively).
Vertebroplasty resulted in a gain in height at the anterior border, at the center, and at the posterior border, in both the gas and non-gas groups. However, vertebroplasty resulted in a statistically greater height gain for the gas group than for the non-gas group at the anterior border (P = .001) and at the center (P = .008) of the vertebra (Table 4).
Loss-and-Gain Relationship
The wedge-angle reduction after vertebroplasty appeared to be most directly related to the original wedge-angle loss before vertebroplasty (R2 = 0.369). We found a tendency for greater gain (wedge-angle reduction after vertebroplasty) for cases with more original loss (wedge angle before vertebroplasty) in the correlation plot of gain versus loss for wedge-angle change (Fig 5). In comparison with the non-gas group, the gas group generally had a larger original wedge angle and a greater wedge-angle reduction after vertebroplasty (Fig 5).

Correlation plot of gain (the wedge angle reduction)versus loss (original wedge angle) after vertebroplasty. There is a trend toward higher gain in cases with more original loss. Most cases of the “gas” group are in the right upper quadrant, whereas most cases of the “non-gas” group are in the left lower quadrant, suggesting that the gas group had larger wedge angle before vertebroplasty and more wedge angle reduction after vertebroplasty. After linear regression analysis, the slope for the “gas” group (0.61) is significantly larger than that for the “non-gas” group (0.24), again confirming the wedge angle reduction effect was more obvious in the “gas” group.
Fig 6. Correlation plot of the gain from percutaneous vertebroplasty versus the loss from fracture for the anterior border of collapsed vertebral bodies. There is a trend toward higher gain in cases with more original loss. Most cases of the “gas” group are in the right upper quadrant, whereas most cases of the “non-gas” group are in the left lower quadrant, suggesting the gas group had larger initial loss of height before vertebroplasty and more gain after vertebrolasty. The regression line for the “gas” group is higher than the “non-gas” group, which confirms again that the vertebroplasty resulted in better height restoration at the anterior border of the collapsed body in the “gas” group.
Among different parameters depicting the changes in the height of the vertebral body after the vertebroplasty, the anterior border showed the best correlation of the loss-and-gain relation (R2 = 0.304), followed by the center (R2 = 0.216), and the posterior border (R2 = 0.164). There was a trend toward greater gain (increase in the anterior height of the vertebral body with vertebroplasty) for cases with more original loss (original shortening of anterior height of the vertebral body height due to fracture before vertebroplasty), as shown on the correlation plot of gain versus loss (Fig 6). In comparison with the non-gas group, the gas group generally had a larger original loss in height and a greater gain in height at the anterior border after vertebroplasty (Fig 6).
Restoration percentages are reported in Table 5. The wedge angle had the best restoration percentage, followed by height at the anterior border, the height at the center, and the kyphosis angle. The restoration percentage was better in the gas group than in the non-gas group for all of these parameters.
Restoration percentage, or gain-to-loss ratio
Discussion
To examine the effect of vertebroplasty on the reduction of the wedge angle and on the restoration of height for the collapsed vertebral bodies, we analyzed different parameters before and after vertebroplasty. We calculated the gain in different parameters and their restoration percentage. From our results, the restoration percentage was highest for the wedge angle, followed by height at the anterior border and height at the center (Table 5). The remarkable restoration percentage for the wedge angle may be attributed to the following factors: 1) The padding beneath the upper chest and pelvic region of the patient may have reduced the wedge angle of the collapsed vertebral body. 2) The anterior vertebral height significantly increased by 16.7% after vertebroplasty, much more than the posterior vertebral height did. 3) The bone cement was injected and deposited mainly in the anterior four-fifths of the collapsed vertebral body for reasons of safety.
The effect of vertebroplasty on reduction of the kyphosis angle was, however, less remarkable (Tables 3 and 5). The mean reduction in the kyphosis angle after vertebroplasty was smaller than the mean wedge angle reduction. The kyphosis angle is affected by the relative position of adjacent vertebral bodies and intervertebral disk spaces, in addition to the individual wedge angle of the vertebral body. Therefore, the reduction in the wedge angle was more than the reduction of the kyphosis angle. The measurement of the kyphosis angle might have been affected by a slight change in the patient’s body position at the time the lateral radiographs of the thoracolumbar spine were acquired.
Percutaneous balloon kyphoplasty has been reported to be an effective technique for improving the height of the fractured vertebra and for alleviating kyphosis (5–7); however, the balloon catheter is expensive. In the report by Garfin et al (6), the gains in the height at the anterior border, center, and posterior border of the fractured vertebral body after kyphoplasty were 16%, 16%, and 14%, respectively. Our data for these parameters after vertebroplasty were 17%, 15%, and 7%, respectively. For an average height of 30 mm for the posterior border of the T12 vertebral body, these percentages result in average height increases of 5.1, 4.5, and 2.1 mm, respectively, in our cases after vertebroplasty. Hiwatashia et al (8) reported an increase in vertebral-body height after percutaneous vertebroplasty in 30 patients with osteoporosis, with changes of 2.7 mm anteriorly, 2.8 mm centrally, and 1.4 mm posteriorly. In their report and in ours, gains in the height at the anterior border and at the center of the vertebral bodies after vertebroplasty were similar to those reported by Garfin et al after kyphoplasty. In our study, the gain in the posterior wall from vertebroplasty was less than the gain the anterior wall. Hiwatashia et al reported a similar result. The mean restoration percentage in the midline vertebral height with kyphoplasty was 35% of the lost height in the report by Lieberman et al (5). Our data showed that this restoration percentage after vertebroplasty was 26.7% in all 73 vertebral bodies (Table 5). Garfin et al and Hiwatashia et al did not discuss the restoration percentage. The height of the anterior border of the fractured vertebral bodies was 83% ± 14 of the predicted height before kyphoplasty, and this was restored to 99% ± 13 of predicted height after kyphoplasty in the report by Garfin et al. In our cases, the height of the anterior border of the fractured vertebral bodies was 48% ± 18 of the normal posterior height before vertebroplasty, and this was restored to 65% ± 17 of normal posterior height after vertebroplasty. On the basis of these data, it seems that both kyphoplasty and vertebroplasty may result in similar gain in the vertebral height at the anterior border and at the center, and kyphoplasty has better height restoration percentage than percutaneous vertebroplasty did in our cases. However, the severity of the compression fracture was different in these studies, and more research in a comparable patient population is needed to address this issue.
In both the study by Garfin et al and in ours, we have seen decreased posterior vertebral-body height as a result of a fracture before the interventional procedure of kyphoplasty or vertebroplasty are performed. Therefore, we did not use this measure as an internal reference in calculating the height ratio. The decreased height of the posterior vertebral body suggests a fracture line involving the posterior border of the vertebral body. Leakage of bone cement along the fracture line to the spinal canal may occur if the fracture involves the posterior border of the vertebral body. We did not have any cases of the epidural leakage of bone cement or any sudden paraplegia with vertebroplasty so far. We believe that the following factors may improve safety in performing vertebroplasty: 1) ensuring adequate opacification of the bone cement, 2) keeping the biopsy needle from breaking the medial wall of the pedicle or from passing through the spinal canal while the needle is advanced into the vertebral body, 3) constantly monitoring the injection of bone cement by using a high-resolution biplane fluoroscopy, and 4) immediately ceasing the injection when the cement reaches the posterior one-fourth of the vertebral body.
Gas in a fractured vertebral body or “radiographically visible linear intravertebral vacuums” was considered a benign finding and pathognomonic for avascular necrosis (Kummel disease) (10, 11). Lanea et al (11) found that 32% of their 236 osteoporotic compression fractures contained clefts at the time of vertebroplasty. The investigators concluded that these clefts are more common than previously described and that they probably represent fracture non-unions. Lanea et al also found a trend toward greater pain relief in patients with clefts that were opacified at the time of vertebroplasty. McKiernan et al (9) found that 35% of vertebrae undergoing vertebroplasty had dynamic mobility in the fractured vertebral body, by comparing standing lateral views and supine cross-table lateral views. For vertebroplasty, they positioned their patients prone in extension on a four-poster frame table, with padding. They reported that the mean anterior height of the vertebral body increased from 42% to 70% of the reference normal (increase of 28%, ie, an average absolute increase of 8.4 mm). The mean vertebral-body kyphotic angle (equivalent to the wedge angle in this article) decreased 7.18° after vertebroplasty in the fractured vertebral body containing intravertebral clefts. In our study, 39 (53%) of 73 vertebral bodies treated with first vertebroplasty were found to have a gas-filled intravertebral cleft on plain radiographs obtained before vertebroplasty. For vertebral bodies containing gas, the anterior height of the vertebral body increased from 14% to 64% of the reference normal (increase of 24%, ie, average increase of 7.2 mm), and the mean wedge angle decreased 10.2° postoperatively. With vertebroplasty, the effects of wedge-angle reduction, as well as restoration of the height of the vertebral body at the anterior border and at the center, were more significant in the gas group than in the non-gas group (Tables 3–5). We think that the likelihood of opening the anterior border for correction of the wedge angle during vertebroplasty is better for the vertebral bodies containing a cavity or cleft with gas than for vertebral bodies without a cavity or cleft.
There were some difficulties in obtaining these measurements, although intraobserver reproducibility and interobserver reproducibility were satisfactory. Possible variance in the measurement results may have occurred: 1) when the posterior borders of the vertebral body were difficult to discern in patients with severe osteoporosis. (A slightly oblique body position on the lateral view and overlap of the posterior border of the vertebral body by a rib increases the difficulty.) and 2) when the borders of the vertebral body were obscured by bone cement on the postvertebroplasty radiograph. In this study, we used routine vertical-beam lateral views for measurement. Slight differences in the rotation of the patient when these spinal views were obtained before and after vertebroplasty may have caused a slight difference in the individual’s data. Most pretreatment lateral views (in 55 of 73 vertebral bodies) for measurement were acquired 3–14 days before vertebroplasty. A rapid increase in the wedge angle or a rapid reduction in the height of the fractured vertebral body might have occurred during the interval between the acquisition of the lateral radiograph for measurement and the vertebroplasty procedure. In this study, six vertebral bodies had an increase in the wedge angle (value below 0 in Fig 3) following treatment. The increase was less than 1° in four vertebral bodies and, thus, ignorable. In one patient with severe osteoporosis, the wedge angle in two vertebral bodies increased to 3.4° and 3.5°. In this patient, a vertical-beam lateral view happened to have been obtained when the patient was on the angiography table just before vertebroplasty was performed. By comparing this image and the lateral view acquired 5 days before treatment, we found a rapid change in the 5 days before vertebroplasty. On the basis of the vertical-beam lateral view obtained on the angiography table just prior to vertebroplasty on the day of vertebroplasty as a pre-vertebroplasty measurement, there was reduction in the wedge angle of 3.7° and 0.4° after vertebroplasty in these two vertebral bodies, respectively.
Severe kyphosis and a reduction in the height of the thoracic vertebral bodies occurs because of osteoporosis, and multiple vertebral fractures may reduce the pulmonary capacity, which in turn leads to an impairment of pulmonary function (6). Patients with a severe reduction in the total height of the lumbar spine may have reduced abdominal space associated with a loss of appetite (6). From this study, we observed that percutaneous vertebroplasty has effects in height restoration and wedge-angle reduction. Yet, our main application for percutaneous vertebroplasty is to alleviate back pain, as patients are usually referred to us because of severe back pain. The effects of height restoration and wedge-angle reduction are byproducts of vertebroplasty. Through these effects, it is possible to prevent future impairment in pulmonary function or future abdominal complaints resulting from severe kyphosis and shortening of the vertebral bodies.
Conclusion
Percutaneous vertebroplasty produces height restoration and the wedge-angle reduction in the fractured vertebral body, and also kyphosis-angle reduction in the affected spine. Using padding under the upper chest and pelvic region during the procedure, we obtained the following results: 1) Vertebral height was restored more at the anterior border than at the posterior border; 2) the restoration percentage of vertebral body height was greater in the anterior border than in the posterior border; and 3) the restoration percentage was highest for wedge-angle reduction, followed by height restoration at the anterior border of the vertebral body and height restoration at the center of the vertebral body. The effects of height restoration and wedge-angle reduction were more remarkable in patients with gas inside the fractured vertebral body than in those without gas inside the vertebral body, as shown on plain radiographs obtained before vertebroplasty.
Footnotes
Supported in part by Taipei VGH research grants 91–231 and 92–295 and National Science Council of the Republic of China grant NSC 91-2314-B-075-120.
References
- Received March 8, 2003.
- Accepted after revision May 5, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Increased sagittal vertical axis is associated with less effective control of acute pain following vertebroplasty
- Analysis of Related Factors on the Deformity Correction of Balloon Kyphoplasty
- In Not Only Vertebroplasty but Also Kyphoplasty, the Resolution of Vertebral Deformities Depends on Vertebral Mobility
- Significance of Dynamic Mobility in Restoring Vertebral Body Height in Vertebroplasty
- Percutaneous Balloon Kyphoplasty with the Patient under Intravenous Analgesia and Sedation: A Feasibility Study
- The Value of Dynamic Radiographs in Diagnosing Painful Vertebrae in Osteoporotic Compression Fractures
- Kyphoplasty and Vertebroplasty Produce the Same Degree of Height Restoration
- Percutaneous vertebroplasty for vertebral compression fractures with and without intravertebral clefts
- Percutaneous vertebroplasty and balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures and osteolytic tumours