
Abstract
Summary: We present a patient with advanced head and neck carcinoma and a bleeding pseudoaneurysm diagnosed by means of CT angiography; this was not apparent on conventional digital subtraction angiograms. The information provided by CT angiography facilitated rapid identification of the pseudoaneurysm and treatment with embolization. CT angiography may be helpful before embolization in cases of hemorrhage in head and neck cancer.
Catheter arteriography has been the diagnostic technique of choice for determining the sources of bleeding from head and neck cancer before endovascular embolization treatment (1–4). Over the past decade, considerable advances in CT angiography (CTA) have been achieved. Some consider CTA to rival conventional angiography in the evaluation of some vascular disorders of the brain and head and neck. We present a case of head and neck hemorrhage requiring embolization in which the CTA evaluation enabled the diagnosis. The condition may have been missed had conventional angiography been the only diagnostic examination performed.
Case Report
A 55-year-old man was transferred to our facility from an outside hospital. The patient had a history of nonresectable squamous cell carcinoma involving the right pharyngeal wall and tonsil that was previously treated with radiation therapy and chemotherapy. He received a course of palliative chemotherapy, with the last treatment administered on the day before his admission. The patient presented to the outside emergency department with massive oral bleeding, passing large blood clots per os. Blood was also passing through the nares and tracheostomy, which had been placed 1 month previously. At the outside hospital, his heart rate was 120 beats per minute, and his blood pressure was 120/76 mm Hg. Upon the patient’s arrival at our facility, his blood pressure was 101/48 mm Hg, and his heart rate was 138 beats per minute. Laboratory results obtained upon his admission included a hematocrit level of 21.5%, a prothrombin time of 14.4 seconds, a partial thromboplastin time of 29.2 seconds, and a creatinine level of 1.7 mg/dL. The patient was resuscitated with intravenous isotonic sodium chloride solution, 5 U of packed red blood cells, and 6 U of platelets. He was assessed by the otolaryngology (ENT) department, and both oral and nasal packing were inserted. The patient was referred to the interventional neuroradiology unit for angiography and embolization because of uncontrolled oral bleeding around the packing material. His past medical history included intravenous drug abuse, HIV and hepatitis C infections, and hypothyroidism. The patient’s medications upon his admission included lansoprazole, stavudine, lamivudine, indinavir, levothyroxine sodium, albuterol nebulizer, methadone, diazepam, and oxycodone and acetaminophen. On examination, he was alert, he followed commands, and his neurologic functions were intact. He was bleeding around the oral packing materials. The exact site of bleeding could not be determined by the ENT physicians because of the rapidity of hemorrhage and presence of trismus.
The patient was intubated and stabilized hemodynamically. A CT angiogram was performed by using a Lightspeed scanner (GE Medical Systems, Milwaukee, WI) during the dynamic injection of 120 mL of Ultravist 300 contrast material (Berlex, Camden, NJ) at a rate of 3.0 mL/s with a 25-second delay after the injection. CTA included the neck and skull base up through the region of the circle of Willis. CTA revealed a 14 × 6-mm irregular pseudoaneurysm (Fig 1) in an extensive soft-tissue mass centered in the region of the right tonsillar fossa fed by a small branch of the right facial artery (Fig 2). The tumor was centered in the right tonsillar fossa encasing and narrowing the right internal carotid artery and the proximal branches of the right external carotid artery.

Axial source image from the CTA examination demonstrates an enhancing pseudoaneurysm (arrowhead) in the large tumor mass (arrows) centered in the right tonsillar fossa.

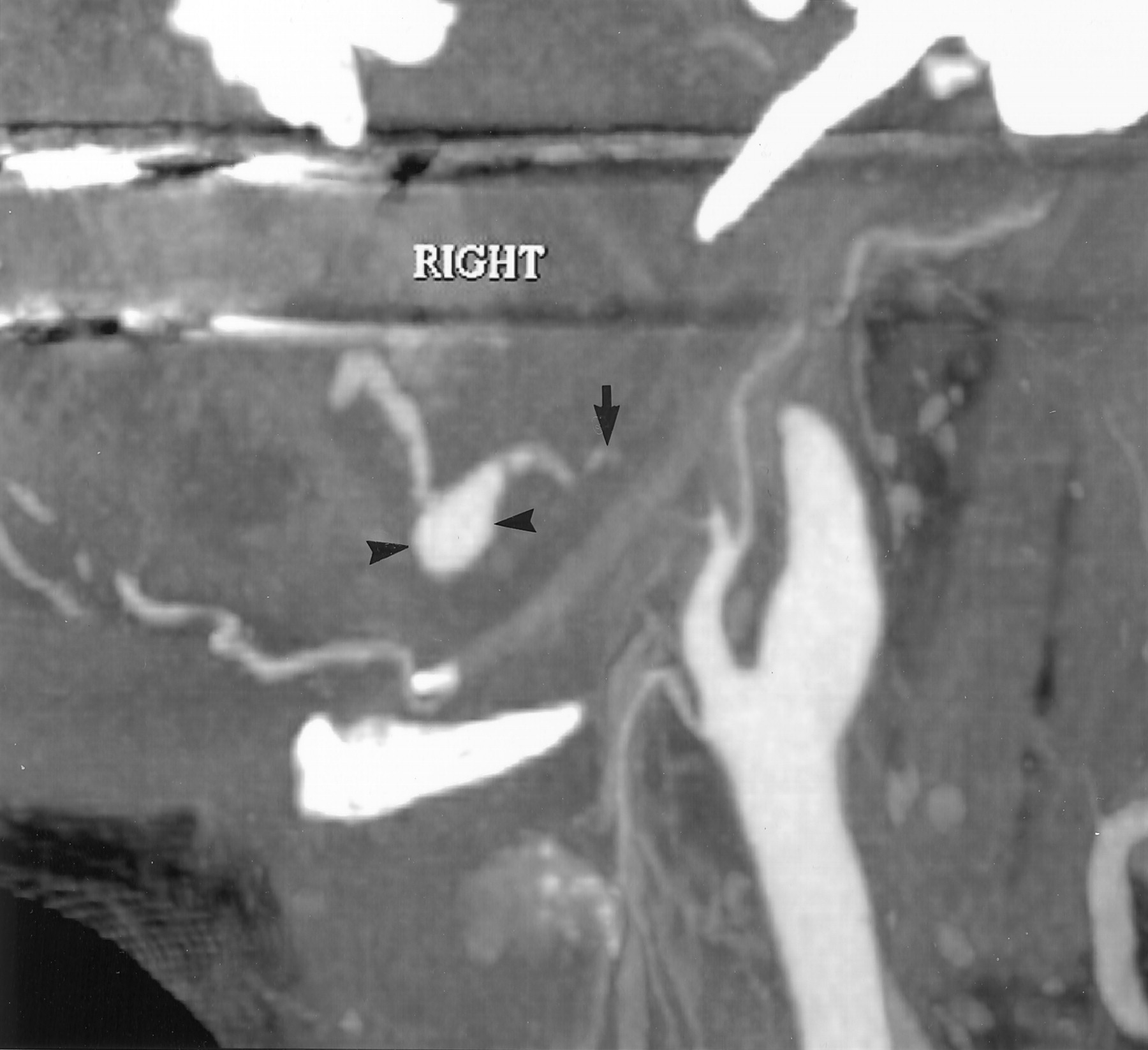
Oblique sagittal maximum intensity reconstruction image from the CTA examination demonstrates the pseudoaneurysm (arrowheads) arising off a branch of the facial artery.
The patient was taken to the interventional neuroradiology suite and placed under general anesthesia. Diagnostic digital subtraction arteriography (DSA) performed by using a 5F Envoy guide catheter (Cordis Endovascular Systems, Inc, Miami, FL) during an injection of the right common carotid artery demonstrated a narrowed and distorted right internal carotid artery. Distortion and irregularity of the right external carotid artery was demonstrated with poor filling of several branches. Selective arteriography was performed with the catheter placed at the origin of the right external carotid artery (Fig 3). This examination again demonstrated distortion of the proximal right external carotid artery and underfilling of several branches. The pseudoaneurysm seen at CTA was not identified during angiography performed with the catheter placed in the right common carotid artery or right external carotid artery origin.

Selective DSA image with the catheter tip in the origin of the right external carotid shows reflux of contrast material into a narrowed internal carotid artery (arrows) and narrowing of the external carotid branches (arrowheads). Note that the pseudoaneurysm is not visible.
A Prowler 14 (Cordis Endovascular Systems, Inc, Miami, FL) microcatheter was advanced through the guide catheter over an Agility 14 Soft microwire (Cordis Endovascular Systems, Inc), and subselective angiography of the right facial artery was performed during hand injection (Fig 4). This injection demonstrated the pseudoaneurysm previously identified on CT angiograms. The pseudoaneurysm was successfully embolized with a single 0.4-mL injection of a 33% mixture of n-butyl cyanoacrylate and ethiadol (Cordis Endovascular Systems, Inc). No procedural complications occurred.

Subselective DSA image with the microcatheter tip in a proximal facial artery branch demonstrating a pseudoaneurysm (arrow). Note the presence of subtraction artifact in the anterior aspect of the pseudoaneurysm (arrowhead).
The patient was transferred to the medical intensive care unit, and he remained in stable condition in hospital for 4 days, without evidence of recurrent hemorrhage. He was discharged home on postprocedural day 4 in stable condition and neurologically intact.
Discussion
Conventional catheter arteriography has been the technique of choice for the evaluation of patients referred for uncontrolled bleeding related to head and neck cancer, before treatment (1–4). At our institution, many of these patients had been taken directly to the interventional neuroradiology suite for diagnostic angiography and subsequent therapeutic intervention without prior vascular imaging. The lack of prior vascular imaging is often justified by the presumption that DSA provides greater sensitivity for the detection of treatable vascular causes of head and neck bleeding. Cases in which CTA has been used in the diagnosis of hepatic pseudoaneurysm before embolization have been reported (5–6) However, to our knowledge, the use of CTA in the setting of hemorrhage due to head and neck cancer has not been emphasized in the literature.
In the case presented here, the diagnosis of pseudoaneurysm was made by means of CTA, and it would likely have been missed had only DSA been performed. The information provided by CTA allowed for more rapid selection of the culprit vessel, with the microcatheter allowing successful embolization. This technique allowed a reduction in the time needed for general anesthesia and a decrease in number of vessels selected.
Why CTA was more sensitive than DSA in evaluating the pseudoaneurysm in this case is uncertain. This discrepancy could be related to a number of factors such as tumor mass and edema. CTA may offer increased sensitivity to slow-filling lesions because of the prolonged, slow injection versus the rapid, transient injection during DSA. CT may also have greater sensitivity for faint contrast medium opacification because of increased overall contrast sensitivity. The DSA study was performed after CTA; this allowed possible further accumulation of blood products in the oral cavity, which possibly resulted in increased mass effect on the pseudoaneurysm and a tamponade effect. Another possibility is that the guidewire- or catheter-induced vasospasm may have temporarily restricted flow in the vessel supplying the pseudoaneurysm during common carotid and external carotid contrast injections.
Conclusion
We suggest that CTA may be helpful in patients referred for embolization because of head neck bleeding before diagnostic angiography and intervention.
- Received June 21, 2002.
- Accepted after revision July 14, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.