
Abstract
Summary: We herein describe a case of an isolated multilocular hydatid cyst occurring in the basilar cisterns, with nondependent levels of different signal intensities shown on MR images. Three portions were visualized on T1-weighted images: the hyperintense inferior aspect, the isointense central part, and the superior aspect of lower signal intensity. The inferior portion was hypointense on T2-weighted images. This unusual appearance was caused by layering of hydatid sand and may represent a characteristic feature of hydatid disease.
Hydatid disease, an infestation by the larva of Echinococcus tapeworm, rarely affects the CNS. This disease is usually diagnosed during childhood, most commonly affecting the cerebral parenchyma.
MR imaging findings of intracranial granulosus echinococcosis have been reported to show a well-defined oval mass with signal intensities similar to those of CSF, sometimes with a hypointense rim (1–4). A pericyst may be seen as a halo of high signal intensity on T2-weighted images, and lesions typically show no contrast enhancement. When rupture, superinfection, or hemorrhage occurs in the cyst, the signal intensity may be slightly decreased on T2-weighted images and slightly increased on T1-weighted images (4). Intracranial multilocularis echinococcosis is a malignant disease, with heterogeneous enhancing lesions and extensive perifocal edema shown on MR images (5).
Case Report
A 50-year-old man presented with intense headache, of 1 week’s duration, in the cervico-occipital region. The headache was accompanied by nausea and vomiting. The patient had no history of trauma or seizures. A clinical examination revealed neck stiffness and subtle anisocoria. CT revealed a hyperattenuated mass in the anterior aspect of the medulla oblongata and lower pons (not shown). CSF examination revealed numerous WBCs, predominantly lymphocytes, and no other abnormalities.
MR imaging was performed on a 1.0-T imager, and it showed a multiloculated lesion in the premedullary cistern, ≤3 cm in diameter. On T1-weighted images, the lesion consisted of three different parts: the central one was isointense to the medulla, the superior one was of lower signal intensity, and the inferior one was hyperintense (Fig 1A–C). On T2-weighted images, the inferior portion was hypointense, whereas the rest of the mass was of high signal intensity (Fig 1D and E). The inferior area was clearly separated from the rest of the lesion, with an appearance of a nondependent level on both T1- and T2-weighted images (Fig 1A–E). The mass showed no contrast enhancement. The results of intra-arterial cerebral angiography were unremarkable.

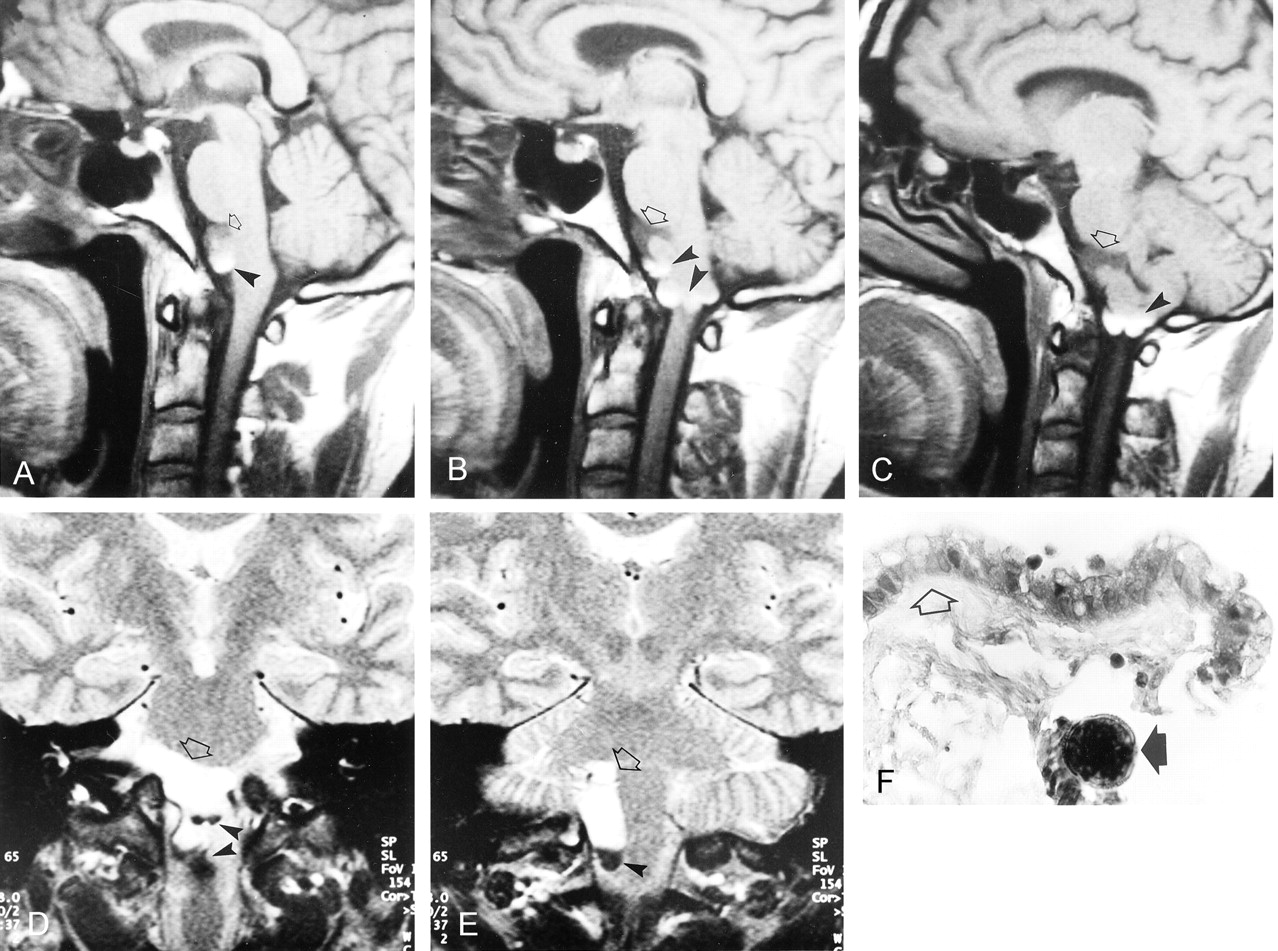
Images from the case of a 50-year-old man with cerebral hydatid disease.
A–C, Sagittal spin-echo T1-weighted MR images (584/12 [TR/TE]) show a multilocular mass in the premedullary cistern, extending from the lower pons to the C1 level. The central part of the lesion is isointense with the brain stem, whereas the superior portion is of lower signal intensity (open arrows). The inferior aspect of the mass is hyperintense, with an appearance of nondependent levels, best seen in C (arrowheads). The layering appearance is best appreciated in A.
D and E, Coronal spin-echo T2-weighted MR images (1858/80) show the lesion in the subarachnoid space, located in the midline and extending to the right (open arrows). The lesion is predominantly hyperintense compared with CSF, with low signal intensity in its inferiormost portion, which is well delineated (arrowheads). A subtle transitional zone can be seen just above this hypointense area.
F, Photomicrograph of the hydatid cyst wall shows the germinative epithelium, with ruptured daughter vesicles. A number of scolices are seen, predominantly in the vicinity of the daughter vesicles. The laminated membrane is found on the outer aspect of the germinative epithelium (Mallory; original magnification, ×400).
Surgery was performed with the patient in the sitting position, by using a far lateral suboccipital approach on the right side. A portion of the C1 transverse process was resected, accompanied by dorsal transposition of the vertebral artery and suboccipital craniotomy. When the dura was opened, a cystic lesion was found in the premedullary subarachnoid space, surrounded by a thickened arachnoid membrane. There was no evidence of hemorrhage or calcification. The entire intact cyst, containing thick, whitish material, predominantly in its inferior aspect, was dissected from the arachnoid membrane and extirpated. The postoperative course was uneventful.
Histologic findings finally provided the diagnosis, showing a typical hydatid cyst, including inner germinal layer with daughter vesicles and scolices in the lumen (Fig 1F). The pericyst was not developed, and no signs of superinfection or hemorrhage were found. Postoperative serologic tests were negative for Echinococcus, and the results of CT of the liver and lungs were unremarkable.
Discussion
Hydatid disease is a rare parasitic infestation in humans, caused by the larval stage of the cestode species Echinococcus granulosus or Echinococcus multilocularis. E. granulosus is the most frequently encountered type of hydatid disease in humans. It is prevalent in the grazing regions of the world, particularly the Mediterranean region, the Middle East, South America, Africa, Australia, and New Zealand (1). E. multilocularis is endemic in parts of the Northern hemisphere, including Russia, North America, Japan, and Europe (5). The definitive hosts of the tapeworm are usually dogs and foxes, respectively. Eggs are excreted in the feces, and ingested by intermediate hosts, such as sheep and rodents. The cycle is completed when the definitive host eats the viscera of the intermediate host. When humans become accidental intermediate hosts, the larvae penetrate the intestinal wall and spread into the circulation. The larvae may then develop into hydatid cysts in different organs, most commonly in the liver (1, 5).
The hydatid cyst has three layers: the outer pericyst, composed of inflammatory host cells and a fibrous protective zone; the acellular laminated membrane in the middle; and the inner germinal layer, also known as the germinative epithelium. The laminated membrane and the germinal layer form the true wall of the cyst, referred to as the endocyst (the laminated membrane is occasionally called ectocyst). The pericyst may not be present in all cases. Daughter vesicles are formed from rests of the germinative epithelium and resemble a bunch of grapes. The vesicles contain scolices (the larval stage of the parasite), and when they rupture, the scolices pass into the cyst fluid and form a white sediment known as hydatid sand. The cyst fluid is itself clear or pale yellow and contains proteins, lipids, and polysaccharides (1).
Intracranial granulosus echinococcosis occurs in only approximately 2% of cases of hydatid disease, typically involving the cerebral parenchyma, especially the parietal lobes, corresponding to the middle cerebral artery watershed territory (2, 3). Intracranial subarachnoid spaces are the second most common location of the disease in the CNS, although their occurrence is far less frequent (2–4, 6). Cases of cerebral aqueduct cyst (6), gigantic cyst arising from the diploë of cranial bones with intracranial extension (7), and intradural spinal hydatid cysts (8) have been reported. Vertebral involvement has been well documented (9). Cysts are usually single and may be unilocular or multilocular.
Classic CT appearance of E. granulosus intracranial hydatid disease is a spherical cystic lesion with sharply defined border and attenuation similar to that of CSF (1–3). MR imaging shows a well-defined oval or cystic mass with signal intensities similar to that of CSF, sometimes with a low intensity rim (1–4). MR imaging may also show pericyst as a halo of high signal intensity on T2-weighted images, and, in some cases, perifocal edema may be detected (2–4). The lesion typically shows no contrast enhancement, and calcifications, usually peripheral, are rare. A mild enhancement of the wall may be found (2). When a secondary process occurs in the cyst, such as infection or rupture, the signal intensity tends to be slightly decreased on T2-weighted images and a little higher on T1-weighted images (4). In one described case of a hydatid cyst, proton MR spectroscopy revealed a large succinate peak, in addition to lactate, alanine, and acetate (10, 11).
Infestation with E. multilocularis is a more malignant disease, referred to as alveolar echinococcosis. CT findings of brain involvement are typically multiple isoattenuated or hyperattenuated lesions that show contrast enhancement (5). On MR images, the lesions are heterogeneous, with areas of low signal intensity on both T1- and T2-weighted images, presumably corresponding to calcifications. Extensive perifocal edema is present, and heterogeneous contrast enhancement can be seen (5).
The lesion in our patient was of an unusual appearance on MR images, and we suspected that the areas of both T1 and T2 shortening could correspond to blood products, microcalcifications, or high protein content. The MR imaging pattern observed was not typical of any particular disease, and we put epidermoid tumor with complications at the top of our differential diagnosis list. An arachnoid cyst with secondary changes was next on our list, and infestations with parasites, primarily racemose cysticercosis and E. granulosus, were also included. We also entertained the possibility of an unusual aneurysm, because the mass was adjacent to the right vertebral artery. Apparent diffusion coefficient maps and especially proton spectroscopy could have provided additional information, but our MR imager did not have echo-planar imaging or spectroscopy capabilities.
No evidence of hemorrhage or calcifications was present, either intraoperatively or histologically, and the whitish fluid within the cyst corresponded to hydatid sand. We propose that layering of the scolices and then secondary changes within the cyst are responsible for the MR imaging findings of different levels within the lesion, which are especially well shown on T1-weighted images. This appearance has not been previously reported, and it may be characteristic for hydatid disease.
It is commonly thought that E. granulosus lesions in the CNS are typically secondary, but a number of studies have indicated that brain and vertebral involvement may more frequently be primary (9, 12). It is proposed that the high rates of secondary involvement reported previously may have been due to delayed diagnosis and insufficient treatment during the pre-CT era (12). The case we present supports this view in that no evidence of any other organ involvement was found by imaging studies or laboratory tests.
References
- Received April 24, 2002.
- Accepted after revision June 27, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.