
Article Figures & Data
Figures
- Fig 1.
Case 3.
A, Cranial sonogram obtained on day 2 of life shows a large right occipital porencephalic cyst containing echogenic clot.
B and C, Axial view unenhanced cranial CT scans obtained on day 3 of life show large porencephalic cysts within the right occipital and temporal lobes. The occipital cyst communicates with the right lateral ventricle.
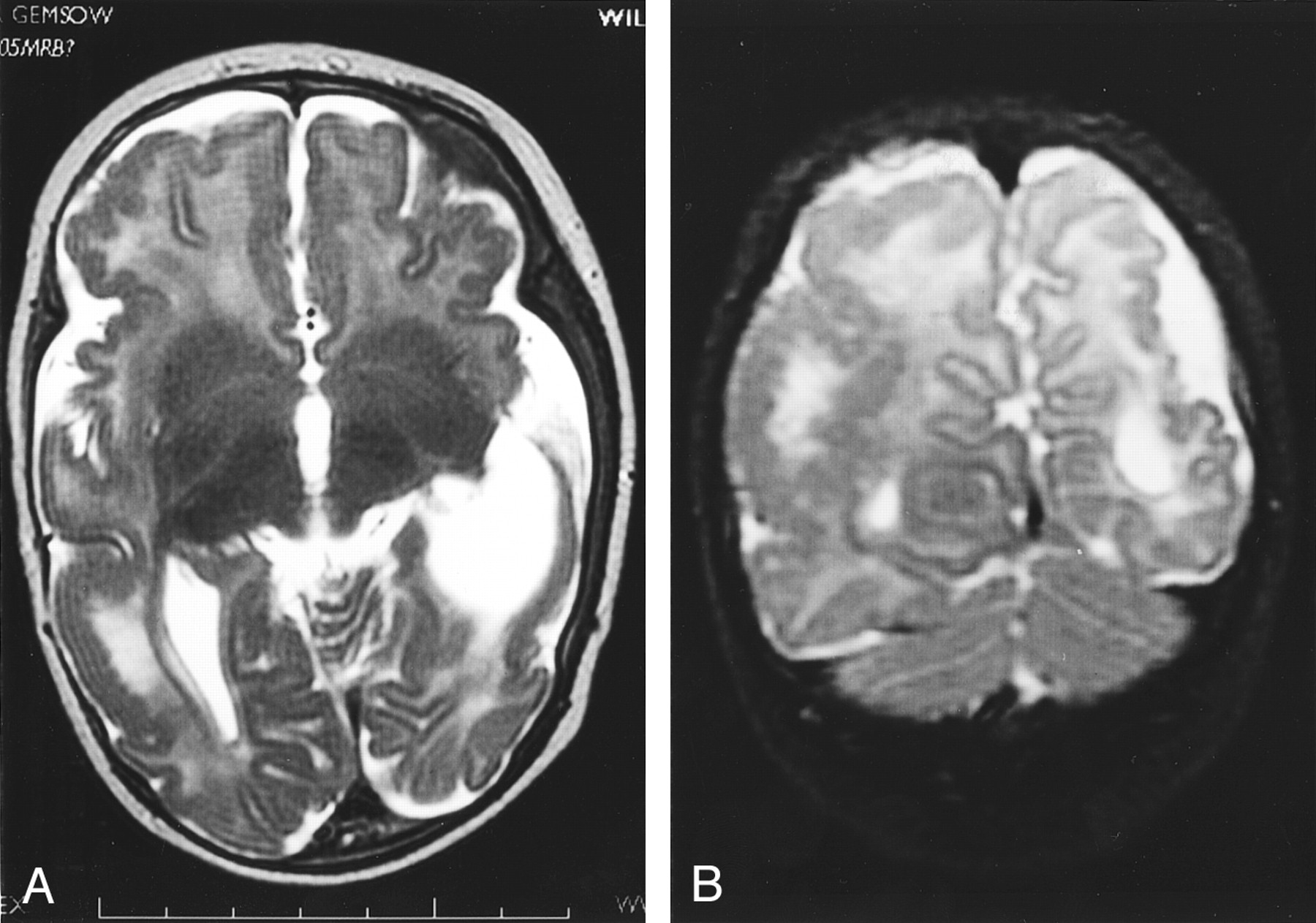
- Fig 2.
Case 1.
A, Unenhanced axial view cranial CT scan shows large right frontotemporal and left temporal porencephalic cysts with enlargement and remodeling of the middle cranial fossae.
B, Coronal view fluid-attenuated inversion recovery image (10002/147 [TR/TE]; inversion time, 2200 ms), obtained when the patient was 8 years old, shows large bilateral porencephalic cysts. There is absence of any surrounding high signal intensity gliosis. There is ex vacuo dilation of the right lateral ventricle.
C, Coronal T2-weighted image (6200/101 [TR/TE]) shows bilateral porencephalic cysts. Communication of the right cyst with the ventricular system after fenestration surgery can be seen.
- Fig 3.
Case 4.
A and B, Axial view unenhanced cranial CT scans, obtained on day 3 of life, show very large bilateral areas of porencephaly with marked loss of cerebral parenchyma. The cysts contain clots of varying ages and attenuation. Both cysts communicate with the ventricles.
- Fig 4.
Case 2.
A, Sagittal view cranial sonogram, obtained on day 3 of life, shows increased bulk and echogenicity of the choroid plexus within the lateral ventricle, compatible with choroid plexus hemorrhage, as well as ventricular dilation.
B, Unenhanced axial view cranial CT scan, obtained on day 4 of life, shows abnormal enlargement and variable attenuation of the extraaxial spaces, compatible with extraaxial hemorrhagic collections. Hyperattenuated blood can be seen along the tentorium cerebelli, compatible with more acute hemorrhage. A left temporal porencephalic cyst is also present.
C, Coronal view gradient echo image (625/14.9), obtained on day 8 of life, shows hemosiderin deposition (very low signal intensity) within the choroid plexus of both lateral ventricles, along the tentorium cerebelli, and over the cerebellar surface. Loculated, mixed signal intensity and bilateral extraaxial collections compatible with hemorrhagic collections of varying ages can be seen. The lateral ventricles are dilated.
- Fig 5.
Case 6.
A and B, Fetal MR images obtained at 21 weeks’ gestation. Axial and coronal view T2-weighted images show a large left-sided extraaxial hemorrhage of variable signal intensity, with mass effect on the underlying cerebral hemisphere.
C and D, Fetal MR images obtained at 23 weeks’ gestation. Axial and coronal view T2-weighted images (26480/100) show the mixed signal intensity extraaxial hemorrhage with more clarity. Signal intensity change within the left parietal lobe can be seen, with breech of the overlying cortex and adjacent wall of the lateral ventricle representing an area of evolving porencephaly.
E and F, Fetal MR images obtained at 33 weeks’ gestation. Axial and coronal view T2-weighted images (42597/95.7) show further evolution and resolution of the left extraaxial hemorrhage. There is left temporoparietal porencephaly with ventricular communication. High signal intensity abnormality is now noted within the white matter of the right temporal lobe.
G and H, Cranial MR images obtained when the patient was 5 months of age. Axial and coronal view T2-weighted images (3420/168) show left temporoparietal porencephaly with ventricular communication and loss of cerebral substance. Ventriculomegaly can be seen. Persisting signal intensity abnormality can be seen within the white matter of the right temporal and parietal lobes. A new finding is of a neuronal migrational disorder with extensive polymicrogyria and areas of bandlike heterotopia with an almost “double cortex” appearance.
- Fig 6.
Case 6.
A and B, Axial and coronal view T2-weighted images (3420/168), obtained when the patient was 5 months of age, show left parietal and temporal porencephaly in association with a neuronal migrational disorder with extensive areas of polymicrogyria.






Tables
- TABLE 1:
Summary of clinical details for patients with neonatal alloimmune thrombocytopenia
Case Sex Gestation at Delivery Mode of Delivery Platelet Count(Cord Blood Sample)Normal = 150–400 × 109 Early Clinical Features 1 F 41 /40 SVD 12 × 109 Generalized petechiae, bruising 2 F 38 /40 Elective LUSCS 12 × 109 Generalized petechiae, purpura 3 F 37 /40 SVD 13 × 109 Generalized petechiae, bruising 4 M 38 /40 Emergency LUSCS 20 × 109 Bruising, large head circumference, intraretinal hemorrhages, small optic discs 5 M 40 /40 Forceps 28 × 109 Generalized petechiae 6 F 33 /40 Elective LUSCS 83 × 109 (Antenatal) Microcephaly, seizures Note.—F indicates female; M, male; SVD, spontaneous vaginal delivery; LUSCS, lower uterine segment caesarian section.
Case No. Imaging Modality and Age Imaging Findings Clinical Outcome 1 US, 1 mo Large left temporal and right frontotemporal porencephalic cysts Seizures, cerebral palsy, left hemiplegia, developmental delay, microcephaly CT, 1–6 yr Bilateral porencephalic cysts, right lateral ventricular enlargement MR imaging, 8 yr Multilocular left temporal porencephalic cyst, right frontotemporal porencephaly with ventricular communication (after fenestration surgery), right lateral ventricular enlargement 2 US, days 1 and 3 Bilateral choroid plexus hemorrhages, thick echogenic extraaxial spaces, left temporal porencephalic cyst with ventricular communication, ventriculomegaly Seizures, developmental delay CT, day 4 Choroid plexus hemorrhages, acute on chronic bilateral extraaxial hemorrhages, left temporal porencephaly MR imaging, day 8 Choroid plexus hemorrhages (hemosiderin), hemosiderin over cerebellar sulci, mixed signal loculated extraaxial collections, left temporal porencephalic cyst with ventricular communication, lateral ventriculomegaly with colpocephaly 3 US, day 2 Large right temporal porencephalic cyst with clot, right occipital lobe porencephalic cyst with clot communicating with lateral ventricle Seizures, developmental delay, microcephaly CT, day 3 Right-sided porencephalic cysts with clot, small acute parenchymal hemorrhage in right frontal white matter, dilated right lateral ventricle 4 US, day 3 Large left frontotemporal porencephalic cyst with clot communicating with lateral ventricle, large right parietotemporal and occipital porencephalic cyst with clot and ventricular communication, ventriculomegaly (colpocephaly) Died during neonatal period CT, day 3 Bilateral large porencephalic cysts with clot and ventricular communication, ventriculomegaly 5 CT, 4 mo Large right occipitotemporal porencephalic cyst communicating with right lateral ventricle, mild right lateral ventricular dilatation Seizures, blindness, developmental delay MR imaging, 2 yr Large right temporal porencephalic cyst with ventricular communication, ventriculoperitoneal shunt, reduced periventricular/periatrial white matter with increased fluid-attenuated inversion recovery/T2 signal (gliosis) 6 Fetal MR imaging, 21/40 Left extraaxial hemorrhage with mass effect, signal change left parietal lobe with cortical breech, porencephaly? Microcephaly, seizures Resolving extraaxial hemorrhage, extensive parietotemporal porencephaly with hemosiderin lining cyst, ex vacuo dilation right lateral ventricle, high signal right temporal lobe, delayed maturation with delayed sulcation MR imaging, 5 mo Left parietotemporal porencephaly, ventriculomegaly, neuronal migrational disorder with extensive polymicrogyria and periventricular heterotopia with almost double cortex appearance, abnormal signal right temporal and parietal white matter





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}