
Article Figures & Data
Figures
- Fig 1.
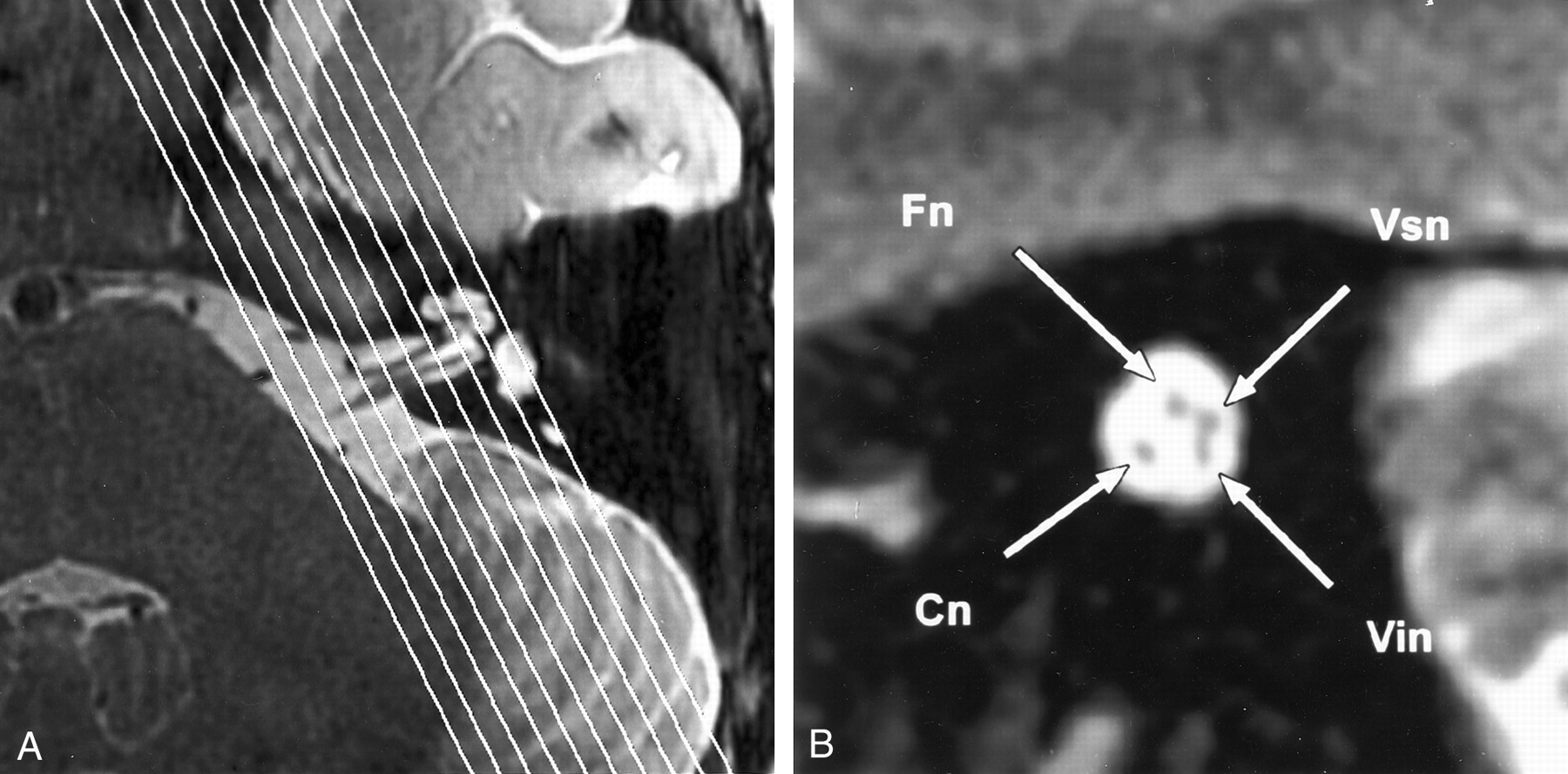
High-resolution T2-weighted fast spin-echo MR images provide excellent depiction of the cisternal and intracanalicular segments of the facial nerve and the three divisions of the vestibulocochlear nerve.
A, Axial view of the left cerebellopontine angle and IAC shows the normal anatomy. Parallel lines illustrate the plane prescribed for oblique plane sagittal images obtained perpendicular to the nerves of the IAC.
B, Oblique plane sagittal image obtained at the fundus of the IAC, oriented with anterior to the left and the cerebellum to the right. High-signal-intensity CSF delineates the four nerves of the IAC. In the anterior aspect of the canal, the facial nerve (Fn) lies superiorly, with the cochlear nerve (Cn) inferior to it. Superior (Vsn) and inferior (Vin) vestibular nerves lie posteriorly.
- Fig 2.
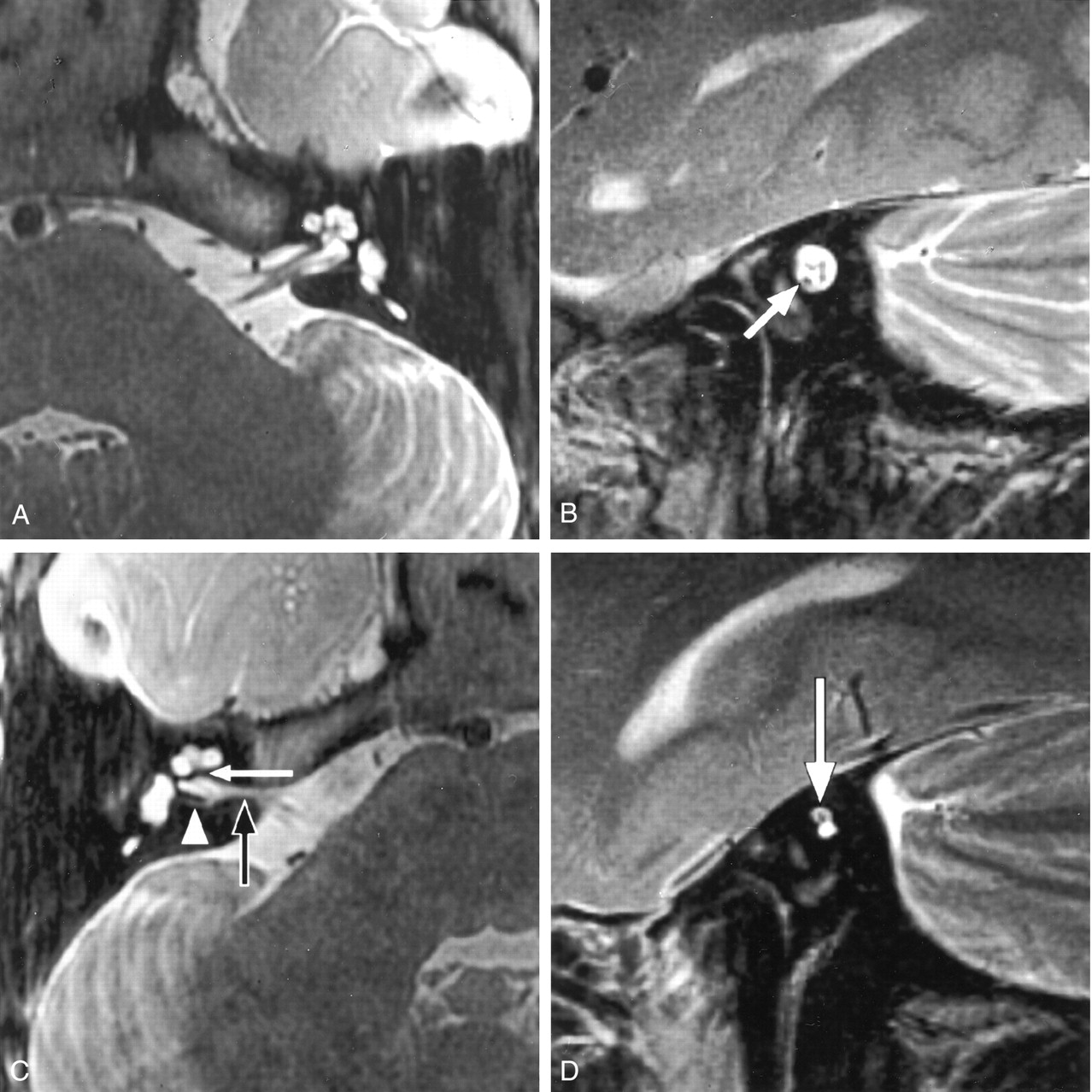
Congenital absence of the cochlear nerve with an isolated cochlea. Axial and oblique sagittal T2-weighted fast spin-echo MR images of a 5-year-old girl with profound unilateral hearing loss (patient C8).
A, Image of the normal left side shows the normal contours of the cochlea and other labyrinthine structures.
B, IAC is of normal size and contains four nerves of comparative size. Cochlear nerve lies anteroinferiorly (arrow).
C, Right side shows a deformed contour of the IAC (black arrow). Low-signal-intensity bar separates the fundus of the IAC from the modiolus (white arrow), which was confirmed to be bony at CT. We describe this as an isolated cochlea. The arrowhead indicates a singular canal containing the nerve of the posterior semicircular canal.
D, Oblique sagittal image of the distal IAC shows a solitary nerve within the superior aspect of the small, deformed canal (arrow). The cochlear nerve is absent in this patient with normal facial nerve function.
- Fig 3.
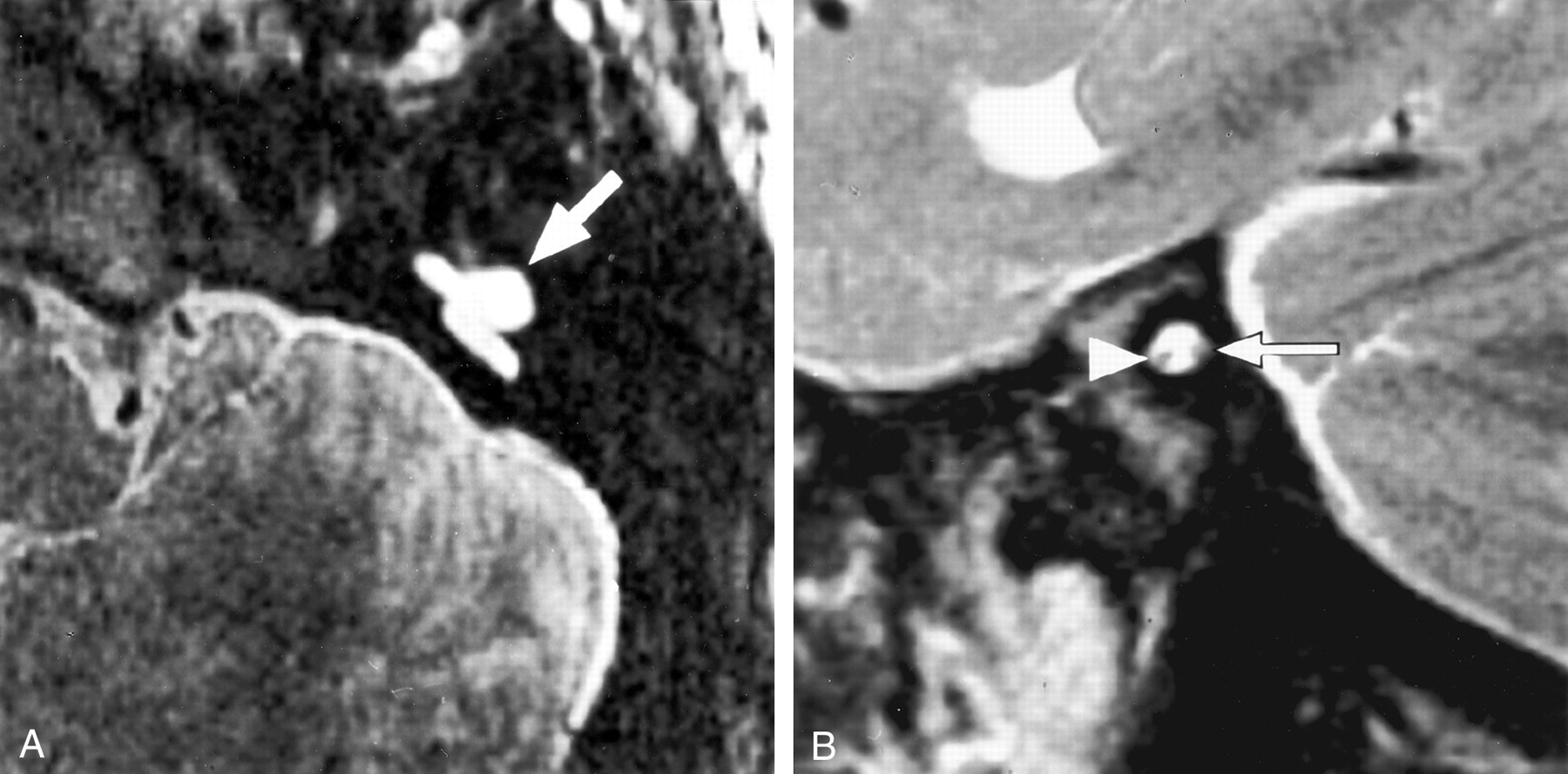
Bilateral cochlear nerve absence in a 7-year-old patient with severe dysplasia and bilateral absence of the cochlea (patient C10). Facial nerve function was preserved.
A, Axial T2-weighted fast spin-echo MR image of the left side shows dysplasia of the vestibule and semicircular canals (arrow). Cochlea was absent.
B, Oblique sagittal MR image obtained on the same side shows a small IAC containing only two nerves. The intact facial nerve lies anteriorly (arrowhead). We suspected that the posterior nerve was vestibular, on the basis of its position and the absence of cochlear structures (arrow).
- Fig 4.
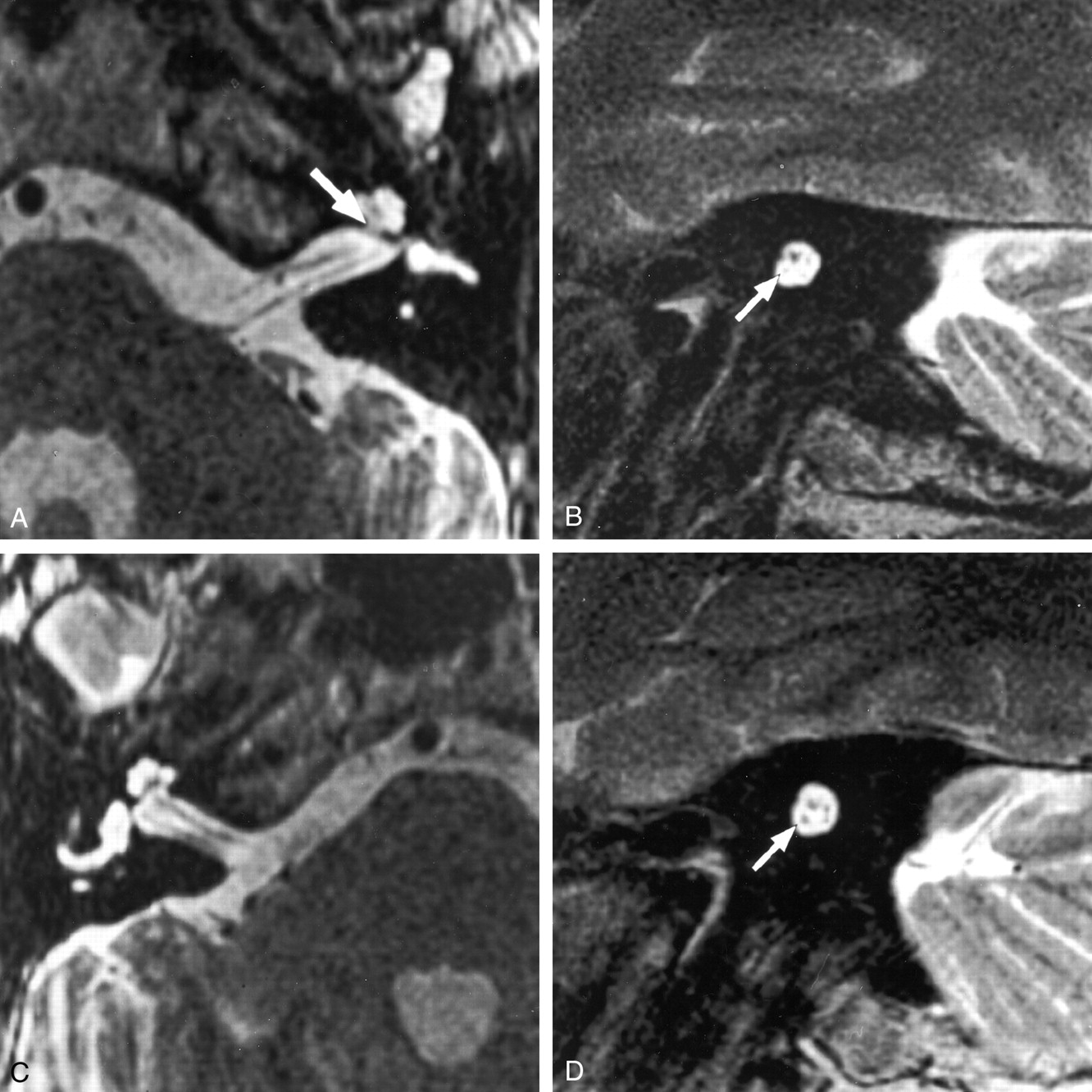
Deficient cochlear nerve in a 60-year-old patient with a 50-year history of left hearing loss after a motor vehicle accident (patient A10). This patient presented with a 3-month history of right-sided hearing loss.
A, Axial T2-weighted fast spin-echo MR image shows a small left modiolus (arrow) but no other structural cochlear abnormalities.
B, Corresponding oblique sagittal image shows a small caliber cochlear nerve (arrow) in a normal-sized IAC.
C, Axial T2-weighted fast spin-echo MR image of the right side shows no abnormality to explain the recent hearing loss.
D, Oblique sagittal T2-weighted fast spin-echo MR image of the right side also shows no abnormality to explain the recent hearing loss. A normal-caliber cochlear nerve is seen (arrow). Cochlear implantation was successfully performed on this side.
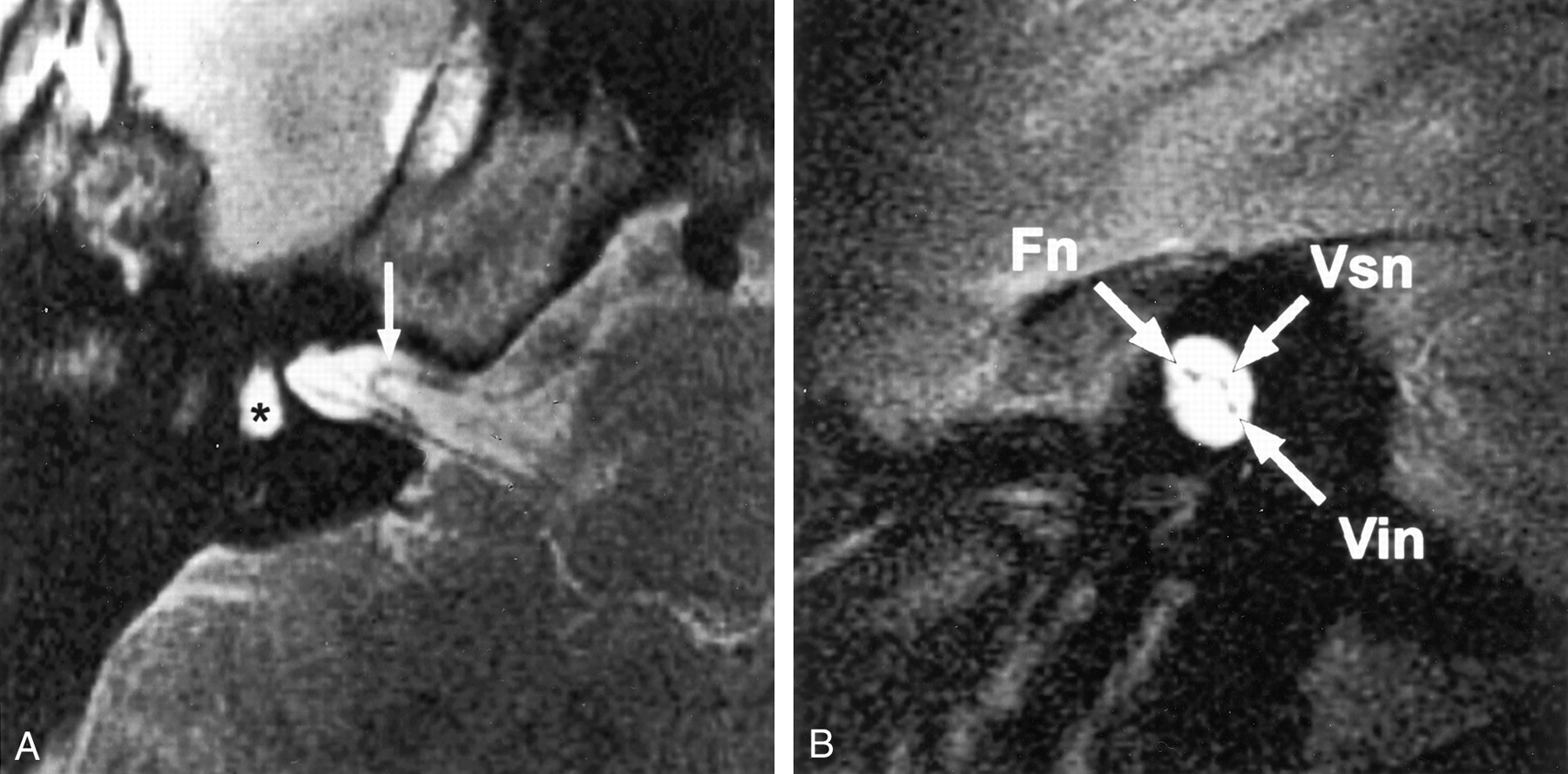
- Fig 5.
Acquired cochlear nerve deficiency in a 14-year-old patient with hearing loss after meningococcal meningitis at the age of 6 months (patient A3). Bilateral labyrinthitis ossificans was shown by CT (not shown).
A, Axial T2-weighted fast spin-echo MR image of the right side shows loss of the normal high-signal-intensity CSF in the labyrinth. The asterisk indicates the vestibule; arrow, arterior inferior cerebellar artery (AICA) loop.
B, Corresponding oblique sagittal image shows three nerves in the IAC. The cochlear nerve cannot be identified. Note the normal size of the IAC in this acquired cochlear nerve deficiency. Fn indicates the facial nerve; Vsn, superior vestibular nerve; and Vin, inferior vestibular nerve.
- Fig 6.
Acquired left-sided hearing loss of unknown etiology in patient A6. Axial high-resolution MR images showed a small left modiolus but no other labyrinthine abnormality (not shown). Cn indicates cochlear nerve; Fn indicates facial nerve; Vin, inferior vestibular nerve; and Vsn, superior vestibular nerve.
A, Right oblique sagittal T2-weighted fast spin-echo MR image clearly shows four normally sized nerves in the IAC.
B, On the affected left side, the cochlear nerve is not identified. Note the normal size of the IAC, which indicates an acquired abnormality after in utero formation of the canal.






Tables
Patient Age (y)/ Sex Significant MH History (R/L) Audiology (R/L) MR IAC Size MR Findings, Inner Ear and Nerves C1 4/M Hirschprung syndrome NAD/HL of unknown duration NAD/no response L small/R NAD R NAD/L modiolar deficiency, no L VIII n, clumped vestibular n C2 8/M Premature birth, cleft lip and palate NAD/HL of unknown duration NAD/severe profound mixed HL L small/R NAD R NAD/L modiolar deficiency, no L VIII n C3 44/M Negative Long-standing HL/progressive HL Audiology not available R small/L NAD R EELDS, modiolar deficiency, no R VIII n/L NAD C4 3/M CHARGE syndrome Bilateral HL since birth Profound bilateral SNHL Bilateral small Bilateral severe cochleovestibular dysplasia, no R or L VIII n C5 5/F Meconium intussusception Bilateral HL since birth Profound bilateral SNHL Bilateral small Bilateral severe cochleovestibular dysplasia, no R or L VIII n C6 4/M Marked developmental delay, lactic acidosis Bilateral HL at age 9 months Could not perform Bilateral small Bilateral dysplastic cochlea, bilateral small clumped VIII n C7 47/F Scarlet fever as a child Bilateral HL at age 3 y No response/profound SNHL Bilateral NAD Bilateral EELDS with modiolar deficiency, bilateral small VIII n C8 5/F Negative Long-standing HL/NAD Profound SNHL/NAD R small/L NAD R “isolated” cochlea, no R VIII n/L NAD C9 3/F In utero CVA, motor and developmental delay Bilateral progressive HL No response bilaterally Bilateral small Bilateral modiolar deficiency, no R or L VIII n C10 6/F Negative Bilateral HL since birth No response bilaterally Bilateral small Bilateral severe dysplasia with no cochlea, no R or L VIII n C11 12/F In utero toxoplasmosis exposure NAD/HL (at age 5 y) NAD/moderate profound SNHL L small/R NAD R NAD/L modiolar deficiency, no L VIII n C12 8/M Negative HL since birth/NAD Profound SNHL/NAD R small/L NAD R isolated, modiolar deficiency, no R VIII n or Vinf/L NAD Note.—MH indicates medical history; CVA, cerebrovascular accident; R, right; L, left; NAD, no abnormality detected; HL, hearing loss; SNHL, sensorineural hearing loss; IAC, internal auditory canal; VIII n, cochlear nerve; n, nerve; EELDS, enlarged endolymphatic duct and sac; Vinf, inferior vestibular nerve.
Patient Age (y)/ Sex Significant MH History (R/L) Audiology (R/L) MR Findings A1 63 /M Hypertension HL for 2 mo/HL for 3.5 y Moderate SNHL/moderate–severe SNHL R NAD/abnormal L modiolar signal, small L VIII n A2 68 /M Negative HL for 2 y/3 mo progressive HL Moderate–severe SNHL/mild SNHL R small modolus, small R VIII n/L NAD A3 14 /F Meningitis at age 6 mo Bilateral HL post-meningitis No response bilaterally Bilateral labyrinthitis ossificans, no R VIII n/small L VIII n A4 7 /F Negative HL of unknown duration/NAD Severe SNHL/NAD R mural labyrinthitis ossificans, small R VIII n/L NAD A5 45 /M Negative HL at age 21 y/progressive HL since age 21 y Moderate–severe SNHL/severe high tone SNHL No R VIII n, small R vestibular nerves/L NAD A6 6 /M Negative NAD/HL since age 3 y NAD/severe high tone SNHL R NAD/deficient L modiolus, no L VIII n A7 78 /M Negative No loss noted/HL for 3–4 y Mild–moderate SNHL/moderate–severe SNHL R NAD/large L schwannoma, small L VIII n A8 40 /F Negative HL for 2 y/NAD Moderate SNHL/NAD R 3.5-cm schwannoma, very small R VIII n/L NAD A9 9 /M Negative NAD/HL since age 7 y, stable NAD/mild SNHL R NAD/L small cochlea, modiolar deficiency, small L VIII n A10 60 /M MVA at age 10 y HL for 3 mo/HL after MVA Severe–profound SNHL/no response R NAD/L deficient modiolus, small L VIII n Note.—MH indicates medical history; MVA, motor vehicle accident; R, right; L, left; HL, hearing loss; NAD, no abnormality detected; SNHL, sensorineural hearing loss; VIII n, cochlear nerve.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Whether A Positive Response at approximately 4.5 ms in Auditory Brainstem Response Signifies Cochlear Nerve Deficiency in Infants?
- MRI Evaluation of the Normal and Abnormal Endolymphatic Duct in the Pediatric Population: A Comparison with High-Resolution CT
- Unilateral facial nerve hypoplasia without evident facial palsy
- Comparison of a Photon-Counting-Detector CT with an Energy-Integrating-Detector CT for Temporal Bone Imaging: A Cadaveric Study
- Evaluation of the Normal Cochlear Second Interscalar Ridge Angle and Depth on 3D T2-Weighted Images: A Tool for the Diagnosis of Scala Communis and Incomplete Partition Type II
- Vestibular Aqueduct Measurements in the 45{degrees} Oblique (Pöschl) Plane
- Mutations in apoptosis-inducing factor cause X-linked recessive auditory neuropathy spectrum disorder
- Pediatric Sensorineural Hearing Loss, Part 1: Practical Aspects for Neuroradiologists
- Brain Stem and Inner Ear Abnormalities in Children with Auditory Neuropathy Spectrum Disorder and Cochlear Nerve Deficiency
- Vertigo and Hearing Loss
- Complete Labyrinthine Aplasia: Clinical and Radiologic Findings with Review of the Literature