
Article Figures & Data
Figures
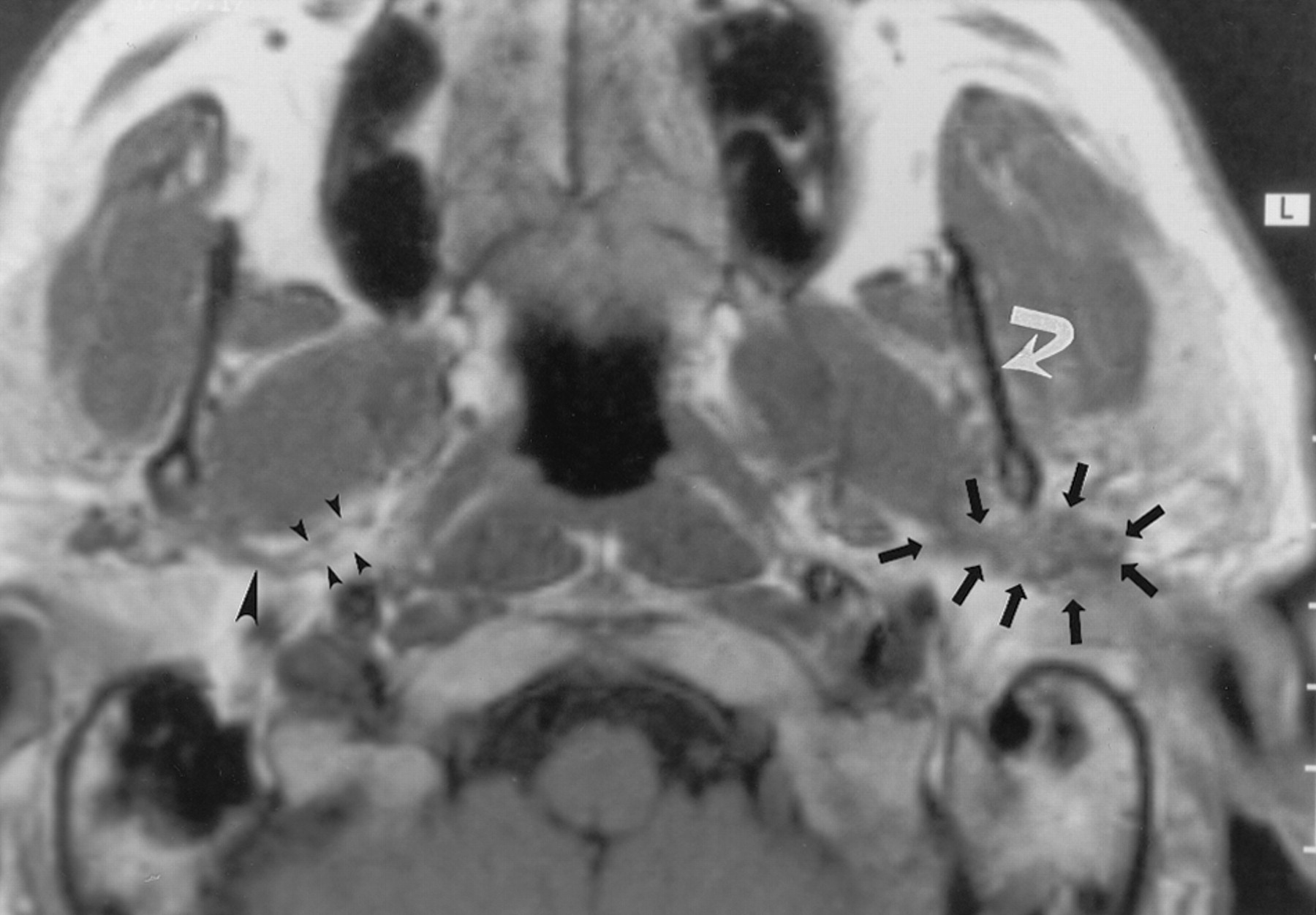
- Fig 1.
Axial nonenhanced T1-weighted MR image (700/10 [TR/TE]) obtained in a 50-year-old man with mucoepidermoid carcinoma of the parotid gland, a mass posterior to the left mandible, and no symptoms of TMJ dysfunction or neurologic signs related to V3 or the facial nerve. The image demonstrates a soft-tissue mass (straight arrows) posterior to the left mandibular ramus (curved arrow) that extends along the expected course of the left auriculotemporal nerve. MR examination revealed no signs of V3 or facial nerve involvement. These findings were interpreted as suggesting isolated perineural tumor spread along the auriculotemporal nerve; this was confirmed at pathologic examination. Note the normal appearance of the auriculotemporal nerve on the right side, with its two rootlets (small arrowheads) and trunk (large arrowhead).
- Fig 2.
Axial images obtained in a 55-year-old man with squamous cell carcinoma of the left temporal region, who had pain and swelling in the preauricular region, as well as facial nerve weakness.
A, Contrast-enhanced CT scan shows an infiltrating mass (m) in the left parotid gland that extends medially (★) between the ramus of the mandible (R) and mastoid tip (t) into the parapharyngeal space, along the expected course of the auriculotemporal nerve. Note the asymmetry in the parapharyngeal fat plane when compared with the right side. The tumor extends within the parapharyngeal space (arrowheads) anteriorly and superiorly to involve V3 (not shown). In addition, the tumor extends along the medial margin of the mandibular ramus to infiltrate the masticator space (curved arrow). Note the preserved fat plane (straight arrow) on the right side. The scan does not show the degree of invasion of the lateral pteryoid muscle.
B, Nonenhanced T1-weighted MR image (500/11) shows the same findings as in A at a slightly lower level. Note the differences in signal intensity in the parapharyngeal fat planes (★). The left parapharyngeal fat plane has slightly lower signal intensity than that of the right; this is a sign of tumor involvement (arrowheads). The fat plane medial to the ramus of the mandible on the left is completely obliterated (solid arrows), compared with that of the right (open arrow); this is a sign of tumor extension into the masticator space. Also note the slightly increased signal intensity of the lateral pterygoid muscle (P), compared with that of the right; this is consistent with involvement by tumor.
C, Contrast-agent–enhanced T1-weighted MR image (500/11) obtained with same parameters and at the same level as in B shows no substantial asymmetry in the retromandibular regions (arrows) and parapharyngeal spaces (★). The fat plane medial to the ramus of the mandible (black arrowheads) seems to be intact, when compared with that on the right (white arrowhead). Without the nonenhanced T1-weighted MR images, the full extent of the tumor would have been undiagnosed.
- Fig 3.
Axial contrast-agent–enhanced CT images obtained at two levels in a 77-year-old man with metastatic undifferentiated carcinoma and lymphoma who had a left facial mass and facial weakness.
A, Scan shows that a homogeneous soft-tissue mass (m), which extends medially (arrowheads) along the posterior margin of the ramus (★) of the mandible, almost completely replaces the left parotid gland. This finding was interpreted as suggesting perineural tumor spread along the facial nerve main trunk and auriculotemporal nerve. Pathologic findings, however, did not confirm this. Retrospective review of the CT scans revealed that the soft-tissue mass actually was lower than the expected course of the auriculotemporal nerve.
B, Scan illustrates the correct level of the auriculotemporal nerve. No abnormality in the retromandibular region is depicted at this level. ★ indicates the posterior margin of the mandibular ramus.
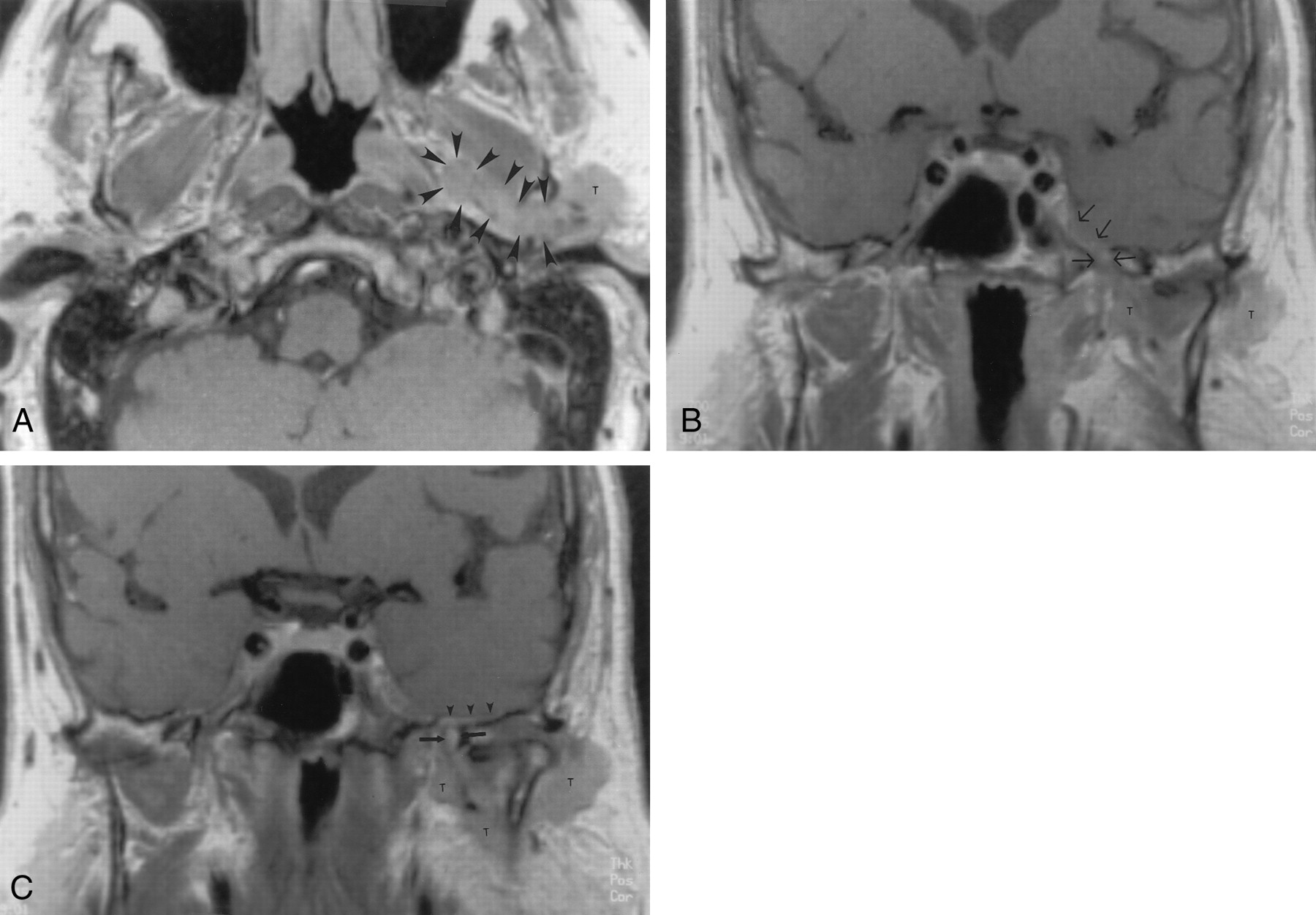
- Fig 4.
Contrast-agent–enhanced T1-weighted MR images (700/15) obtained in a 71-year-old man with skin cancer, who had TMJ tenderness and discomfort in the left ear. Symptoms related to V3 developed 8 months later.
A, Axial image shows a parotid gland mass (T) that extends medially along the expected course of the auriculotemporal nerve (arrowheads) into the parapharyngeal space.
B and C, Coronal images show the superior extension of the tumor along V3 (arrows in B) and middle meningeal artery (arrows in C) to involve the intracranial structures. Subtle dural enhancement is seen along the floor of the temporal fossa on the left (arrowheads in C). Note the normal appearance of V3 on the right. T indicates tumor. Image in C is slightly posterior to the image in B.
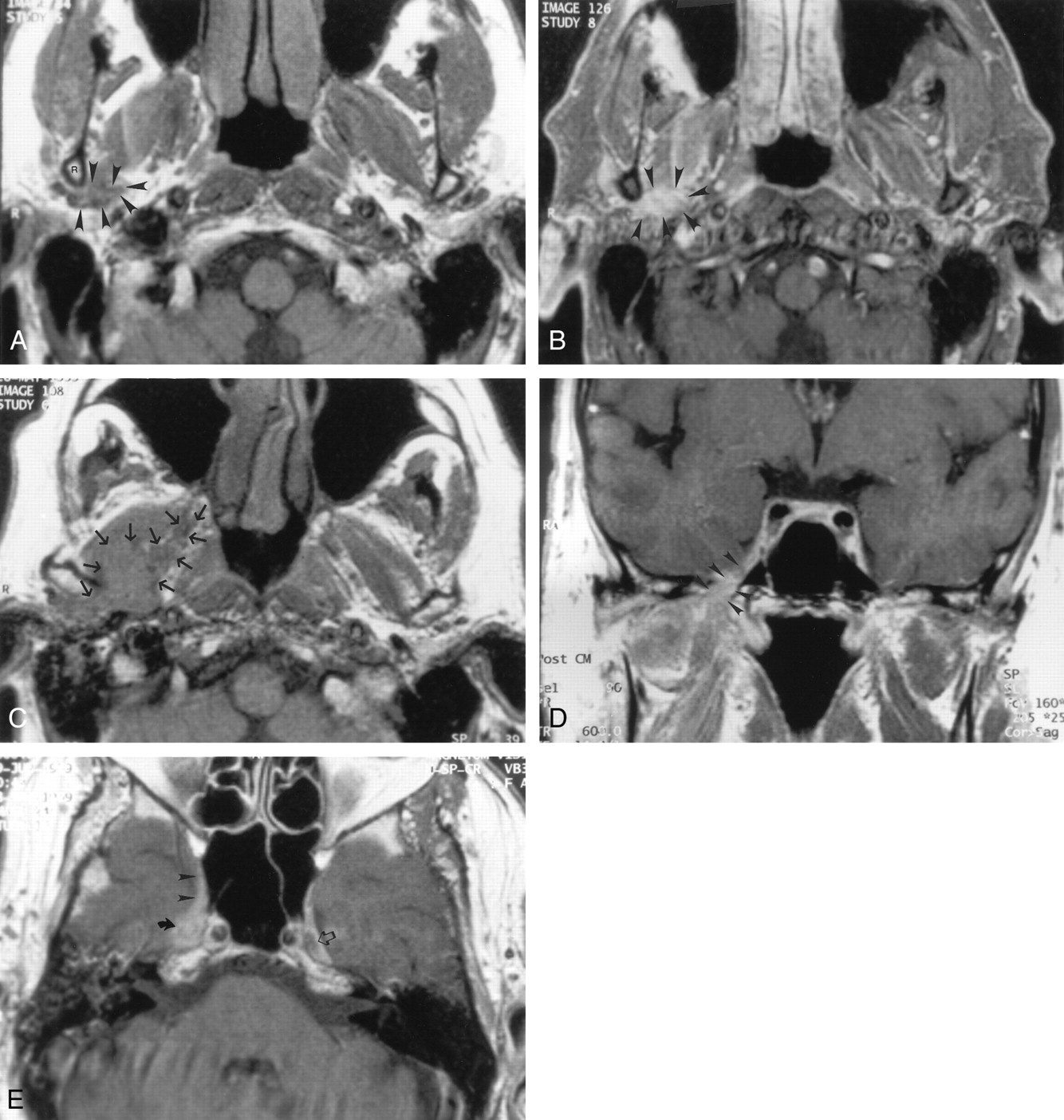
- Fig 5.
MR images obtained in a 70-year-old man with skin cancer who had progressive right facial nerve weakness. Cross-sectional CT (not shown) and MR imaging were performed to evaluate the patient’s facial weakness and preauricular pain.
A, Axial nonenhanced T1-weighted image (600/14) shows a subtle area of soft tissue (arrowheads) posterior and medial to the ramus of the mandible (R) on the right side that is abnormal when compared with the left.
B, Gadolinium-enhanced fat-suppressed T1-weighted image (500/14) obtained at the same level as in A shows marked enhancement of the area of abnormal soft tissue (arrowheads) in A. This finding was interpreted as normal at an outside institution.
C, Repeat nonenhanced T1-weighted image (600/14) obtained 12 months after the first MR examination shows the extensive progression of the tumor (arrows), with now obvious infiltration of the parapharyngeal space on the right.
D and E, Coronal (D) and axial (E) contrast-agent–enhanced T1-weighted images (600/14) show the growth of the tumor along V3 (arrowheads in D) into the Meckle cave (solid arrow in E) and cavernous sinus (arrowheads in E). Note the normal appearance of the Meckle cave on the left side (open arrow in E).
- Fig 6.
Drawings depict the relationship between the mandibular division of the trigeminal nerve (V), auriculotemporal nerve, facial nerve, and the maxillary artery (ma) and its branches. The auriculotemporal nerve arises from V3 from two roots (thin arrows). The middle meningeal artery (thick arrow) courses between the two rootlets, which coalesce, just posterior to the artery, to form a short trunk (★ in B). The trunk forms multiple branches with the anterior and posterior communicating rami (arrowheads), joining the facial nerve (★) within the parotid gland.
A, Coronal projection. aa indicates the anterior auricular nerve; iam, inferior nerve to the external acoustic meatus; sam, superior nerve to the external acoustic meatus; sta, superficial temporal artery; and str, superficial temporal ramus.
B, Axial projection. R indicates the mandibular ramus.
- Fig 7.
Drawing illustrates the relationship between V3 (V), the auriculotemporal nerve, the facial nerve (•), and the maxillary artery (thick solid arrow) and its branches to the adjacent musculature and bony structures. Thin solid arrows indicate the roots of the auriculotemporal nerve; open arrow, superficial temporal artery; arrowheads, anterior and posterior communicating rami of the auriculotemporal nerve; B, buccinator muscle; m, mandible; S, sternocleidomastoid muscle; T, temporalis muscle; z, partially removed zygomatic arch; and +, trunk of the auriculotemporal nerve.







Tables
- TABLE 1:
Patients with pathologically proven perineural tumor spread along the auriculotemporal nerve
Patient No. Diagnosis Cranial Nerve Palsy Symptoms Involvement Additional Imaging Findings Facial Nerve Main Trunk Auriculotemporal Nerve Cranial Nerve V Skull Base Intracranial 1 Poorly differentiated adenoid cystic carcinoma VII palsy at presentation, V3 palsy 10 mo later Otalgia Yes Yes Suspected No No None 2 Moderately differentiated squamous cell carcinoma VII palsy at presentation Face swelling, preauricular pain Yes Yes Yes No No None 3 Adenoid cystic carcinoma VII palsy for 2 y, pain in V3 distribution for 1 y Periauricular pain for 1 y Yes Yes Yes Unknown Unknown None 4 Unknown Right VII palsy at presentation Preauricular swelling Yes Yes Yes No No Involvement of infratemporal fossa 5 Well-differentiated squamous cell carcinoma VII palsy at presentation Preauricular pain and swelling Yes Yes Yes Yes, 16 mo after initial diagnosis Yes, 16 mo after initial diagnosis Involvement of infratemporal fossa 6 Malignant schwannoma VII palsy at presentation, V2 palsy for 16 y Intermittent diplopia Yes Yes Yes No Yes Involvement of V2 7 Mucoepidermoid carcinoma VII palsy at presentation Mass posterior to left jaw No Yes No No No None - TABLE 2:
Patients perineural tumor spread along the auriculotemporal nerve, as determined with imaging findings
Patient No. Diagnosis Cranial Nerve Palsy Symptoms Involvement Additional Imaging Findings Facial Nerve Main Trunk Auriculotemporal Nerve Cranial Nerve V Skull Base Intracranial 1 Poorly differentiated adenocarcinoma VII palsy at presentation Facial weakness Yes Yes Yes Temporal bone along the facial canal No None 2 Squamous cell carcinoma VII palsy at presentation, V3 3 mo later Pretragal mass Yes Yes Yes No Yes, 7 m after initial diagnosis None 3 Poorly differentiated squamous cell carcinoma Clinically suspected auriculotemporal nerve dysfunction, V3 palsy 10 mo later Ear discomfort, TMJ tenderness Yes Yes Yes At the foramen spinosum and ovale No Spread along the middle meningeal artery 4 Poorly differentiated adenocarcinoma VII and V palsy, clinically suspected auriculotemporal nerve dysfunction Retromandibular and pretragal pain Yes Yes Yes At the right foramen ovale Yes, 14 mo after initial diagnosis Involvement of infratemporal fossa 5 Neurofibroma V3 palsy at presentation Pain and mass in the right mandibular region No Yes Yes No No None 6 Moderately differentiated squamous cell carcinoma Bilateral V, right VI, and IX palsy Ear pain, TMJ dysfunction No Yes Yes Yes Yes Involvement of infratemporal fossa 7 Squamous cell carcinoma VII palsy for 22 mo Parotid pain and swelling, preauricular pain Yes Yes No No Yes Involvement of V1
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Secondary Otalgia: Referred Pain Pathways and Pathologies
- An Imagers Guide to Perineural Tumor Spread in Head and Neck Cancers: Radiologic Footprints on 18F-FDG PET, with CT and MRI Correlates
- Visualization of the Peripheral Branches of the Mandibular Division of the Trigeminal Nerve on 3D Double-Echo Steady-State with Water Excitation Sequence
- Perineural Spread of Malignant Melanoma of the Head and Neck: Clinical and Imaging Features
- Detection of Perineural Spread: Fat Suppression versus No Fat Suppression