
Article Figures & Data
Figures
- fig 1.
Patient 2, a 7-year-old girl with a 2-year history of 20 to 30 focal partial motor and sensory seizures a day.
A, Axial T2-weighted image (2200/80/0.75 [TR/TE/excitation]) depicts bilateral cerebral atrophy distributed asymmetrically (left greater than right). Abnormally increased T2 signal is distributed within the white matter of the left centrum semiovale (arrow).
B, Axial proton density–weighted MR image (2200/30/0.75 [TR/TE/excitation]) depicts abnormally increased signal intensity within the posterior white matter bilaterally, left greater than right (arrow).
C and D, Axial 18F-Fluorodeoxyglucose (FDG) Positron Emission Tomography (PET) images at the level of the centrum semiovale (C) and suprasellar cistern (D) show marked hypometabolism throughout the left cerebral hemisphere, with some sparing of the inferior left frontal lobe.
E, Coronal FDG PET image depicts diffuse left cerebral (curved arrow) and right cerebellar (closed arrow) hypometabolism, ie, crossed cerebellar diaschisis. The left cerebellar hemisphere shows normal glucose metabolism (open arrow). Because of the compelling clinical presentation and neuroimaging findings, this patient underwent left hemispherectomy despite a nondiagnostic brain biopsy. Histopathologic findings obtained from the hemispherectomy specimen were consistent with Rasmussen encephalitis (Table).
F, The hemispherectomy specimen shows marked chronic inflammation, including lymphocytic meningitis (top), perivascular cuffing by lymphocytes, and an intraparenchymal lymphocytic infiltrate (hematoxylin and eosin stain, ×368). Neuronal loss and reactive astrocytosis are most apparent on the right side of the field (arrows). The discordance between the biopsy and hemispherectomy specimens likely reflects “sampling error” in the initial biopsy.
- fig 2.
Patient 7, a 10-year-old girl with a 5-year history of intractable seizures and progressive cognitive impairment. The MR and FDG PET images depict a pattern of focal atrophy superimposed on a background of generalized, but asymmetrically distributed, cerebral atrophy.
A–C, Axial T1-weighted images (A) (663/11/1 [TR/TE/excitation]), T2-weighted images (B) (2800/80/1[TR/TE/excitation]), and proton density–weighted MR images (C) (2800/30/1 [TR/TE/excitation]) depict diffuse bilateral but asymmetrical (left greater than right) sulcal prominence with superimposed, marked focal atrophy involving the left frontal lobe. The proton density–weighted image (C) depicts abnormally increased signal in the frontal white matter and posterolateral frontal gray matter (arrows). Signal also was abnormally increased within the frontal gray matter on more superior images (not shown).
D, Temporal-lobe long-axis axial FDG PET image at the level of the centrum semiovale depicts global left hemispheric hypometabolism with a more marked, superimposed focal region of hypometabolism in the left frontal lobe. The distribution of hypometabolism corresponds exactly to the regions of atrophy noted on MR imaging. Although the initial biopsy depicted mild diffuse astrocytosis, microglial proliferation, and perivascular mononuclear infiltration, a biopsy 4 years later depicted findings of “nonspecific encephalitis”. This may reflect either “sampling error” or progression to a “burned-out” phase of Rasmussen encephalitis.
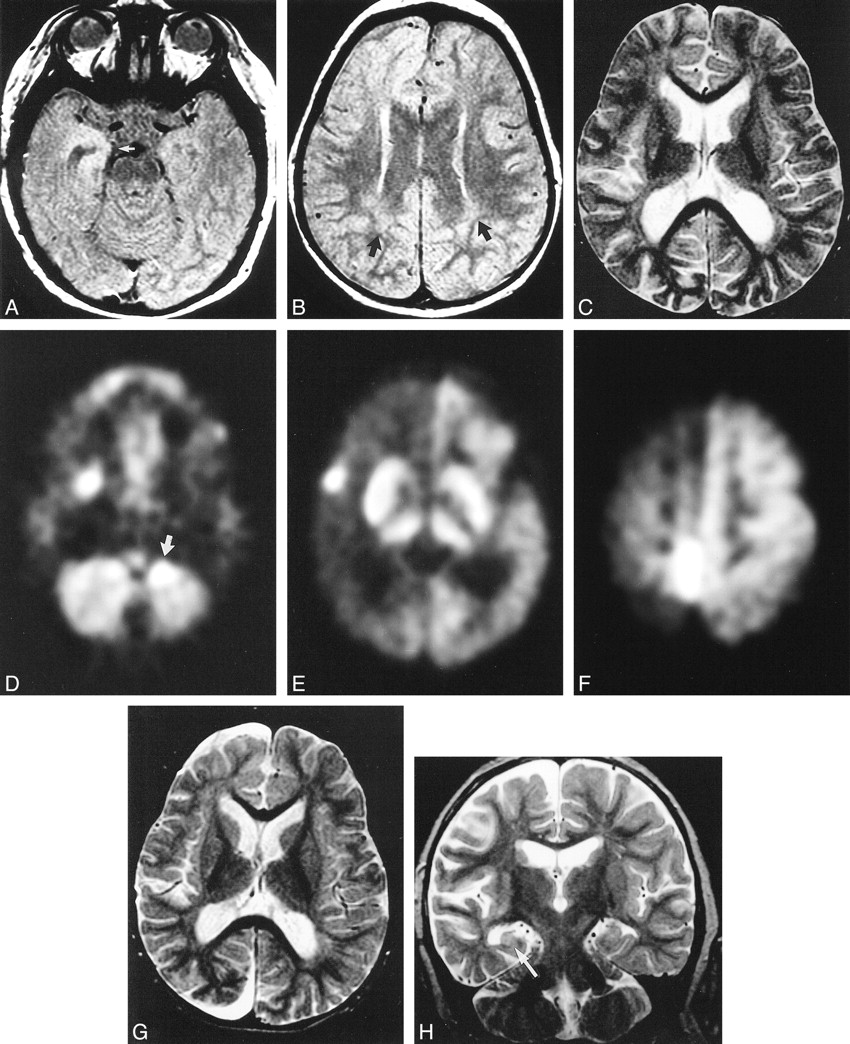
- fig 3.
Patient 3, a 27-month-old boy who presented with a 1-year history of intractable seizures followed by a progressive left hemiparesis.
A and B, Axial proton density–weighted images (2800/30/0.75 [TR/TE/excitation]) depict abnormally increased signal in the right medial temporal lobe gray matter (A, white arrow), right frontal gray and white matter (B), as well as the posterior white matter bilaterally (B, black arrows).
C, Axial T2-weighted image (2800/80/0.75 [TR/TE/excitation]) from the same examination depicts very mild bilateral atrophy, slightly more evident within the right cerebral hemisphere than the left.
D–F, Axial FDG PET images from an examination 5 days later depict global right hemispheric hypometabolism (E, F) with discrete foci of hypermetabolism (indicative of seizure activity at FDG administration) within the medial (D) and lateral (E) right temporal lobe, medial right parietal lobe (F), anterior left cerebellar hemisphere (D, arrow), and right basal ganglia (E). Correlation of the relatively nonspecific MR imaging features with the FDG PET data and clinical history provided a foundation for the diagnosis of Rasmussen encephalitis. In addition, the FDG PET data allowed the unequivocal identification of the affected hemisphere.
G, Axial T2-weighted images from MR imaging study (2800/80/1 [TR/TE/excitation]) 6 months later shows marked progression of the atrophy involving the right cerebral hemisphere, providing further evidence to support the diagnosis of Rasmussen encephalitis and confirm the identification of the affected hemisphere.
H, Fast spin-echo T2-weighted coronal image (4816/110/4 [TR/TE/excitations]) again depicts this asymmetrical (right greater than left) atrophy. In addition, the right hippocampus is atrophied and has abnormally increased T2 signal intensity (arrow). Because of the compelling clinical presentation and neuroimaging findings, this patient underwent right hemispherectomy despite two nondiagnostic brain biopsies. Histopathologic findings from the right hemispherectomy specimen were consistent with Rasmussen encephalitis. The disparity between the biopsy and hemispherectomy pathology results may be attributed to “sampling error”. This patient is now free of seizures and requires no antiepileptic medications (39 months after hemispherectomy).
- fig 4.
Patient 6, a 9-year-old girl who presented with intractable seizures at age 3.
A, Coronal fast spin-echo T2-weighted image (4000/112/3 [TR/TE/excitations]) through the parietal lobes depicts mild diffuse atrophy of the right cerebral hemisphere, with subtle sulcal prominence and asymmetrical dilation of the body of the right lateral ventricle.
B, Coronal FDG PET image (from a study 5 days earlier) through the same region depicts marked relative hypometabolism within the right cerebral hemisphere (arrow). Correlation of the MR imaging data with the FDG PET data and clinical history led to a diagnosis of Rasmussen encephalitis. Analysis of an initial brain biopsy specimen obtained from this patient yielded findings consistent with Rasmussen encephalitis; however, histopathologic analysis from the right hemispherectomy (5 years later) showed only scant perivascular lymphocytic infiltration. This scenario is most consistent with “burned-out” encephalitis. After hemispherectomy, patient 6 became free of seizures and currently requires no antiepileptic medications.
- fig 5.
Patient 8, a 7-year-old patient who, at the age of 5, had abrupt onset of intractable seizures (25 to 30 per day).
A and B, Axial FDG PET images depict global left cerebral hypometabolism with superimposed foci of hypermetabolism within the left parietal lobe (A) and right cerebellar hemisphere (B, arrow). The patient was actively seizing during injection of the radiopharmaceutical. The pattern of glucose hypermetabolism in this case indicates the propagation of seizure activity from the left parietal cortex to the right cerebellar hemisphere via corticopontocerebellar pathways. This patient underwent brain biopsy followed by left hemispherectomy. The histopathologic specimens from both procedures were interpreted as consistent with Rasmussen encephalitis. Hemispherectomy resulted in resolution of this patient's seizure disorder (at 2-year follow-up).





Tables

Surgical interventions and corresponding histopathologic results






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}