
Abstract
BACKGROUND: Long-term posttreatment surveillance imaging algorithms for head and neck squamous cell carcinoma are not standardized due to debates over optimal surveillance strategy and efficacy. Consequently, current guidelines do not provide long-term surveillance imaging recommendations beyond 6 months.
PURPOSE: We performed a systematic review to evaluate the impact of long-term imaging surveillance (ie, imaging beyond 6 months following completion of treatment) on survival in patients treated definitively for head and neck squamous cell carcinoma.
DATA SOURCES: A search was conducted on PubMed, EMBASE, Scopus, the Cochrane Central Register of Controlled Trials, and the Web of Science for English literature published between 2003 and 2024 evaluating the impact of long-term surveillance imaging on survival in patients with head and neck squamous cell carcinoma.
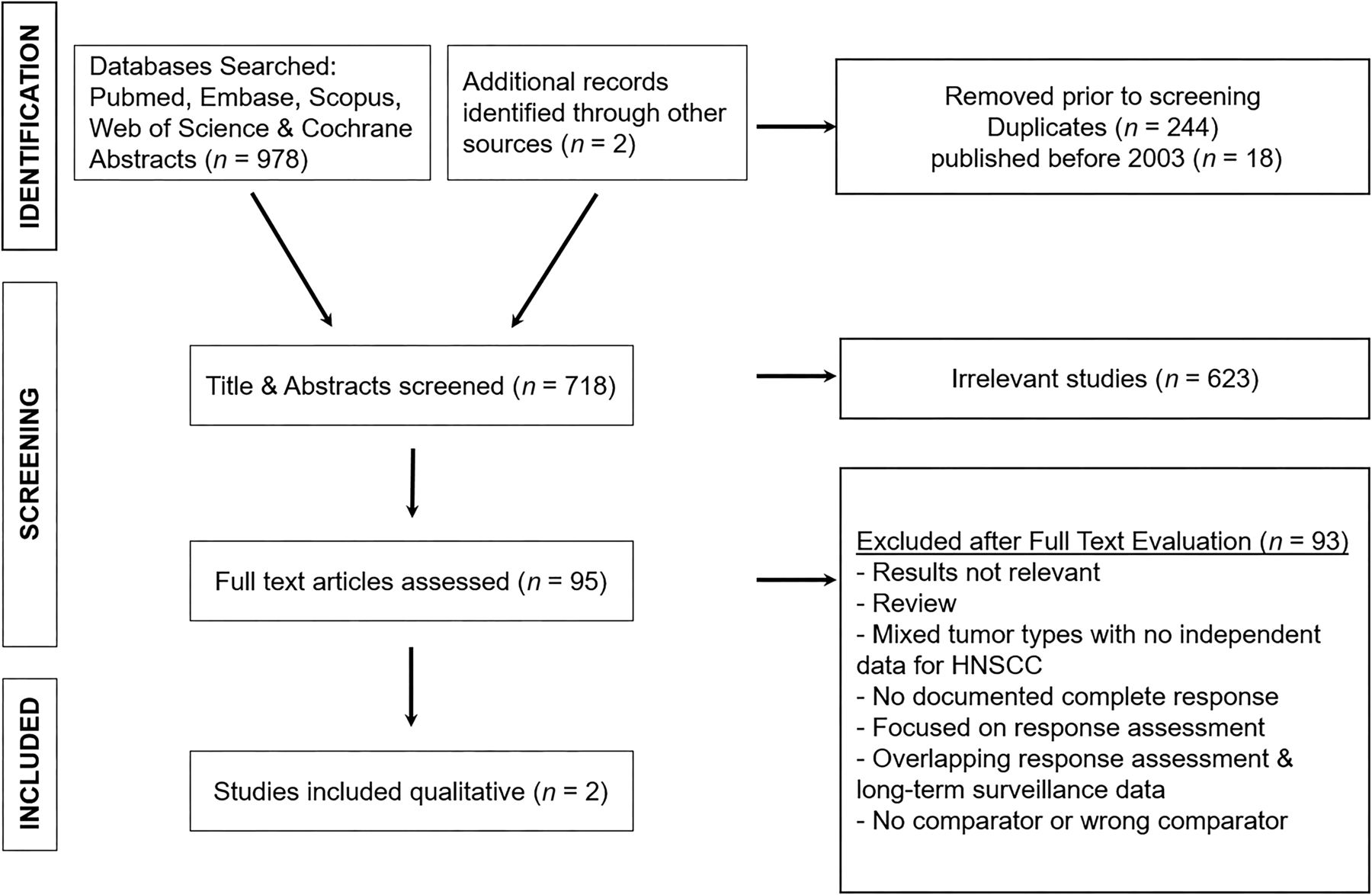
STUDY SELECTION: We screened 718 abstracts and performed full-text review for 95 abstracts, with 2 articles meeting the inclusion criteria. The Risk of Bias in Non-Randomized Studies of Interventions assessment tool was used.
DATA ANALYSIS: A qualitative assessment without a pooled analysis was performed for the 2 studies meeting inclusion criteria.
DATA SYNTHESIS: No randomized prospective controlled trials were identified. Two retrospective 2-arm studies were included comparing long-term surveillance imaging with clinical surveillance and were each rated as having a moderate risk of bias. Each study included heterogeneous populations with variable risk profiles and imaging surveillance protocols. Both studies investigated the impact of long-term surveillance imaging on overall survival and came to different conclusions, with 1 study reporting a survival benefit for long-term surveillance imaging with FDG-PET/CT in patients with stage III or IV disease or an oropharyngeal primary tumor and the other study demonstrating no survival benefit.
LIMITATIONS: Limited heterogeneous retrospective data available precludes definitive conclusions on the impact of long-term surveillance imaging in head and neck squamous cell carcinoma.
CONCLUSIONS: There is insufficient quality evidence regarding the impact of long-term surveillance imaging on survival in patients treated definitively for head and neck squamous cell carcinoma. There is a lack of a standardized definition of long-term surveillance, variable surveillance protocols, and inconsistencies in results reporting, underscoring the need for a prospective multicenter registry assessing outcomes.
ABBREVIATIONS:
- CFU
- clinical follow-up
- CR
- complete response
- CRT
- chemoradiotherapy
- HNSCC
- head and neck squamous cell carcinoma
- HPV
- human papillomavirus
- MPC
- metachronous primary cancer
- NCCN
- National Comprehensive Cancer Network
- NI-RADS
- Neck Imaging Reporting and Data System
- OS
- overall survival
- PFS
- progression-free survival
- RT
- radiation therapy
Treatment for head and neck squamous cell carcinomas (HNSCCs) is variable according to subsite and stage, often including a combination of surgery, radiation therapy (RT), and systemic therapy. Despite therapeutic advances, treatment failure is common, typically within the first 2 years following treatment.1,2 Within 6 months following definitive therapy, defined as the initial response assessment period, the National Comprehensive Cancer Network (NCCN) guidelines recommend CT, MRI, or FDG-PET/CT to assess an incomplete response.3 However, to date, posttreatment long-term surveillance imaging (defined as imaging beyond 6 months after an initial complete response [CR]) is not standardized due to debates over optimal imaging technique, schedule, cost-effectiveness, and a paucity of strong evidence demonstrating improved survival. Consequently, the current NCCN guidelines do not recommend surveillance imaging beyond 6 months. Similarly, the European Society for Medical Oncology does not recommend imaging surveillance beyond 3 months posttreatment unless clinically indicated.4 In this systematic review, we searched for evidence to evaluate the impact of long-term surveillance imaging on overall survival (OS) in patients treated definitively for HNSCC.
MATERIALS AND METHODS
Search Strategy
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.5 The search strategy was guided by investigators and designed by a medical librarian (D.A.-D.) using synonyms through index searching with Medical Subject Headings (MeSH), applying combinations of subject headings and keywords to identify English language articles published between 2003 and 2024. Searches were conducted in November 2023 and in March 2024 in an attempt to capture recent publications on PubMed, EMBASE, Scopus, Cochrane, and the Web of Science using the following keyword and MeSH terms: “head and neck cancer,” “head and neck neoplasms,” “radiology,” “imaging,” “diagnostic imaging,” “tomography,” “X-Ray,” “computed,” “positron emission tomography,” “MR imaging,” “surveillance,” “surveillance imaging,” “mortality,” “survival,” and “treatment outcome.” We retrieved 978 articles, and 2 articles6,7 were provided by investigators during the initial study design and citation searching, respectively. After removing duplication in EndNote (https://web.endnote.com) and the exclusion of studies published before 2003 due to obsolete imaging technology, there were 718 results. Reference lists of identified studies were screened for eligibility, and references were included when appropriate. Detailed search strategy is provided in the Online Supplemental Data.
Article Selection Process.
We identified 718 studies for screening using Covidence Software (Veritas Health Innovation). Six hundred twenty-three abstracts were screened by 1 author (T.J.R). Ninety-five full-text articles were assessed (T.J.R. and P.W.). Secondary full-text review was performed for 24 articles by 2 board-certified radiologists with 17 and 15 years of experience (T.J.R. and P.W.). Three reviewers (T.J.R., P.W., and C.M.-H.) evaluated 4 articles,6,8⇓-10 and 2 studies met the inclusion.6,8 Evaluated articles are provided in the Online Supplemental Data. Included studies evaluated the impact of long-term surveillance imaging on survival in adult patients with HNSCC treated definitively with a documented initial CR within the first 6 months, clear reporting of outcomes, and the comparator being clinical surveillance or no surveillance. Long-term surveillance imaging was defined as imaging performed after 6 months following completion of treatment. Exclusion criteria were the following: 1) did not evaluate the impact of long-term surveillance imaging; 2) focused on response-assessment imaging before 6 months following completion of treatment or did not report results separately for long-term surveillance imaging; 3) did not include patients with HNSCC or did not report results separately for HNSCC; 4) no comparator; 5) published before 2003; and 6) children or mixed age populations unless most subjects were 18 years of age or older or results were reported separately for those 18 years of age or older. Articles without primary data were excluded including review articles, practice guidelines, case reports, case series, commentaries, and editorials.
Data Extraction
We extracted the following data: study design; patient population and source; study size; inclusion and follow-up period; treatment; clinical surveillance protocol; imaging surveillance protocol; metachronous primary cancer (MPC) data; treatment failure data; survival outcomes; and salvage outcomes.
Study Quality Assessment
Studies meeting inclusion were evaluated using the Risk of Bias in Non-Randomized Studies of Interventions assessment tool, designed to assess the risk of bias in estimates of the effectiveness of an intervention from studies without randomization.11
RESULTS
Selected Studies
The search yielded 718 citations, of which 95 full-text articles were evaluated with 24/95 undergoing secondary full-text review. A common reason for exclusion was failure to assess the independent impact of long-term surveillance imaging, with many studies evaluating the impact of response assessment imaging performed ≤6 months following treatment completion. Some excluded studies combined response assessment and long-term surveillance imaging data, precluding an independent evaluation of long-term surveillance imaging on survival. Additional studies were excluded for other reasons, including no documented disease-free interval, no comparator or a wrong comparator, no survival or outcome data, and no separate data for HNSCC. No randomized controlled trials were identified. The Online Supplemental Data summarize the 2 studies that met inclusion,6,8 which were both retrospective, nonrandomized studies, with a moderate risk of bias. The Figure details the selection process.

Study-selection process.
Primary Tumor Characteristics and Treatment
Both studies included patients with newly diagnosed HNSCC arising from variable mucosal subsites treated definitively, with a documented CR by imaging within 6 months of conclusion of treatment.6,8 Both studies included oropharynx, larynx, and hypopharynx subsites. Chen et al8 included the nasopharynx and a subsite listed as “other.” Leclère et al6 included oral cavity and unknown primary cancers. Chen et al8 included only patients treated with primary RT or chemoradiotherapy (CRT), with 56% (190/340) of patients having an oropharyngeal primary cancer and 42% (142/340) testing p16-positive, used as a surrogate for human papillomavirus (HPV). Leclère et al6 included patients treated variably with surgery, RT, or multimodality therapy and indicated that HPV status was unknown for most patients.
Surveillance Modalities and Algorithms
Leclère et al6 evaluated the impact of long-term surveillance FDG-PET/CT with standardized FDG-PET/CT results at 12, 24, and 36 months posttreatment. Chen et al8 assessed the impact of long-term surveillance FDG-PET/CT, MRI, or CT of the head and neck performed at variable times beyond 6 months posttreatment in asymptomatic patients. Both studies incorporated chest CT scans for screening lung cancer among smokers as part of the clinical surveillance cohort and used different standardized clinical surveillance algorithms.
Treatment Failure and Survival Outcomes Reported
Both studies investigated the impact of long-term surveillance imaging on OS and came to different conclusions.6,8 Chen et al8 additionally reported progression-free survival (PFS). The Online Supplemental Data detail the survival results, and Table 1 details surveillance results.
Imaging and clinical surveillance results
Leclère et al6 retrospectively evaluated 782 patients with a minimum of 3 years’ follow-up, 497 of whom had FDG-PET/CT surveillance imaging and 285 of whom had only clinical follow-up (CFU).6 The primary end point was OS defined as the time from diagnosis to death from any cause with censoring at the last follow-up if no death. Survival curves were estimated using the Kaplan-Meier method, and log-rank tests were used to test statistically significant difference in OS. Cox proportional hazards modeling was used to assess the difference in OS between surveillance and CFU groups, adjusting for potential confounders. The overall unadjusted analysis comparing survival curves for FDG-PET/CT surveillance versus CFU found a survival benefit for FDG-PET/CT surveillance (P = . 002). Three-year mean OS was better in the FDG-PET/CT surveillance group compared with the CFU group (72.5% versus 64.3%; P = .002), including for stage III–IV disease (68.5% versus 55.4%; P < .001). No difference in mean 3-year OS was observed for stages I–II comparing the FDG-PET/CT versus CFU groups (84.5% versus 79.4%; P = .72). When we stratified by tumor location, there was a >3-year OS for oropharyngeal tumors in the FDG-PET/CT versus the CFU group (69.9% versus 60.5%; P = .04), but not for oral cavity tumors (72.4% versus 60.1%; P = .11), laryngeal tumors (75.9 versus 73.4%; P = .62), or hypopharyngeal (66.3% versus 64.1%; P = .27) tumors.
Among 164 patients with recurrence, the mean 3-year OS was better in the FDG-PET/CT group compared with the CFU group (36.4% versus 22.2%; P = .005). Several risk factors were statistically significantly worse in the FDG-PET/CT versus CFU group, including a higher prevalence of cancer history and immunodeficiency, greater unfavorable performance status scores, higher rates of unfavorable alcohol consumption, and more patients with advanced-stage disease (stage III–IV). Multivariable Cox modeling results adjusting for potential confounders (age, sex, comorbidities, primary location, stage, surgeon, treatment year, and treatment) agreed with the unadjusted (Kaplan-Meier/log-rank) analysis. The adjusted hazard ratio from Cox modeling was 0.71 (95% CI, 0.57–0.88; P = . 002), indicating better survival in the FDG-PET/CT surveillance group.
Chen et al8 retrospectively evaluated 340 patients, 187 of whom underwent surveillance imaging using variable modalities and 153 of whom underwent clinical surveillance or expectant management, which could include screening chest CT and other medical imaging based on clinical needs. Ninety-five percent (178/185) of patients in the imaging-based surveillance cohort had at least 1 FDG-PET/CT scan. Survival curves were estimated using the Kaplan-Meier method; it was unclear what statistical test was used to test statistically significant differences in OS and PFS. OS was defined as the time from the last day of radiation to death (censored at the last clinic follow-up). When we compared the imaging group versus the clinical surveillance group, the authors found no difference in 3-year OS (94% versus 93%, P = .64), PFS (89% versus 88%, P = .46), local-regional control (90% versus 93%, P = .47), or freedom from distant metastasis (90% versus 90%, P = .38). There were no differences found in 3-year OS in subgroup analysis stratified by covariates, including T-stage, performance status, HPV-positivity, and tobacco use.
DISCUSSION
This systematic review investigated the impact of long-term imaging surveillance on the survival of patients with treated HNSCC compared with those monitored using a clinical surveillance protocol. Two studies met the inclusion criteria with divergent conclusions regarding the impact of long-term surveillance imaging on survival.6,8 Leclère et al6 reported that most imaging-detected recurrences were subclinical, amenable to curative treatment, occurred within the first 2 years after treatment, and decreased in frequency with time. This recurrence information translated into a survival benefit for long-term surveillance imaging with FDG-PET/CT among patients with advanced-stage (III or IV) disease (3-year OS of 68.5% FDG-PET/CT versus 55.4% CFU) or an oropharyngeal primary tumor (3-year OS of 69.9%, FDG-PET/CT versus 60.5% CFU). Furthermore, following recurrence detection, the 3-year OS was better in the FDG-PET/CT group (36.4%) compared with the CFU group (22.2%), suggesting that earlier detection and treatment of recurrence or MPC result in better outcomes. The timing and frequency of surveillance imaging are important because FDG-PET/CT detects 80% of asymptomatic recurrences within the first year after treatment, arguing for more frequent surveillance in the first year.12 It is possible that the study of Leclère et al6 may have shown a greater impact on survival if additional surveillance data between 6 and 12 months were included. A recent, large, retrospective, population-based study by Anzai et al,10 which combined response assessment and long-term surveillance imaging data, similarly found a survival benefit with posttreatment FDG-PET/CT in patients with advanced-stage HNSCC with nodal or distant metastases.
Chen et al8 found no survival benefit from long-term surveillance imaging in a cohort with an unspecified stage and varied imaging modalities, despite most patients undergoing at least 1 FDG-PET/CT scan. Other retrospective studies not meeting the inclusion criteria also suggested that posttreatment imaging detects subclinical recurrence but does not improve survival.9,13,14 In a single-arm retrospective study including patients with HNSCC with an initial CR, Ho et al9 found no survival difference between patients with FDG-PET/CT-detected versus clinically-detected recurrences. The conflicting results of these studies are likely related to the retrospective nature with variable inclusion criteria comprising patient demographics, risk profiles, primary tumor site, HPV status, surveillance algorithms, timing of imaging, and treatment regimens confounding outcomes. Variations in tumor stages among patients may contribute to differing conclusions. Leclère et al6 included a majority (71%, 553/782) of patients with advanced-stage disease, 35% (276/782) of whom had primary oropharyngeal tumors and 62% (484/782) of whom had primary tumors outside the oropharynx. Chen et al8 did not report the stage and included mostly patients with primary oropharyngeal tumors (56%, 190/340), many of whom were HPV-positive (40%, 136/340).
If long-term surveillance imaging proves to offer survival benefits exclusively for advanced-stage cancers rather than early-stage ones, a study like that of Leclère et al,6 which focused on advanced-stage disease, would likely demonstrate such benefits compared with studies primarily involving patients with early-stage cancers or low-risk recurrence. Additionally, given the modest sample size and low event rate, the study of Chen et al8 may be underpowered to detect small-but-clinically meaningful differences in OS. Differences in survival outcomes between studies could also be attributed to variations in the proportion of patients treated with curative intent after recurrence. In Leclère et al,6 >80% of subclinical recurrences received curative treatment. Chen et al8 did not report the number of recurrences treated with curative intent but noted a lower positive predictive value of biopsies and greater morbidity in the imaging surveillance group related to invasive procedures or treatment complications.
The detection of MPC may have also impacted the differences in survival benefit. Excluding cutaneous neoplasms, Leclère et al6 reported a 10% MPC detection rate (51/497) in the FDG-PET/CT group, with 90% receiving curative treatment. Chen et al8 reported a 20% MPC detection rate (68/340, including cutaneous neoplasms), with no difference between the imaging- and clinically-based surveillance cohorts and no indication of the percentage treated curatively. Others have also shown the crucial role of imaging in detecting MPC, potentially improving patient outcomes.15,16 Ng et al16 found that nearly 10% of patients with HNSCC treated definitively with RT developed an MPC, particularly among current or former smokers. Most patients with MPCs received curative treatment, with 5-year OS exceeding 40%, emphasizing the importance of surveillance for MPCs.
Our study identified several issues in the literature regarding the role of long-term surveillance imaging, including the following: 1) a lack of a standard definition, timing, and technique for surveillance imaging across studies; 2) undocumented disease-free intervals; and 3) aggregating data of patients with different tumor biology, risk for treatment failure, and treatment options. Furthermore, the lack of prospective studies comparing long-term imaging with clinical surveillance hinders guideline establishment. Consequently, most guidelines (Table 2) recommend no routine imaging surveillance required after 6 months unless clinically indicated or for tumors inaccessible to clinical examination.3,4,17,18
Various guidelines for imaging surveillance in HNSCC
The goal of long-term surveillance imaging is early detection of recurrence or MPC in high-risk patients to provide curative treatment and improve mortality. Factors to consider when performing long-term surveillance imaging include the following: recurrence risk, temporal recurrence patterns, accurate test availability, available effective treatment or clinical trials, cost-effectiveness, and patient perspective. Subclinical recurrence frequently occurs beyond 6 months posttherapy. Patients with locally advanced HNSCC have a high likelihood of locoregional recurrence or distant metastases, with up to 50% experiencing this result within the initial 2 years posttreatment.1,2 In the systematic review by Van Hoe and Hermans,19 41% of locoregional HNSCC recurrences and/or metastases was exclusively identified by imaging. Furthermore, the average time of detecting recurrent or metastatic disease was 11.5 months after the initial 6-month response-assessment period. Among surveillance modalities, FDG-PET/CT performs favorably versus MRI or CT.20,21 Salvage surgery is feasible for certain patients, with variable outcomes related to recurrence location, stage, and performance status.22 Additionally, recent advances in immunotherapy such as pembrolizumab may lead to long-term remission in the setting of refractory and/or metastatic HNSCC.23 HPV status is particularly important, with patients with HPV+ HNSCC showing delayed metastases and longer survival after metastasis detection compared with patients with HPV–.2,24⇓⇓-27 Furthermore, tailored surveillance is essential due to diverse treatment failure patterns and prognosis between HPV+ and HPV– HNSCC. Considering all factors, some authors support long-term surveillance imaging for up to 2 years posttreatment, with FDG-PET/CT being the preferred method.19,28
There are current efforts to enhance evidence-based surveillance in HNSCC. The strong negative predictive value of FDG-PET/CT posttreatment is prompting assessment of its role in personalized cancer surveillance models.29 One ongoing prospective clinical trial is exploring the impact of long-term surveillance imaging on HNSCC survival,30 while at least 2 other trials were terminated due to nonfeasibility issues,31,32 because data suggest that providers and patients value reassurance from surveillance imaging.33,34 Ideally, prospective randomized controlled trials would provide the highest level of evidence but face challenges in acceptance among providers and patients and are logistically difficult due to preauthorization requirements, limiting generalizability. Additionally, the impact of surveillance imaging on survival depends on treatment types, effectiveness, and patient compliance. A more feasible approach could involve a multicenter prospective registry assessing outcomes in patients with definitively treated HNSCC with CR at 6 months posttreatment.
In 2016, the American College of Radiology established The Neck Imaging Reporting and Data System (NI-RADS) to standardize and establish predictive imaging reporting for head and neck cancer surveillance. NI-RADS assigns scores for the primary site and regional lymph nodes conveying the suspicion level for locoregional recurrence and provides recommendations for management or follow-up imaging.18 Initial data suggest good interobserver agreement and predictive value of NI-RADS for guiding imaging surveillance and management.35,36 Additionally, ongoing research on the mathematical model assessing treatment-failure risk (based on patient and disease-specific factors) and the use of circulating tumor DNA may contribute to future patient-specific surveillance algorithms.37⇓⇓⇓-41
There are several limitations within this systematic review. First, the study is constrained by a small volume of data, precluding conducting a meta-analysis. Most studies lacked direct comparison between long-term imaging and clinical surveillance protocols. No prospective studies were available. There was wide variation in study design, including variability in surveillance protocols such as imaging technique and the timing of follow-up in each study. Data regarding HPV and Epstein-Barr virus–related tumors that impact prognosis and management were incomplete in most publications. Treatment techniques for HNSCC have evolved, leading to variable treatment protocols, which could impact outcomes.
CONCLUSIONS
There is insufficient high-quality evidence regarding the impact of long-term surveillance imaging on survival in patients definitively treated for head and neck squamous cell carcinoma. Retrospective data suggest that FDG-PET/CT effectively detects subclinical recurrence and metachronous primary cancer and may improve survival in select patients with head and neck squamous cell carcinoma. Our study underscores the necessity for prospective multicenter pragmatic trials assessing the optimal surveillance schedule, duration, and the survival impact of long-term surveillance imaging in patients at risk for treatment failure who may benefit from salvage therapy.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received May 20, 2024.
- Accepted after revision June 15, 2024.
- © 2025 by American Journal of Neuroradiology





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.