
Abstract
BACKGROUND AND PURPOSE: Ruptured PICA aneurysms present considerable treatment challenges due to their rarity and proximity to critical neurovascular structures. This study aims to report and critically analyze the long-term neurologic outcomes of patients with ruptured PICA aneurysms treated at our tertiary center and to evaluate the prognostic value of prepontine cistern filling grade on initial CT scans.
MATERIALS AND METHODS: Clinical and radiologic data were retrospectively collected for consecutive patients with ruptured PICA aneurysms treated at our institution between January 2010 and December 2021. The prepontine cistern filling was graded from 0–3 on sagittal slices of the initial CT scan by 2 independent readers.
RESULTS: Fifty-seven patients with ruptured PICA aneurysms were included. The mean aneurysm diameter was 7.2 mm (SD ± 4.9), with a mean radiologic follow-up of 40.2 months (SD ± 45.2). Endovascular treatment was the primary technique (96.5%), with a small number (3.5%) requiring microsurgical clipping. Parent vessel sacrifice was performed in 49% of cases. Complete aneurysm occlusion was achieved in 79% of patients, with a recurrence rate of 19%. External ventricular drainage was necessary in 83% of patients, and 28% later required a permanent ventricular shunt. Symptomatic vasospasm occurred in 37% of patients. The in-hospital mortality rate was 11%, and 55% of survivors required a transient tracheostomy. At 1-year posthemorrhage, 60% had a good neurologic outcome. Multivariate analysis revealed that poor neurologic outcomes were significantly associated with higher grade of prepontine cistern filling (P < .05) and in those whose parent vessel had to be sacrificed (P < .05).
CONCLUSIONS: Ruptured PICA aneurysms carry a grim prognosis and pose major management challenges. Both the grade of prepontine cistern filling on initial CT scan and the need for parent vessel sacrifice are important prognostic factors.
ABBREVIATIONS:
- GCS
- Glasgow Coma Scale
- IQR
- interquartile range
- WFNS
- World Federation of Neurosurgical Societies
SUMMARY
PREVIOUS LITERATURE:
Ruptured PICA aneurysms are rare and present considerable treatment challenges due to their anatomic complexity and high prevalence of fusiform shapes. Consequently, patients with ruptured PICA aneurysms generally have poorer prognosis compared with those with aneurysms located elsewhere. Although previous studies have identified predictive factors for poor neurologic outcomes in subarachnoid hemorrhage, the specific locoregional challenges associated with PICA aneurysms necessitate further investigation into particular predictive factors. These patients are at an elevated risk of brainstem compression, which may not be detected through standard supratentorial monitoring of intracranial pressure.
KEY FINDINGS:
Our retrospective monocentric study identified the grade of prepontine cistern blood filling as a strong and independent predictive factor of poor neurologic outcome in patients with ruptured PICA aneurysms. This underscores the importance of accurately assessing brainstem compression, which is related to the available space in the posterior fossa for this subgroup of patients.
KNOWLEDGE ADVANCEMENT:
We developed a prognostic classification for patients with ruptured PICA aneurysms, based on a simple grading system for prepontine cistern blood filling. This system independently predicts neurologic outcomes, providing valuable guidance for clinicians managing these complex cases.
PICA aneurysms account for approximately 0.5%–3% of all intracranial aneurysms.1,2 Patients with ruptured PICA aneurysms experience worse outcomes compared with those with ruptured aneurysms in other locations, irrespective of their Fisher grade, Hunt and Hess grade, or vasospasm rate at admission.3 The high incidence of poor neurologic outcomes in these patients is likely multifactorial, involving factors such as the higher prevalence of fusiform aneurysms, the proximity of these aneurysms to the brainstem and lower cranial nerves, and the presence of large infratentorial cisternal clots.3⇓-5 Despite advances in both endovascular and microsurgical techniques, treating these rare aneurysms remains a major challenge.3,5 Furthermore, the standardized clinical management of severe SAH is often limited to invasive intracranial pressure monitoring in the supratentorial compartment, despite well-documented differences in pressure between supra- and infratentorial compartments.6 Prognosis classifications for SAH primarily focus on anterior circulation aneurysms, highlighting the need for more robust and specific prognostic indicators for posterior circulation aneurysms. The presence of blood in the subarachnoid cisterns of the posterior fossa has been identified as a prognostic factor in traumatic brain injuries and SAH, potentially contributing to subsequent vasospasm.7 However, despite the frequent observation of blood in the prepontine cistern following ruptures of PICA aneurysms, its prognostic significance for neurologic outcomes has not been documented so far. Importantly, in the context of posterior fossa SAH, the prepontine cistern plays a crucial role in allowing anterior displacement of the brainstem by the compressive clot. Should this space become filled or obliterated, there is a substantial risk of severe brainstem compression.
This study aims to report the long-term neurologic outcomes of patients with ruptured PICA aneurysms and to evaluate the prognostic value of prepontine cistern filling in these patients.
MATERIALS AND METHODS
Approval for this study was obtained from the institutional ethics board (IRB #00011687: 2024/17). In accordance with local regulations, patient consent was waived for this retrospective analysis of anonymized data. The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Data Collection
This monocentric retrospective study was conducted according with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.8 All consecutive adult patients referred to our tertiary center for a ruptured PICA aneurysm between January 2010 and December 2021 were retrospectively identified and included. Inclusion criteria were: patients aged ≥18 who presented with SAH associated with a ruptured PICA aneurysm. Exclusion criteria included patients with other potential causes for SAH, such as a concomitant arteriovenous shunt or recent head trauma, to avoid potential confounding factors. Clinical data were retrospectively collected through medical chart review. Functional neurologic status was evaluated by using the mRS at baseline and 1 year postrupture.9 The Glasgow Coma Scale (GCS) and World Federation of Neurosurgical Societies (WFNS) scale were used to assess clinical status on the day of rupture.10,11 Variables such as sex, age, clinical status on admission, and vascular comorbidities such as blood hypertension, history of stroke, or diabetes were recorded.
Radiologic Assessment
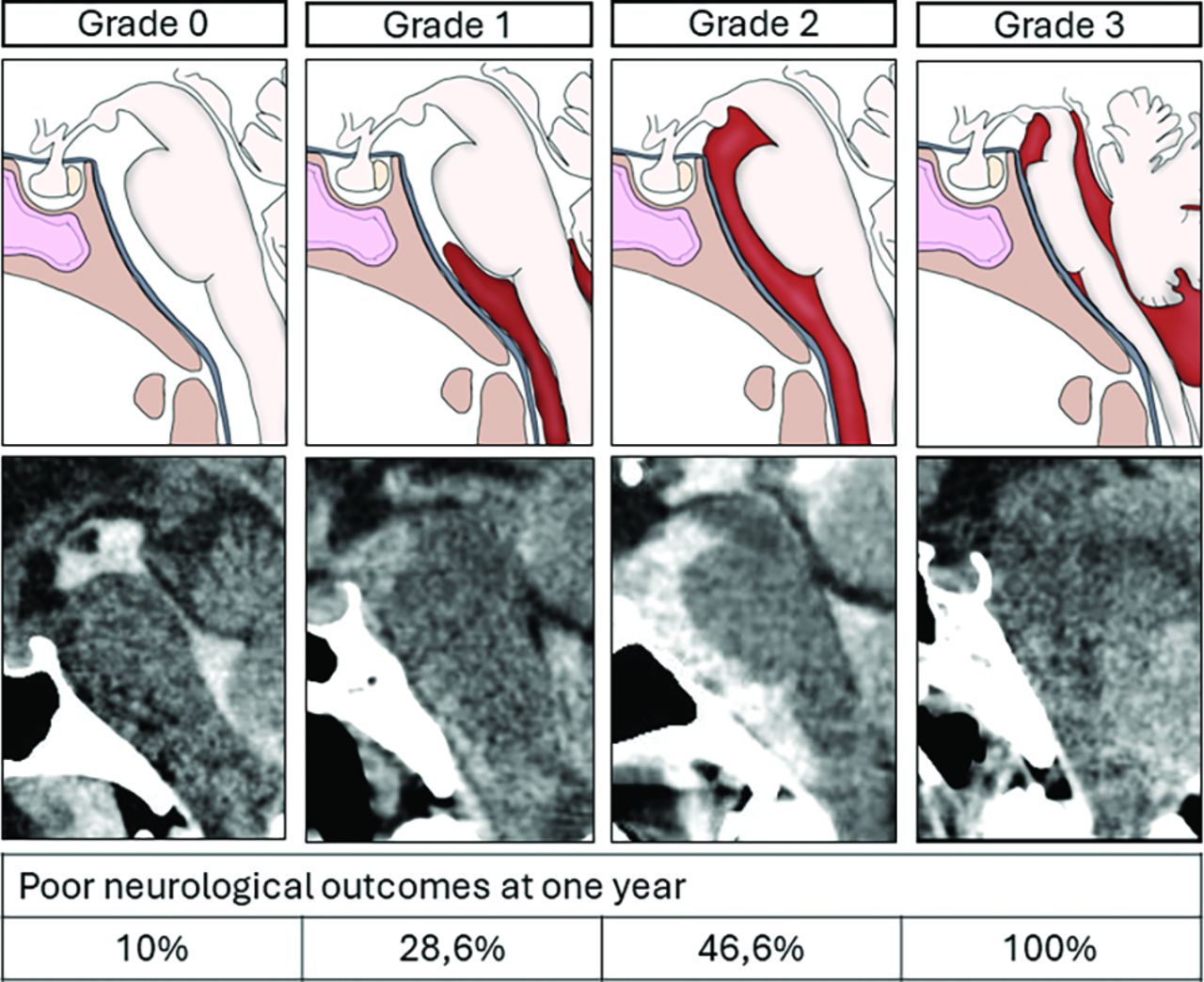
The severity of intracranial bleeding on the initial CT scan was assessed by 2 experienced physicians in cerebrovascular diseases; 1 interventional neuroradiologist (K.P.) and 1 neurosurgeon (E.L.), with 7 and 6 years of experience in brain aneurysm management, respectively. The readers evaluated the following criteria: exact location of the aneurysm on the segments of the PICA (Fig 1), Fisher grade, presence of blood in the fourth ventricle, intracerebellar hemorrhage, blood filling of the cisterna magna, the fusiform or saccular shape of the aneurysm, and the prepontine cistern filling grade. The prepontine cistern filling grade was assessed on the initial CT scan on a sagittal slice as follows: grade 0 when the prepontine cistern was entirely free and only filled with CSF; grade 1 when it was partially filled with blood but some CSF remained visible; grade 2 when the prepontine cistern was entirely filled with blood and no CSF was visible; and grade 3 when the protuberance was directly in contact with the clivus (Fig 2). Discrepancies between raters were resolved by consensus through concomitant review of the CT scan.12

Segments of the PICA. A, Illustration of the lateral view of the brainstem and cerebellum, highlighting the different segments of the PICA and its proximal segments’ close relationship with the lower cranial nerves. B, Graphic representation of good neurologic outcomes based on the location of the aneurysm along the PICA. Ant. = anterior; Lat. = lateral; Med. = medullary; Tel.Vel. = telo-velar; Tons. = tonsillar.

Classification of prepontine cistern filling, with graphic illustrations and examples of sagittal CT scans. Grade 0: The prepontine cistern is entirely filled with CSF, indicating no blood presence. Grade 1: The prepontine cistern is partially filled with blood but still contains CSF. Grade 2: The prepontine cistern is completely filled with blood, leaving no visible CSF. Grade 3: The prepontine cistern is not visible, indicating the brainstem is in direct contact with the clivus, representing severe hemorrhagic impact and brainstem compression.
Statistical Analysis
Data are reported as mean ± SD for continuous variables and median (interquartile ranges [IQRs]) for noncontinuous variables. Interrater reliability between 2 raters (K.P. and E.L.) for the prepontine cistern filling grade was assessed by using Cohen κ coefficient, with a k index ≤ 0.40 indicating poor agreement, 0.41–0.60 moderate, 0.61–0.80 good, and 0.81–1 excellent.13 Univariate analyses and graphical representations were conducted with Prism (Version 9.0.0, GraphPad Software). Group comparisons were made by using the nonparametric Mann-Whitney U test for continuous variables and χ2 or Fisher exact test for binomial variables. Additional analyses were performed by using R (Version 4.3.2, R Foundation for Statistical Computing) through the RStudio interface (Version 2022.07.2 + 576, RStudio, PBC). Data were examined to ensure no violation of the assumptions for logistic regression. A multivariate logistic regression model assessed the association between the presence of CSF in the prepontine cistern and poor neurologic outcome, adjusting for known predictors such as WFNS scale and parent vessel sacrifice. ORs, 95% CIs, and P values were derived to assess the strength and significance of associations. All tests were 2-sided, and P value of < .05 considered statistically significant.
RESULTS
Study Population
Fifty-seven patients with SAH from ruptured PICA aneurysms were included, with a female-to-male ratio of 2:1 and a median age of 52 years (IQR 44–64). Vascular comorbidities were present in 27 patients (47%), and 7 patients (12%) were on antithrombotic therapies before the rupture. All patients were independent at baseline (mRS ≤2): 53 patients (93%) were asymptomatic (mRS = 0), 3 (5.3%) had mild symptoms (mRS = 1), and 1 (1.7%) had slight disability (mRS = 2). The GCS scores were 15 in 18 patients (31.6%), 13–14 in 8 patients (14%), 7–12 in 12 patients (21%), and 3–6 in 19 patients (33%). WFNS grades were: 1 in 18 patients (32%), 2 in 7 (12%), 3 in 1 (1.7%), 4 in 4 (7%), and grade 5 in 19 (33%). Fisher grades were: 1 in 2 patients (3.5%), 2 in 1 (1.7%), and 4 in 54 (95%). Blood in the fourth ventricle was seen in 51 patients (90%), intracerebral hemorrhage in 9 (16%), and associated hydrocephalus requiring external drainage in 47 (83%). Prepontine cistern filling was graded as 0 in 5 patients (8.8%), 1 in 28 patients (49%), 2 in 14 patients (25%), and 3 in 10 patients (18%). The calculated Cohen κ coefficient was 0.819, indicating excellent interrater reliability (P < .05). The characteristics and outcomes of patients in each prepontine cistern filling grade are summarized in Table 1. Nine patients had additional aneurysms. Aneurysms were located on the left PICA in 33 cases (58%) and were fusiform in 33 cases (58%) and saccular in 24 cases (42%). Thirty-three aneurysms (58%) were located on the left PICA and were distributed as follows: 32 aneurysms (56%) were located on the anterior medullary segment with 31.3% of them being fusiform, 9 aneurysms (16%) were located on the lateral medullary segment with 88.9% of them being fusiform, 5 aneurysms (8.8%) were located on the tonsillar medullary segment and were all fusiform (100%), 10 aneurysms (18%) were located on the telo-velar tonsillary segment and were all fusiform (100%), and 1 aneurysm (1.8%) was cortical and fusiform (Fig 1). The mean maximal diameter was 7.2 mm (±4.9). The median time from symptom onset to treatment was 22 hours (IQR 14–47), with 8 patients (14%) experiencing rebleeding before aneurysm exclusion. Fifty-five patients (97%) received endovascular treatment, while 2 patients (3.5%) underwent microsurgical clipping. Endovascular procedures included simple coiling in 28 cases (49%), parent vessel sacrifice by n-butyl cyanoacrylic glue (Glubran) in 15 cases (26%) or simple coiling in 11 cases (19%), and flow-diversion stent placement in 1 case (1.8%). Parent vessel sacrifice was necessary in 28 patients (49%), varying by aneurysm location: 22% in patients with anterior medullary segment aneurysm, 89% in those with lateral medullary segment aneurysm, 80% each in patients with tonsillar medullary segment and telo-velar tonsillar segment aneurysm, and 100% in those with cortical aneurysm. Parent vessel sacrifice was more common in fusiform than saccular aneurysms (77% versus 8.7%; P < .001). There was no statistically significant change in the frequency of parent vessel sacrifice over the duration of the study (P = .36). The characteristics and outcomes of patients with and without parent vessel sacrifice are summarized in Table 2. Four patients (7%) required posterior fossa craniectomy, with 2 also needing intracerebellar hematoma evacuation, on average 15.3 hours (SD ± 8.3) postsymptom onset.
Characteristics of the study population based on the prepontine cistern filling grade
Characteristics of the study population based on the parent vessel status
Outcomes
Complete aneurysm occlusion was achieved in 45 patients (79%) after the initial procedure. At last follow-up, 11 patients (19%) experienced aneurysm recurrence, with 5 requiring a second treatment. The final occlusion rate was 76%. Symptomatic vasospasm requiring active medical or endovascular treatment occurred in 21 patients (37%). An external ventricular drain was placed in 47 patients (83%), and 16 patients (28%) required further internal ventricular shunt surgery. The median hospital length of stay was 29 days (IQR 19–48.5). The mean follow-up was 40.2 months (SD ± 45.2), with an in-hospital mortality rate of 11%. Among survivors, 28 patients (55%) required transient tracheostomy. One year posthemorrhage, 34 patients (60%) had good neurologic outcomes, with only 7 (14%) having persistent lower cranial nerve palsy.
Prognosis Factors
One year posthemorrhage, poor neurologic outcomes varied with prepontine cistern filling grades: 10% in grade 0, 29% in grade 1, 46% in grade 2, and 100% in grade 3 (Fig 2). Univariate analysis demonstrated a significant association between prepontine cistern filling grade avec poor neurologic outcomes at 1 year (P < .05; Table 3 and 4). Patients who underwent parent vessel sacrifice exhibited worse neurologic outcomes compared with those who did not (61% versus 21%; P < .05). Higher WFNS grades were also associated with poorer neurologic outcomes compared with those with lower grades (P < .05). There was no significant difference in outcomes based on Fisher grades (P = .78), the need for external ventricular drain (P = .28), or aneurysm type (fusiform versus saccular; P = .13). Aneurysm location on PICA segments did not predict outcomes (Fig 1B), though there was a trend toward better outcomes in patients with anterior medullary segment aneurysms (P = .08).
Univariate analysis of suspected predicting factors for good neurologic outcomes at 1 year
Multivariate analysis of suspected predicting factors for good neurologic outcomes at 1 year
Variables for the multivariate logistic regression model were selected based on their association with clinical outcomes identified through univariate analysis. The final model incorporated the WFNS grade, the prepontine cistern filling grade and parent vessel sacrifice as predictors of outcomes. Among these, the prepontine cistern filling grade (OR 3.13; 95% CI, 1.3–9.1; P = .02) and parent vessel sacrifice (OR 5.3; 95% CI, 1.39–23.02; P = .02) were independently associated with poor neurologic outcome. These findings are summarized in Table 3 and 4 and Fig 3.

Graphic representation of neurologic outcomes based on the necessity of sacrificing the parent vessel or not, the presence of hydrocephalus requiring external ventricular drainage or not, and the shape of the aneurysm after univariate analysis. PV = parent vessel; **P < .01).
DISCUSSION
In this study, we report acceptable outcomes in patients treated for ruptured PICA aneurysm and identify predictive factors for subsequent neurologic outcomes.
Challenges in Prognosis
Although they represent only 0.5%–5% of all ruptured intracranial aneurysms, ruptured PICA aneurysms pose major treatment challenges.3,5,14 Their proximity to the brainstem and lower cranial nerves contributes to higher rates of poor neurologic outcomes compared with other intracranial aneurysms, despite similar grades of initial hemorrhage severity.3,14⇓⇓⇓-18 Additionally, the diverse locations of these aneurysms along the PICA leads to varying degrees of lower cranial nerve dysfunction and/or the need for tracheostomy, further complicating treatment strategies.3,15 Moreover, fusiform morphology, which is more common in PICA aneurysms, adds complexity to treatment.3,15,16,18 Furthermore, large clots within the posterior fossa can compress the brainstem, exacerbating the grim prognosis of these patients.
Treatment Modalities
Direct surgical manipulation of the lower cranial nerves to adequately expose and clip PICA aneurysms has repeatedly been implicated as the main cause for high rates of lower cranial nerve dysfunction in these patients.3,19,20 However, the predominance of endovascular treatment in our series, coupled with a substantial incidence of transient tracheostomies (55%), questions whether surgical intervention is the primary cause of this dysfunction. Presently, both endovascular and microsurgical treatments have demonstrated comparable outcomes, without strong evidence favoring one over the other (Supplemental Data).3,5,16,18,20 Yet the rarity of PICA aneurysms makes it difficult to conduct randomized trials to definitively compare these modalities.
In case of Fisher grade 4 subarachnoid hemorrhage that required the placement of an external ventricular drain, stent placement was intentionally avoided to minimize the risk of hemorrhagic complications associated with antiplatelet therapy. Consequently, simple coiling was prioritized whenever feasible, with parent vessel sacrifice reserved for instances where vessel preservation was not possible, particularly in the case of fusiform aneurysms. Detailed anatomic considerations that influenced the decision to preserve or sacrifice the parent artery in each case are summarized in the Supplemental Data.
Prognostic Factors
The severity of bleeding, clinically assessed by the WFNS scale, correlates with subsequent neurologic outcome.5,17,20,21 Starnoni et al5 observed no significant influence of aneurysm morphology (fusiform versus saccular) on neurologic outcome. In our series, while a trend toward worse outcomes with fusiform aneurysms was observed, it did not reach statistical significance (P = .08). Similarly, Sejkorova et al17 reported no discernible difference in neurologic outcomes between proximal and distal PICA aneurysms.
Our findings also revealed that fusiform aneurysms were more likely to necessitate parent vessel sacrifice (P < .001). In our series, parent vessel sacrifice was associated with poorer outcomes (P < .05).
However, despite variable distribution of fusiform-shaped aneurysms along the PICA, long-term neurologic outcomes did not significantly correlate with the location of the aneurysm. Nevertheless, there was a trend suggesting better outcomes in patients with aneurysms located in the anterior medullary segment compared with those with more distal aneurysms (P = .08). Indeed, proximal PICA aneurysms may pose a higher risk of neurologic damage due to their close proximity to lower cranial nerves and the presence of vital brainstem perforators, which precludes safe parent vessel sacrifice. Conversely, it is noteworthy that 64% of proximal aneurysms were saccular, in contrast to only 4% of more distal aneurysms. Consequently, anterior medullary segment PICA aneurysms necessitated parent vessel sacrifice in merely 22% of cases, compared with 84% in more distal locations. This likely accounts for their similar outcomes to distal aneurysms, despite their deep and anatomically challenging intracranial location.
Additionally, while not previously highlighted as a prognostic factor, our series suggests that sacrificing the parent vessel may be associated with poorer outcomes (P < .05).3,5 The high rate of parent vessel sacrifice in our series (49%) and its strong association with subsequent poor neurologic outcomes raise questions about the feasibility of performing a surgical bypass to avoid deliberate endovascular occlusion of the damaged artery in these cases. In light of these results, and with the goal of improving patient’s outcomes, practices may need to shift toward higher rates of parent vessel preservation.
Prepontine Cistern Filling as a Prognostic Indicator
Our multivariate analysis identified a strong association between the filling of the prepontine cistern and poor neurologic outcomes (P < .05). In cases of severe intracranial hemorrhage, monitoring of intracranial pressure is routinely conducted in the supratentorial compartment.22 However, despite the recognized importance of brainstem compression in posterior fossa hemorrhage, infratentorial pressure monitoring remains underutilized.6 The presence of a thick and diffuse cisternal clot has been previously identified as an independent predictor of vasospasm-related morbidity and poor outcomes after SAH.7
The presence of prepontine CSF may indicate available space in the posterior fossa, while its absence suggests brainstem compression. Prepontine CSF may reflect loco-regional intracranial pressure and the potential for anterior displacement of the brainstem by large posterior compressive clots. Conversely, its absence, whether due to being filled with blood or compressed against the clivus, reflects a lack of space in the posterior fossa and an increased risk of further brainstem compression. These findings underscore the critical need to identify additional predictors of poor neurologic outcomes in this patient population.
Relevance and Limitations of the Study
This study presents a substantial series of patients with ruptured PICA aneurysms treated primarily with endovascular techniques, achieving acceptable outcomes. It is the first to suggest an association between persistent prepontine CSF and favorable neurologic outcomes in this context. However, the retrospective design and limited sample size restrict definitive conclusions, underscoring the necessity for further prospective studies. Additionally, the high rate of parent vessel sacrifice likely contributes to poor neurologic outcomes, although these are comparable to existing literature. The lack of multicollinearity between prepontine cistern filling and parent vessel sacrifice strengthens the multivariate analysis results. Additionally, while MRI could offer valuable insight into parenchymal damages related to prepontine CSF absence, it was not systematically available in this retrospective study as it was reserved for severe cases with delayed awakening. In the acute phase, CT remains the primary technique, and despite its lower sensitivity compared with MRI, CT grading is likely more practical and widely applicable in these patients.
CONCLUSIONS
Ruptured PICA aneurysms present major challenges due to their rarity and intricate nature. Their close anatomic proximity with vital structures such as the lower cranial nerves and the brainstem, the high prevalence of fusiform dissecting aneurysms, and the subsequent frequent need for parent vessel sacrifices contribute to considerable morbidity following both surgical and endovascular treatments. Our study identifies prepontine cistern filling as a key prognostic indicator of neurologic outcomes. Additionally, the requirement for sacrificing the parent vessel emerges as a factor contributing to poorer neurologic prognoses. These findings highlight the importance of advancing our understanding of PICA aneurysms to refine treatment approaches and enhance patient care.
Acknowledgments
We extend our sincere thanks to Hugues Pellerin for his valuable assistance in double-checking the statistical analysis of this article. His expertise ensured the accuracy and reliability of our results, contributing to the quality of our work.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received August 28, 2024.
- Accepted after revision October 20, 2024.
- © 2025 by American Journal of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.