
Abstract
BACKGROUND AND PURPOSE: Patients with autosomal dominant polycystic kidney disease (ADPKD) develop cysts in the kidneys, liver, spleen, pancreas, prostate, and arachnoid spaces. In addition, spinal meningeal diverticula have been reported. To determine whether spinal meningeal diverticula are associated with ADPKD, we compared their prevalence in subjects with ADPKD with a control cohort without ADPKD.
MATERIALS AND METHODS: Subjects with ADPKD and age- and sex-matched controls without ADPKD undergoing abdominal MRI from the midthorax to the pelvis from 2003 to 2023 were retrospectively evaluated for spinal meningeal diverticula by 4 blinded observers. The prevalence of spinal meningeal diverticula in ADPKD was compared with that in control subjects, using t tests and correlated with clinical and laboratory data and MR imaging features, including cyst volumes and cyst counts.
RESULTS: Identification of spinal meningeal diverticula in ADPKD (n = 285, median age, 47; interquartile range [IQR], 37–56 years; 54% female) and control (n = 285, median age, 47; IQR, 37–57 years; 54% female) subjects had high interobserver agreement (pairwise Cohen κ = 0.74). Spinal meningeal diverticula were observed in 145 of 285 (51%) subjects with ADPKD compared with 66 of 285 (23%) control subjects without ADPKD (P < .001). Spinal meningeal diverticula in ADPKD were more prevalent in women (98 of 153 [64%]) than men (47 of 132 [36%], P < .001). The mean number of spinal meningeal diverticula per affected subject with ADPKD was 3.6 ± 2.9 compared with 2.4 ± 1.9 in controls with cysts (P < .001). The median volume (IQR, 25%–75%) of spinal meningeal diverticula was 400 (IQR, 210–740) mm3 in those with ADPKD compared with 250 (IQR, 180–440) mm3 in controls (P < .001). The mean spinal meningeal diverticulum diameter was greater in the sacrum (7.3 [SD, 4.1] mm) compared with thoracic (5.4 [SD, 1.8] mm) and lumbar spine (5.8 [SD, 2.0] mm), (P < .001), suggesting that hydrostatic pressure contributed to enlargement.
CONCLUSIONS: ADPKD has a high prevalence of spinal meningeal diverticula, particularly in women.
ABBREVIATIONS:
- ADPKD
- autosomal dominant polycystic kidney disease
- IQR
- interquartile range
SUMMARY
PREVIOUS LITERATURE:
Schievink and Torres first reported spinal meningeal diverticula in 3 women with ADPKD being evaluated for headache, visual blurring aggravated by upright positioning, and low CSF pressure. Since then, there have been additional reports of spinal CSF leaks related to spinal meningeal diverticula in subjects with ADPKD. Asymptomatic spinal meningeal diverticula have also been reported in patients with ADPKD, all of whom were women. Așik et al reported more and larger cysts in 50 subjects with ADPKD compared with 37 controls without ADPKD and correlated the number and size of spinal meningeal diverticula with a headache severity score.
KEY FINDINGS:
Spinal meningeal diverticula are observed in 51% of patients with ADPKD on abdominal MRI, which is 2.2 times greater than that in a control population without ADPKD, (P < .001) and 1.8 times more common in women (98 of 153 [64%]) than men (47 of 132 [36%], P < .001).
KNOWLEDGE ADVANCEMENT:
Spinal meningeal diverticula are prevalent in subjects with ADPKD and should be included in the differential diagnosis of headache in ADPKD, especially when the headache is exacerbated or provoked by upright posture.
Autosomal dominant polycystic kidney disease (ADPKD) is characterized by multiorgan cystic (eg, kidney, liver) and noncystic (eg, pericardial, pleural) fluid accumulations.1⇓⇓⇓⇓⇓–7 Although most ADPKD imaging focuses on the kidneys, the spine is within the abdominal field of view, enabling the evaluation of nerve roots. Patients with ADPKD are known to develop intracranial arachnoid cysts.8⇓⇓–11 We have also noticed that spinal meningeal diverticula appear to be more prevalent in patients with ADPKD, and there have been multiple case reports.12⇓⇓⇓⇓⇓–18
Spinal meningeal diverticula, also known as nerve root cyst or perineural cyst, are focal fluid-filled outpouchings along the nerve root that directly communicate with the subarachnoid space and are covered with arachnoid and dura mater. The etiology is unknown, but increased prevalence in connective tissue disorders and spinal injuries has been reported.19⇓–21 One hypothesis is that inflammation and a ball valve mechanism between the nerve root sheath and subarachnoid space result from pulsatile hydrodynamic forces on the CSF.21 Most spinal meningeal diverticula are asymptomatic, though the clinical presentation can include headache exacerbated by upright posture,12,14,16,17 low back pain,22⇓⇓–25 sciatic pain,23⇓–25 leg weakness,23⇓–25 bowel and bladder dysfunction,23⇓–25 claudication,23,24 and sacral insufficiency fractures.26 Spinal meningeal diverticulum formation may also be associated with idiopathic intracranial hypertension,27 in which there is elevated intracranial pressure in the absence of hydrocephalus or mass lesions. Additionally, spinal meningeal diverticula can also be associated with spontaneous spinal CSF leaks, with CSF flowing directly into the surrounding epidural space (type 2 CSF leak) or flowing into an aberrant connection between the subarachnoid space and an adjacent paraspinal vein (type 3 CSF leak), resulting in spontaneous intracranial hypotension.28⇓–30
In this STrengthening the Reporting of OBservational studies in Epidemiology checklist–guided study, we identified the prevalence of spinal meningeal diverticula in subjects with ADPKD compared with age- and sex-matched control subjects without ADPKD to determine whether these spinal meningeal diverticula are also associated with ADPKD.
MATERIALS AND METHODS
Study Design and Populations
This retrospective, cross-sectional study of existing data and images acquired from 2003 to 2023 is compliant with the Health Insurance Portability and Accountability Act (HIPAA) and was approved by the Weill Cornell Medicine Institutional Review Board. We retrospectively analyzed 285 patients with ADPKD and 285 age- and sex-matched control subjects without ADPKD. All subjects with ADPKD were enrolled in the Rogosin PKD Repository (https://clinicaltrials.gov/study/NCT01988038), signed informed consent, and underwent MR imaging as outpatients. The requirement for informed consent was waived for analysis of existing data from control patients.
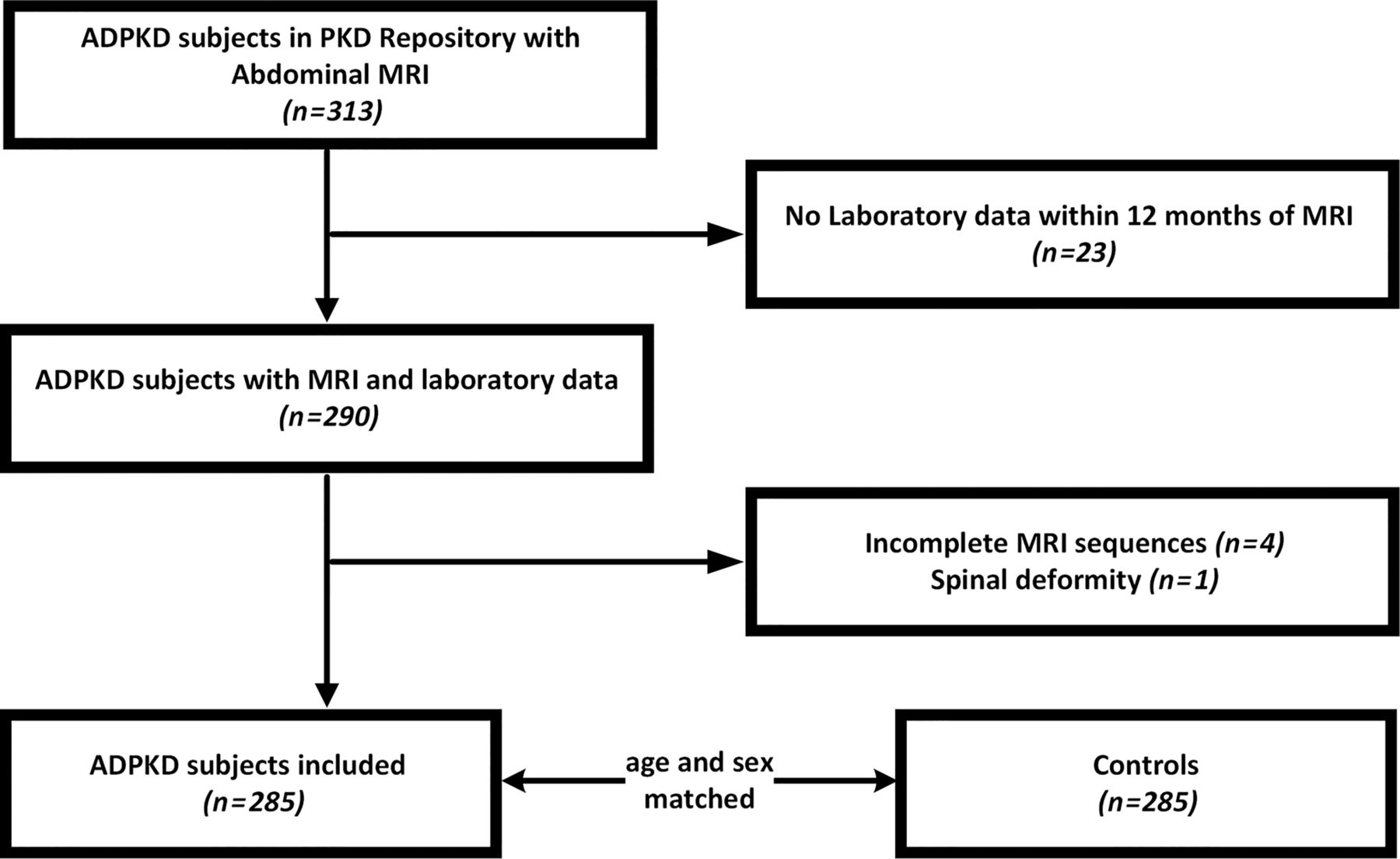
Inclusion criteria for subjects with ADPKD were the following: 1) a diagnosis of ADPKD based on the Pei-Ravine criteria,31 and 2) MRI with T2-weighted images covering from midthorax extending below the kidneys. Exclusion criteria were the following: 1) medical conditions associated with spinal meningeal diverticula including connective tissue disorder or spinal deformity, 2) an incomplete T2 MRI, and 3) laboratory data unavailable within 12 months of the MRI (Fig 1). For each patient with ADPKD, we identified age- (within 2.5 years) and sex-matched control patients without ADPKD, connective tissue disorder, or spinal deformity from the PACS with contemporaneous examination dates.

Patient flow chart.
Data Extraction
ADPKD and control subjects’ demographic information, clinical data, laboratory data, and genetic data were extracted from the PKD Repository and the electronic medical records for the date closest to the MRI date. We analyzed MRI reports prepared prospectively at the time of imaging to obtain data on kidney, liver, and spleen volumes, cyst counts/fractions, pancreatic cysts, prostate cysts, seminal megavesicles, and pleural effusions.
Image Acquisition
MRI examinations without contrast enhancement were obtained at 1.5T or 3T using a body array coil with the parameters shown in the Online Supplemental Data. Pulse sequences used for this analysis were coronal and axial T2-weighted single-shot FSE (Signa family; GE Healthcare) or HASTE (Magnetom Skyra; Siemens).
Image Analysis
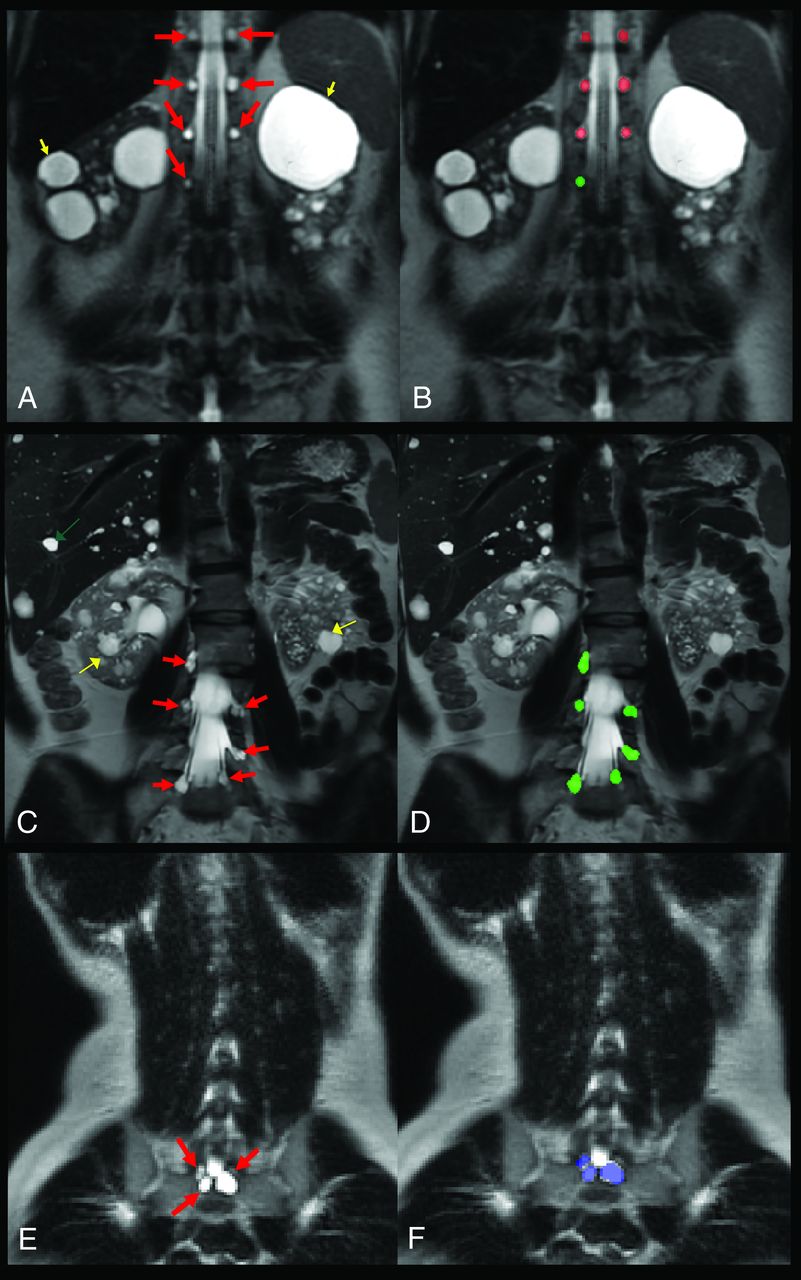
Axial and coronal T2 MR images were analyzed by 4 independent, experienced observers (U.S., X.Y., X.L., M.R.P.) blinded to the patient information. Observers independently counted the number of spinal meningeal diverticula present in each subject. Disagreements were resolved by consensus. Spinal meningeal diverticula were defined as present when there was a well-defined T2 bright signal corresponding to fluid intensity along the course of the normal nerve root on T2-weighted images at least doubling the normal nerve root diameter. For size measurement and region distribution, one of the observers (U.S.) annotated spinal meningeal diverticula on coronal images using ITK-SNAP software, Version 3.8.0 (www.itksnap.org) (Fig 2).

Coronal T2-weighted single-shot FSE images in 3 typical patients with ADPKD including a 60-year-old woman with T10-12 spinal meningeal diverticula bilaterally (red arrows, A) and an L1 spinal meningeal diverticulum on the right (B) in red (thoracic) and green (lumbar); C, A 46-year-old woman with lumbar spinal meningeal diverticula (red arrows, C) with a corresponding annotation (D) in green for L2 (right), L3 (bilateral), L4 (left), and L5 (bilateral); E, a 28-year-old female with sacral spinal meningeal diverticula (red arrows, F) in blue. Also, note renal cysts (yellow arrows) and liver with multiple cysts (green arrow).
Descriptive Statistics
For normally distributed continuous variables (assessed by the Shapiro-Wilk test), means (SDs) were reported. For non-normal distributions, median and interquartile range (IQR) were reported. Frequency and percentage were calculated for categoric variables.
For 2-group matched continuous variables, a paired t test was used to assess the statistical significance. For multigroup continuous variables, the ANOVA was used to assess statistical significance. For categoric variables, a χ2 or Fisher exact test was used to assess statistical significance, depending on sample size. Interobserver agreement for identifying spinal meningeal diverticula and the number of spinal meningeal diverticula were assessed using the pair-wise Cohen κ and intraclass correlation coefficients, respectively.
Regression Models
Bivariate analysis was used to estimate the correlation between the presence of spinal meningeal diverticula and age, sex, height, weight, body mass index, body surface area, blood pressure, blood urea nitrogen level, creatinine level, estimated glomerular filtration rate, albumin level, aspartate transaminase and alanine transaminase levels, height-adjusted total kidney volume, height-adjusted total liver volume, height-adjusted total spleen volume, number of renal cysts, number of hemorrhagic renal cysts, number of liver cysts, number of pancreatic cysts, pleural effusion, severe headache, and PKD genotype. The variables that had significance (ie, P < .05) were used in a multivariable linear regression analysis to assess their effect after adjusting for the other variables. The analysis was performed using GraphPad Prism software, Version 10.2.0392 (GraphPad Software).
RESULTS
Abdominal MRI results were available in 285 subjects with ADPKD (median age, 47 [IQR, 3–56] years; women 54%, white 84%) and a control group without ADPKD controlled for age and sex (Fig 1 and Online Supplemental Data).
As expected, the ADPKD group had higher diastolic blood pressure, blood urea nitrogen and creatinine levels, a lower estimated glomerular filtration rate, and higher height-adjusted total kidney volume, height-adjusted total liver volume, height-adjusted total spleen volume, number of liver cysts, and number of kidney cysts (Online Supplemental Data). Information on race was available for more patients with ADPKD compared with control patients, reflecting the willingness of subjects with ADPKD to provide this information when enrolling in the Rogosin PKD Repository. This availability resulted a higher number of subjects with unknown race in the control population (Online Supplemental Data).
Indications for MRI in the control subjects included inflammatory bowel disease follow-up (n = 99), indeterminate lesion (n = 82), pain (n = 51), cancer follow-up (n = 23), liver disease (n = 15), pancreatitis (n = 7), hematuria (n = 4), small bowel obstruction follow-up (n = 2), endometriosis (n = 1), and uterine leiomyomas (n = 1).
Prevalence of Spinal Meningeal Diverticula in ADPKD
Spinal meningeal diverticula were identified in 51% of subjects with ADPKD compared with 23% of controls (Online Supplemental Data; P < .001). In the ADPKD group, 64% of all women had spinal meningeal diverticula compared with 36% of men (P < .001). In the control subjects, 31% of women had spinal meningeal diverticula compared with 14% of men (P = .001) (Online Supplemental Data).
In the ADPKD group, subjects with cysts had a mean of 3.6 (SD, 2.9) cysts per subject, which was 50% greater than the mean number in controls, (2.4 [SD, 1.9], P < .001). The median spinal meningeal diverticulum volume was 400 (IQR, 210–740) mm3 in subjects with ADPKD with spinal meningeal diverticula compared with 250 (IQR, 180–440) mm3 in controls (P < .001). The mean spinal meningeal diverticulum diameter was 6.6 (SD, 3.4) mm in subjects with ADPKD compared with 6.1 (SD, 2.6) mm in the control subjects (P = .06). Spinal meningeal diverticula were more prevalent in the sacrum compared with lumbar or thoracic spine locations (P < .001) (Online Supplemental Data). Large cysts (>10 mm) were more prevalent in the ADPKD group than the control group (35/285 [12.3%] versus 6/285 [2.1%]) (P < .001) (Online Supplemental Data). The mean diameter of spinal meningeal diverticula was largest in the sacrum, (7.3 [SD, 4.1) mm, compared with the lumbar (5.8 [SD, 2.0] mm) and thoracic (5.4 [SD, 1.8] mm) spine, (P < .001) (Fig 3 and Online Supplemental Data).

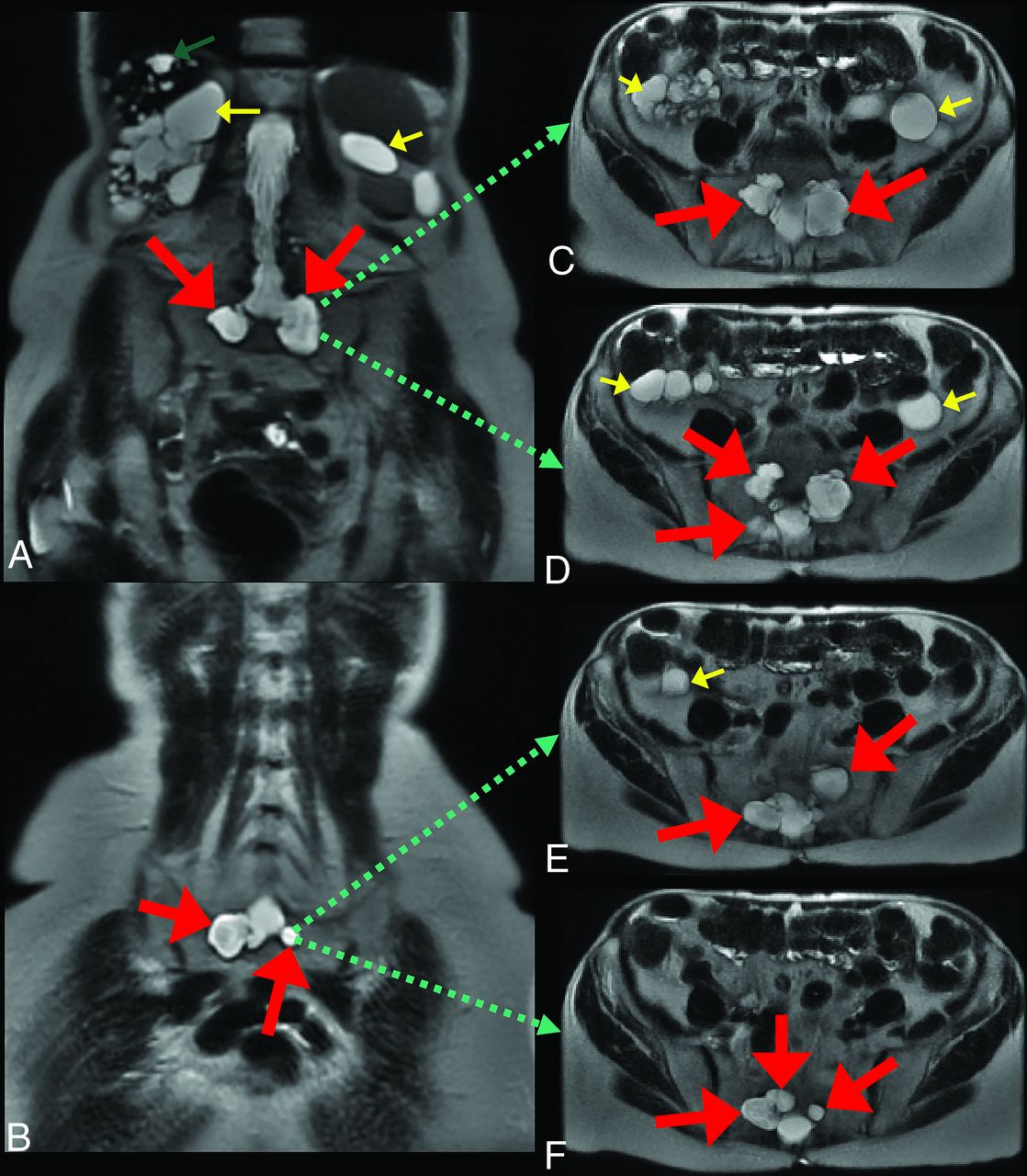
A 73-year-old woman with ADPKD reporting a remote history of severe headache lasting 2 weeks. A and B, coronal, and C–F, sequential, axial T2-weighted single-shot FSE images show multiple large sacral spinal meningeal diverticula (red arrows). Also, note renal cysts (yellow arrows) and liver with multiple cysts (green arrow).
As expected, the ADPKD group had a higher prevalence of pancreatic cysts, seminal megavesicles, and midline prostate cysts than the control group, as previously reported.5,6 Serum albumin and aspartate transaminase levels were slightly higher in those with ADPKD compared with the control group; however, these values were within normal limits for both groups.
Interobserver Variability
Interobserver agreement for the presence of spinal meningeal diverticula was high, with a pair-wise Cohen κ = 0.74. Interobserver agreement for the number of spinal meningeal diverticula in each subject was excellent, with an intraclass correlation coefficient = 0.95.
Genotype
Among patients with ADPKD with either a PKD1 (n = 187/245 = 76.3%) or PKD2 (n = 58/245 [23.7%]) mutation, 95 of 187 (51%) with PKD1 mutations had spinal meningeal diverticula compared with 30 of 58 (52%) with PKD2 mutations (Online Supplemental Data; P = .9). The prevalence of truncating mutations in PKD1 was similar in those with and without spinal meningeal diverticula.
Correlation with Laboratory and Imaging Parameters
The presence of spinal meningeal diverticula on MRI in subjects with ADPKD was significantly correlated with female sex and severe headache by bivariate analysis (Online Supplemental Data). The presence of spinal meningeal diverticula negatively correlated with height, weight, body mass index, body surface area, blood urea nitrogen level, creatinine level, height-adjusted total kidney volume, height-adjusted total spleen volume, the number of renal cysts, and the number of hemorrhagic renal cysts. However, a multivariate analysis, including sex, height, weight, body mass index, body surface area, blood urea nitrogen level, creatinine level, height-adjusted total kidney volume, height-adjusted total spleen volume, the number of renal cysts, the number of hemorrhagic renal cysts, severe headache, and spinal meningeal diverticula, showed that sex was the only parameter to retain statistical significance (Table), though the number of hemorrhagic cysts was of borderline significance.
| Variable | Coefficients | 95% CI (Asymptotic) | P Value |
|---|---|---|---|
| Intercept | –0.18 | –5.84–5.48 | .94 |
| Male sex | –0.31 | –0.481 to −0.14 | <.001b |
| Height (cm) | 0.91 | –4.944–6.76 | .76 |
| Weight (kg) | 0.003 | –0.051–0.06 | .92 |
| Body mass index (kg/m2) | –0.01 | –0.107–0.09 | .83 |
| Body surface area (m2) | –0.24 | –5.473–4.98 | .92 |
| Blood urea nitrogen (mg/dL) | 0.004 | –0.003–0.01 | .31 |
| Creatinine (mg/dL) | –0.07 | –0.161–0.02 | .11 |
| Total kidney volume/height (mL/m) | –0.00003 | –0.0001–0.00004 | .40 |
| Spleen volume/height (ml/m) | –0.0007 | –0.001 to 0.0003 | .17 |
| Number of renal cysts | 0.00002 | –0.0002 to 0.0002 | .85 |
| Number of hemorrhagic renal cysts | –0.0009 | –0.0019 to 0.0000267 | .06 |
| Severe headache | 0.093 | –0.02503–0.2107 | .12 |
a Including parameters with P value < .05 on bivariate analysis (model P value = < .001).
↵b Significant P value.
Multivariate analysis for the presence of spinal meningeal diverticula in patients with ADPKDa
Clinical Effects and Progression of Spinal Meningeal Diverticula
There was more frequent reporting of severe headache in the ADPKD group with spinal meningeal diverticula (68/145 [47%]) compared with those without spinal meningeal diverticula (48/140 [34%], P = .03). Headache prevalence data were not systematically available for the control group. None of the 145 subjects with ADPKD with spinal meningeal diverticula reported any other symptoms attributable to these cysts. The Online Supplemental Data show the number of spinal meningeal diverticula observed for each of the 285 subjects with ADPKD, showing no relationship with patient age.
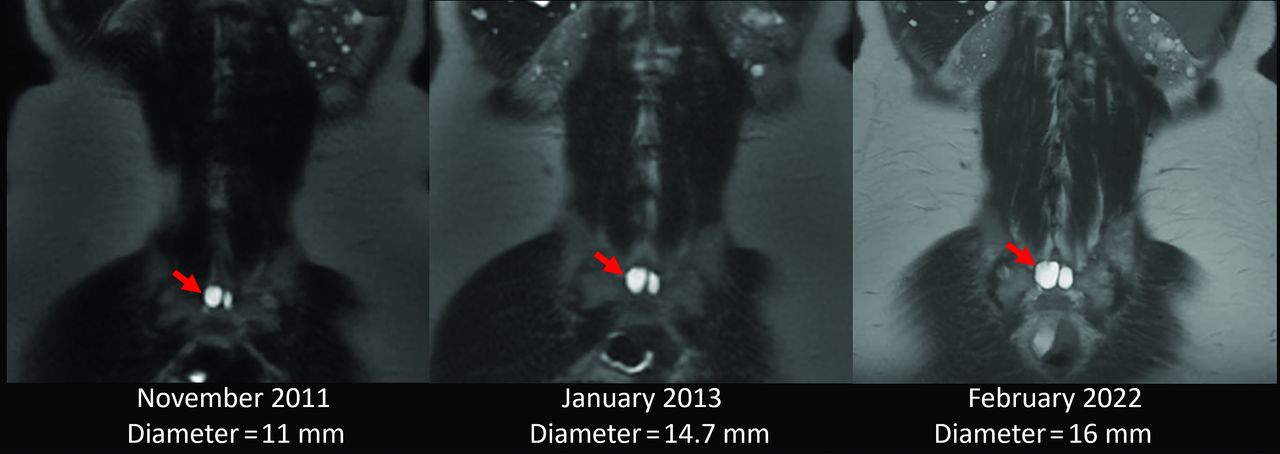
There were 50 subjects with ADPKD who had 10+ years of MRI scans, median follow-up = 11.2 years [IQR, 10.6–13.1]). The Online Supplemental Data show that the characteristics of these patients with ADPKD with 10+ years of follow-up are similar to those in the entire ADPKD population. One of these subjects with ADPKD with follow-up initially had no spinal meningeal diverticula but developed a 5.8-mm spinal meningeal diverticulum. Subjects with ADPKD with follow-up also included 32 subjects with a spinal meningeal diverticulum on the initial MRI. For these 32 affected subjects with ADPKD with follow-up (Online Supplemental Data), the mean number of cysts on their first scan, 3.3 [SD, 2.7], was similar to the mean number of cysts on the most recent scan, 3.2 [SD, 2.6] (P = .4). However, the mean diameter of the largest cyst increased from 8.1 [SD, 3.2] mm on the first scan to 8.9 [SD, 3.7] mm (P = .01) on the most recent scan (Fig 4). The Online Supplemental Data show the growth of spinal meningeal diverticula from the first scan compared with the most recent scan in all subjects with ADPKD with 10+ years follow-up.

Coronal T2 single-shot FSE images spanning 10 years in a 44-year-old woman with ADPKD showing a right sacral spinal meningeal diverticulum (red arrows), which increased in short-axis diameter from 11 to 16 mm.
DISCUSSION
These data from 285 subjects with ADPKD and matched control patients show that the prevalence of spinal meningeal diverticula was 51%, which was 2.2 times higher in those with ADPKD than the control group. In a multivariable model, women with ADPKD were more likely than men to have spinal meningeal diverticula. Furthermore, spinal meningeal diverticula were larger and more numerous in subjects with ADPKD, and the total spinal meningeal diverticular volume was 60% greater compared with controls.
In 1997, Schievink and Torres12 reported spinal meningeal diverticula in 3 women with ADPKD being evaluated for headache, visual blurring aggravated by upright positioning, and low CSF pressure. Symptoms in 1 patient resolved after surgical repair of an 8-cm thoracic spinal meningeal diverticulum. Additional reports of spinal CSF leaks related to spinal meningeal diverticula in subjects with ADPKD also showed resolution of headache after surgical repair or an epidural blood patch.14,16 Although Kranz et al,32 in 2013, reported no difference in the prevalence of spinal meningeal diverticula between patients with spontaneous intracranial hypotension and controls, asymptomatic spinal meningeal diverticula have also been reported in patients with ADPKD, all of whom were female.15,18 Our data confirm the findings of Așik et al,17 who reported more and larger cysts in 50 subjects with ADPKD compared with 37 controls without ADPKD. In that study, the number and size of spinal meningeal diverticula correlated with a headache severity score. However, the ADPKD population in that study was not randomly selected, the prevalence of spinal meningeal diverticula was not reported, and the authors did not report a female predominance.17
Our data in control subjects without ADPKD, which showed that spinal meningeal diverticula were twice as prevalent in women compared with men, is in agreement with Burdan et al,33 who evaluated spinal perineural cysts among Eastern European patients, and Langdown et al,34 who reported that these cysts were seen in about 70% of women. Female prevalence was also observed in a study of neurosurgical patients in which 102 (84%) of 122 patients who underwent percutaneous sealing of perineurial cysts were women.35
Spinal meningeal diverticula, also known as nerve root cysts or perineural cysts, are hypothesized to arise at sites of dural weakness and are more prevalent in connective tissue disorders, suggesting meningeal connective tissue weakness as a risk factor.19,20 Other proposed mechanisms include nerve root inflammation, followed by fluid accumulation, arachnoidal proliferation, and communications between dilated sheaths and the subarachnoid space expanding under the influence of pulsatile hydrodynamic CSF forces.21 The association of spinal meningeal diverticula with ADPKD supports the concept that ADPKD is a more generalized connective tissue disorder. The observation of more and larger sacral spinal meningeal diverticula, compared with the lumbar and thoracic regions, suggests that the increased hydrostatic pressure in the sacral region while the patient is upright may promote cyst formation. This concept is also supported by reports of spinal meningeal diverticula occurring with a type 2 CSF leak (ruptured spinal meningeal diverticulum) or type 3 CSF leak (an aberrant connection between the subarachnoid space and an adjacent paraspinal vein), often presenting as postural headache indicating spontaneous intracranial hypotension.28⇓–30
The strengths of this study are the large, unselected population of subjects with ADPKD in the Rogosin PKD Repository with an age- and sex-matched control group and multiobserver analysis blinded to the patient data. We further strengthened the study by excluding all subjects with known connective tissue disorders, debilitating spinal deformities, and incomplete MRI sequences that may have confounded the analysis.
Limitations of this study include retrospective image analysis and failure of MRI sequences to cover the entire thoracic or cervical spine. This feature may have biased the study toward underreporting the true spinal meningeal diverticula prevalence. True blinding was also not possible due to ADPKD status being apparent on the images. None of the patients in this study underwent a procedure to measure CSF pressure or for cyst drainage or excision, which precluded histopathologic evaluation.
CONCLUSIONS
These findings indicate that spinal meningeal diverticula are prevalent in subjects with ADPKD, particularly in women, and should be included in the differential diagnosis of headache in ADPKD, especially when the headache is exacerbated or provoked by upright posture.
Acknowledgments
We acknowledge the support of the Rogosin Institute, the Department of Radiology of Weill Cornell Medicine, and the Weill Cornell Clinical and Translational Science Center (National Institutes of Health grant: UL1TR002384), and the Shaw Foundation.
Footnotes
This work was supported by the Rogosin Institute, the Department of Radiology of Weill Cornell Medicine, Weill Cornell Clinical and Translational Science Center (National Institutes of Health grant: UL1TR002384), and the Shaw Foundation.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received April 29, 2024.
- Accepted after revision July 1, 2024.
- © 2025 by American Journal of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.