
Abstract
BACKGROUND AND PURPOSE: Overuse of CT-based cerebrovascular imaging in the emergency department and inpatient settings, notably CTA of the head and neck for minor and nonfocal neurologic presentations, stresses imaging services and exposes patients to radiation and contrast. Furthermore, such CT-based imaging is often insufficient for definitive diagnosis, necessitating additional MR imaging. Recent advances in fast MRI may allow timely assessment and a reduced need for head and neck CTA in select populations.
MATERIALS AND METHODS: We identified inpatients or patients in the emergency department who underwent CTAHN (including noncontrast and postcontrast head CT, with or without CTP imaging) followed within 24 hours by a 3T MRI study that included a 2.5-minute unenhanced multicontrast sequence (NeuroMix) and a 5-minute intracranial time of flight MRA) during a 9-month period (April to December 2022). Cases were classified by 4 radiologists in consensus as to whether NeuroMix and NeuroMix + MRA detected equivalent findings, detected unique findings, or missed findings relative to CTAHN.
RESULTS: One hundred seventy-four cases (mean age, 67 [SD, 16] years; 56% female) met the inclusion criteria. NeuroMix alone and NeuroMix + MRA protocols were determined to be equivalent or better compared with CTAHN in 71% and 95% of patients, respectively. NeuroMix always provided equivalent or better assessment of the brain parenchyma, with unique findings on NeuroMix and NeuroMix + MRA in 35% and 36% of cases, respectively, most commonly acute infarction or multiple microhemorrhages. In 8/174 cases (5%), CTAHN identified vascular abnormalities not seen on the NeuroMix + MRA protocol due to the wider coverage of the cervical arteries by CTAHN.
CONCLUSIONS: A fast MR imaging protocol consisting of NeuroMix + MRA provided equivalent or better information compared with CTAHN in 95% of cases in our population of patients with an acute neurologic presentation. The findings provide a deeper understanding of the benefits and challenges of a fast unenhanced MR-first approach with NeuroMix + MRA, which could be used to design prospective trials in select patient groups, with the potential to reduce radiation dose, mitigate adverse contrast-related patient and environmental effects, and lessen the burden on radiologists and health care systems.
ABBREVIATIONS:
- CTAHN
- CTA of the head and neck including noncontrast and delayed postcontrast head CT with or without CTP
- ED
- emergency department
- ICH
- intracranial hemorrhage
- LOS
- length of stay
- MRA
- time-of-flight MRA
- NeuroMix
- unenhanced multicontrast MR brain sequence
- ST
- slice thickness
SUMMARY
PREVIOUS LITERATURE:
The use of CT angiography of the head and neck has been expanding, increasing patient risks and putting strain on radiologists and the medical system. Fast MR brain protocols have been developed at multiple institutions, initially for pediatrics but more recently for adults. In adults, such fast MR brain protocols are primarily compared with conventional MRI protocols, demonstrating significant time savings without significant loss in diagnostic quality. No studies to date have compared a fast MR brain protocol with typical CTAHN protocols for adult patients presenting with acute neurologic symptoms.
KEY FINDINGS:
A fast MR imaging protocol consisting of unenhanced multi-contrast NeuroMix and TOF-MRA sequences detected all structural and almost all vascular findings seen with CTAHN, while detecting unique findings in over a third of cases. Cervical vascular findings were rare, and were missed due to the NeuroMix+MRA protocol’s anatomic coverage.
KNOWLEDGE ADVANCEMENT:
Noncontrast fast MR brain protocols such as NeuroMix+MRA may diagnostically substitute for CTAHN protocols. Significant cervical vascular findings were rare in our population. The current findings can inform the development of prospective trials to evaluate whether fast MR protocols can replace CTAHN in defined patient populations.
Increased use of CT in the emergency department (ED) and inpatient settings places growing demands on imaging services resources.1⇓-3 These include increased health care costs and radiologist burnout,4 as well as patient safety concerns related to radiation and contrast-related risks.5,6 This concern is particularly evident in the setting of minor and nonfocal neurologic symptoms,7 in which CTA of the head and neck including noncontrast and delayed postcontrast head CT with or without CTP (CTAHN) is increasingly performed.8,9 This preference for broad CTA use may be partly due to increased ordering by non-MD advanced practice providers.10,11
CTAHN studies typically consist of thousands of images requiring lengthy evaluations by radiologists. Nonetheless, these studies often yield insufficient diagnostic information,2,10 leading to subsequent evaluation with MRI. In this study, we retrospectively assessed the performance of fast MR protocols based on a 2.5-minute unenhanced multicontrast MR brain sequence (NeuroMix)12 acquired alongside standard MRI sequences and performed within 24 hours of a contrast-enhanced CTAHN in patients with acute neurologic presentations to better understand the benefits and challenges of a “fast MR first” approach in select patient groups.
MATERIALS AND METHODS
Patient Population
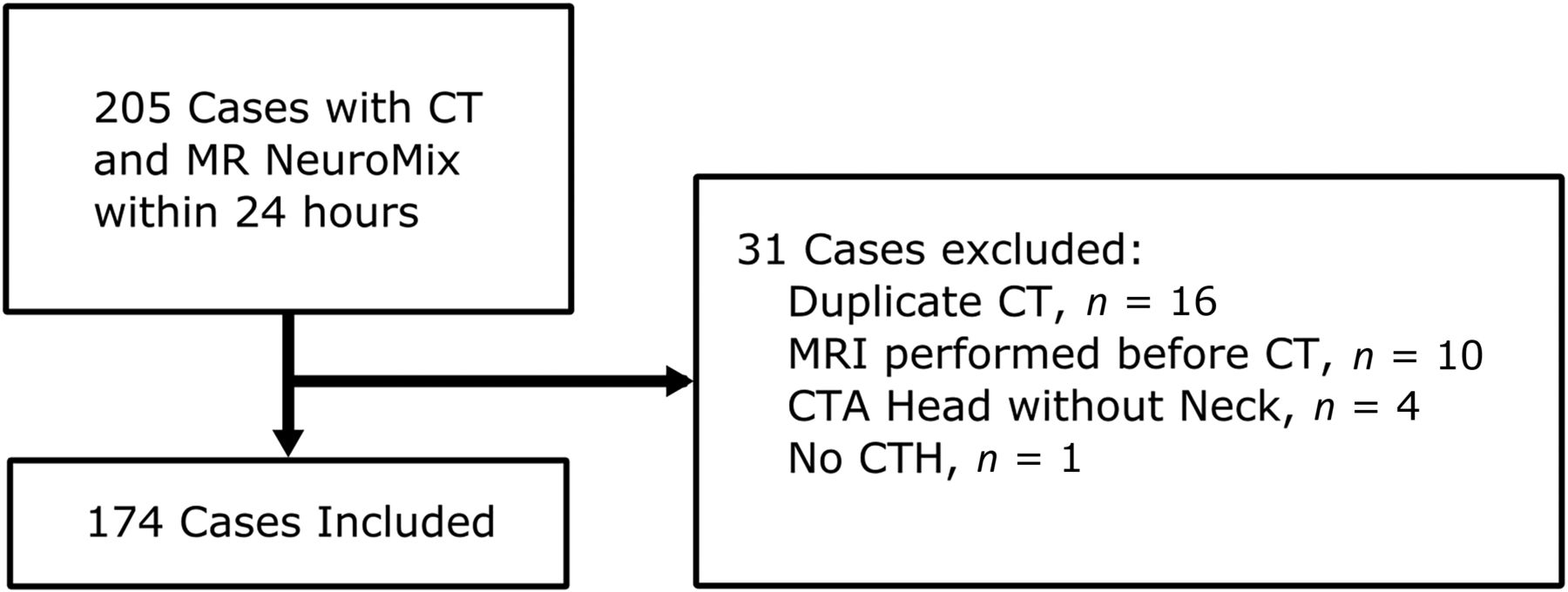
We performed an institutional review board–approved, retrospective review of data from a single institution. Sequential inpatients and ED patients who underwent an MRI that included NeuroMix12 and intracranial time-of-flight MRA (MRA) within 24 hours of CTAHN with or without CTP between April and December 2022 were identified by querying our electronic medical record (Fig 1). All CTAHN studies included noncontrast head CT and 5-minute postcontrast head CT. For patients with multiple CT studies in the 24 hours before MRI, only the examination closest in time to the MRI was included. Imaging time was defined as time between the first and last acquired image. For stroke codes, this time included the delay after initial noncontrast head CT to communicate the presence of hemorrhage and the determination to proceed to CTAHN.

Flow chart shows a collection of cases by initial inclusion criteria, subsequent exclusion, and total cases that underwent analysis.
Chart review was performed to collect demographic data and presenting symptoms. Presenting symptoms were categorized by ABCD2 risk stratification:13 ABCD+ (focal weakness or speech disturbance), non-ABCD (sensory loss, dizziness, altered mental status, gait abnormality, headache, or vision loss), or other (acute trauma or follow-up examinations). In cases in which a stroke code was initiated, we recorded the presenting NIHSS score and whether thrombolytic therapy was ultimately administered.
Imaging Protocols
CTAHN was performed on 2 scanners (Revolution; GE Healthcare; Somatom Force; Siemens). Parameters were as follows: noncontrast and postcontrast CT: slice thickness (ST) = 0.625–0.75 mm, dual-energy = 80 and 150 kV(peak); CTA: ST = 0.625–0.75 mm, 80 kVp; CTP: ST = 10 mm, 70 kVp. Typical dose-length product was 3000−5000 mGy-cm. The typical iodinated contrast dose was 100 mL. CTP studies had split-dose contrast administration.
3T MRI was performed on 1 of 3 scanners (Premier (n = 2) and MR750 (n = 1, GE Healthcare). NeuroMix is a fast segmented EPI and single-shot fast spin-echo acquisition with 5 standard and 3 optional tissue contrasts,12 requiring 2.5 minutes for 5-mm ST, 1–1.3 mm in-plane resolution, and 2 selected optional contrasts. Standard contrasts are axial EPI DWI, T1-weighted FLAIR, T2-weighted and T2 FLAIR single-shot fast spin-echo, and T2*-weighted EPI. Selected optional contrasts included sagittal T1-weighted 3D EPI using an ST of 1.2 mm and axial SWI 3D EPI using an ST of 2.5 mm (Fig 2). Intracranial noncontrast MRA parameters were 3 slabs, TR/TE = 22/2.6 ms, ST = 1.2 mm, imaging duration approximately 5 minutes. While cervical MRA was occasionally performed, we assessed only the intracranial MRA information because this was common to all MR imaging studies.

NeuroMix sequence compared with CT in a 67-year-old woman with a history of prior strokes and worsened left-sided weakness and dysarthria. Graded as unique NeuroMix information regarding acute infarct and microhemorrhages. A, Axial noncontrast head CT without focal hypoattenuation or a CTP deficit (not shown). B, DWI with diffusion restriction in the right corona radiata (arrow). C, Axial reconstruction of NeuroMix sagittal 3D T1-weighted acquisition. T2-weighted (D) and T2 FLAIR (E) images show confluent subcortical white matter hyperintensity. F, SWI shows a right parietal microhemorrhage (arrowhead).
Data and Statistical Analysis
Four radiologists reviewed all studies in consensus. Abnormalities were categorized as structural (eg, infarct, hemorrhage, microhemorrhage) or angiographic (eg, >50% arterial stenosis, occlusion, aneurysm, dissection). Comparisons were made to determine whether CT and MR protocols provided equivalent or unique diagnostic information. For example, when CT imaging with CTP suggested acute infarct that was confirmed by MRI and limited to the same vascular territory, this suggestion was considered equivalent. Otherwise, DWIs positive for acute infarcts were recorded as unique MR information if the findings on CT were not visible, equivocal, or favored to be chronic. Conversely, if CT suggested an acute infarct that was disproven on MRI, this suggestion was considered unique MRI information. Results are presented for the entire cohort, as well as the following subgroups: patients who presented as stroke codes, as nonstroke codes, with a presenting NIHSS of 0, 1−6, or >6, and with focal weakness or speech disturbance (ABCD+), and those with other symptoms (non-ABCD). CIs were calculated using the modified Wald method.14
RESULTS
Two hundred five matched CT and MR cases met our initial criteria, of which 31 were excluded, resulting in analysis of 174 cases (Fig 1). The primary reason for excluding individual cases was when a patient had >1 CTAHN study within the 24-hour period before MRI (n = 16). Most (75%) cases were from the ED, 56% were women, 47% self-identified as white, and the mean age was 67 years (range, 20−102 years). The most common presentation was focal weakness (16%), followed by speech disturbance (15%), sensory abnormality (13%), dizziness (13%), and altered mental status (11%) (Table 1).
Patient demographics and presenting symptomsa
CTAHN, NeuroMix, and MRA sequences were interpretable in all cases. MR studies were acquired a mean of 6.5 (SD, 4.5) hours after the CT study. Five MR studies were prematurely halted due to patient factors, though after acquisition of NeuroMix and MRA. The mean imaging time, as defined in the Materials and Methods section, was 12 (SD, 5) minutes for CTAHN without CTP, 17 (SD, 6) minutes for CTAHN with CTP, and 33 (SD, 10) minutes for conventional MRI.
Overall, 43 cases (25%) had normal findings or had irrelevant incidental findings on both MRI and CTAHN, while another 10 cases (6%) demonstrated obviously chronic findings. The remaining 121 patients (70%) had potentially relevant diagnostic information on either CTAHN or NeuroMix + MRA, 98 with structural findings and 59 with angiographic findings (Tables 2⇓–4). NeuroMix-only and NeuroMix + MRA protocols were deemed equivalent or better than CTAHN in 71% and 95% of patients, respectively (Table 5; Online Supplemental Data). Unique findings were seen on NeuroMix alone and NeuroMix + MRA in 35% and 36% of patients, respectively, most commonly acute infarction not identified on CT (Fig 3) or findings seen only on SWI (Fig 4). Unique findings were seen on CTAHN in 8/174 cases (5%) compared with NeuroMix + MRA, with findings of high-grade carotid bifurcation (n = 3) or proximal vertebral artery (n = 5) stenosis outside the MRA field of view.

Unique NeuroMix information (pontine infarct) in a 62-year-old man presenting with 1 day of left-sided weakness and tingling. A, Axial noncontrast CT without structural abnormality. CTA and perfusion findings were also unremarkable. B, NeuroMix axial DWI shows diffusion restriction within the right pons compatible with acute infarct (arrow). C, Conventional axial DWI similarly shows the acute right pontine infarct (arrow).

Two cases with unique and useful NeuroMix information on SWI. A and B, A 49-year-old woman presenting with worsening multifocal pain, weakness, and numbness not confined to a particular neurovascular territory. A, Axial noncontrast CT head shows a heterogeneously hyperattenuating lesion in the left parieto-occipital white matter (arrow). B, Axial NeuroMix SWI shows blooming of this lesion (arrow) as well as multiple lesions not evident on CT (arrowheads), consistent with multiple cavernous vascular malformations. C and D, A 74-year-old woman with transient left facial droop and dysarthria. C, Axial noncontrast CT without notable structural abnormality. D, Axial NeuroMix SWI shows central-predominant foci of susceptibility (arrowheads) suspicious for hypertensive microhemorrhages.
Imaging findings
Structural findingsa
Angiographic findingsa
CTAHN and NeuroMix MR comparison
In most of our cases (106/174, 61%), a stroke code prompted CTAHN. Ten patients (6%) received IV thrombolysis. No patients underwent thrombectomy. Seventy-five percent had an NIHSS score of ≤6. Of note, one-half (34/68) of all nonstroke code cases also included CTP. Intracranial hemorrhage (ICH) was noted in 23 cases, all identified by both CT and NeuroMix. NeuroMix-based SWI detected a superimposed pattern of multiple microhemorrhages suggesting cerebral amyloid angiopathy or chronic hypertension in 4 cases.
DISCUSSION
We compared MR studies that included NeuroMix and MRA sequences with a recently performed CTAHN (including noncontrast head CT, often with CTP, and delayed postcontrast head CT) in patients with acute neurologic presentations. In 95% of these cases, the fast MR-based protocol provided equivalent or better information relative to CTAHN, detecting unique structural findings such as acute infarcts or microhemorrhages in more than one-third of cases, while detecting all intracranial vascular findings. NeuroMix + MRA missed a total of 8 (4.6%) findings, all of which were extracranial vascular findings not included in the MRA field-of-view; of these, only 3 (1.7%) had a vascular finding that would change management (ie, high-grade carotid stenosis). This result suggests that there may be a role for fast MR-first protocols in patients with acute neurologic presentations, which could be further assessed with prospective evaluation.
CTAHN has undergone dramatic growth in recent years,8,9 being generally fast and widely available. However, CTAHN as a first study for patients with neurologic symptoms exposes patients to ionizing radiation and iodinated contrast. Lengthy evaluation times for CTAHN studies, concurrent with increasing demands for rapid report turn-around-times15 and overall rising volumes,2 increases pressure on radiologists and contributes to workload and burnout.4 The number of studies without relevant findings is also increasing,9 possibly due to less emphasis on physical examination and clinical judgment and more reliance on physician extenders in the ED.10 MRI allows faster and more definitive reporting of acute ischemic stroke due to DWI. If timely MRI access can be facilitated, a “fast MR-first” approach for certain acute neurologic presentations may benefit multiple stakeholders with more definitive and potentially lower-cost imaging. Additionally, an unenhanced NeuroMix + MRA protocol would avoid contrast material injection, saving imaging time, avoiding contrast reaction or extravasation, and reducing environmental/water pollution downstream from sites with high concentrations of imaging centers.16,17
We found that NeuroMix + MRA provided unique information in more than one-third of cases relative to CTAHN.18 This estimate is likely conservative, because we did not specifically consider the clinical value of a DWI with negative findings, which allows more definitive management decisions and might facilitate more rapid patient discharge. These advantages must be weighed against a low rate of missed cervical vascular findings, because some pathways suggest a benefit of early intervention in patients with transient ischemic attack or stroke and >50% carotid bifurcation stenosis.19,20 This issue could be largely mitigated if noncontrast MRA coverage extended from the circle of Willis to the carotid bifurcation or with nonemergent follow-up imaging of neck vessels. The benefit of imaging of the vertebral arteries for posterior circulation symptoms21,22 is less clear, given the lack of benefit of vascular intervention23 over medical therapy.24 Depending on the clinical scenario, NeuroMix-based protocols may be variably appropriate, and this observational study can serve as a foundation to explore their application to different patient populations with prospective trial designs.
Long wait and acquisition times have limited traditional MR examinations in the ED setting. Abbreviated MRI examinations have been validated in the pediatric setting to expeditiously evaluate hydrocephalus25 and trauma,26,27 though CT retains some advantages over MRI in trauma, depending on the clinical scenario.28 Accelerated protocols often rely on gradient recalled echo-only echo-planar imaging29⇓⇓⇓-33 to provide multicontrast imaging. NeuroMix,12 with both gradient recalled echo–EPI and single-shot fast spin-echo–based acquisitions, has decreased susceptibility artifacts at the skull base. A recent study using a deep learning–augmented fast MR protocol was shown to be effective in patients presenting with strokelike symptoms relative to standard MRI.34 NeuroMix + MRA had an imaging time comparable to the average CTAHN (noncontrast head CT, head and neck CTA, +/− CTP, delayed contrast-enhanced head CT) in our cohort: NeuroMix + MRA at 7.5-minutes “gradient-on-time,” CTAHN without CTP at 12 minutes, and CTAHN with CTP at 17 minutes. This lengthy CT time is largely driven by the number of stroke codes in our cohort and the associated required care team communications. CT imaging time will likely be reduced if fewer stroke codes are included, and prospective trials comparing CT and NeuroMix-based protocols will need to account for total imaging time (room time, order-to-report, or presentation-to-disposition) to determine the feasibility and utility of NeuroMix-based protocols. Nevertheless, we believe that there is roughly similar table time for these 2 approaches, with the potential of further speeding up the MRA study, which was not optimized for fast imaging but was rather our routine clinical sequence. Other issues, including access to MRI, would need to be addressed in a prospective trial.
Triaging patients to NeuroMix + MRA over CTAHN may reduce the length of stay (LOS), a critical metric and driver of imaging. EDs are structured to provide short door-to-CT times generally15 and for trauma and stroke particularly.35 Conventional MRI is viewed as increasing the LOS,36 but having dedicated ED MR scanners,37 protocols,30,31 and workflows has been shown to result in overall decreased hospital LOS.36 One study showed equivalent ED LOS between CT and MR work-up to evaluate hip fracture, with more definitive management after MR.38 A recent model analysis suggests that specialized MRI is the most cost-effective evaluation of patients with dizziness in the ED.7 Nevertheless, patient screening, scanner availability, and staffing are potential barriers to expedite MR access in the ED setting, even when MR is the more appropriate study, though access to MRI improves when individual patient examinations are shortened.39
A NeuroMix + MRA fast imaging protocol is not meant to replace comprehensive MRI, and this study was not designed to evaluate these differences. Nevertheless, NeuroMix was acquired alongside conventional MRIs, allowing an evaluation of NeuroMix findings compared with conventional MR protocols in our cohort. We found that 9% of cases had findings on conventional MRI that were not evident or not fully evaluated on NeuroMix + MRA. In 8/16 (50%) cases, this issue was related to nondetection or incomplete characterization of enhancing lesions, which is expected, given the noncontrast nature of the fast MR protocol. Other discrepancies included new information in 6/16 cases derived from arterial spin-labeling perfusion imaging, while in 2/16 cases, subtle punctate infarcts were seen on comprehensive 3-mm DWI but not on 5-mm NeuroMix DWI. NeuroMix has the option of acquiring images at a thinner ST (3 or 4 mm) with slightly increased imaging duration so that the extra imaging time must be weighed against the need to visualize tiny infarcts. If a fast MRI-first protocol is implemented, the protocol may enable more informed decision-making regarding the need for further imaging evaluation, such as CTAHN, neck ultrasound, and/or conventional MRI. There is a risk that ordering providers may rely excessively on the fast MRI without understanding potential limitations, and education around protocols will be important.
Several patients in our cohort were found to have acute ICH. Noncontrast CT remains a bedrock of evaluating patients for acute ICH, but clinically relevant hemorrhage can be equally well or better assessed with MRI using gradient-echo and SWI.40,41 No cases of ICH were missed by NeuroMix. In 4 cases of CT-evident ICH, SWI revealed a microhemorrhage pattern consistent with hypertension or cerebral amyloid angiopathy, thereby adding important clinical information. A theoretic concern exists regarding the delay in ICH diagnosis due to differences in access to MRI versus CT, and this issue should be monitored when assessing fast MR-first protocols in patients with mild neurologic presentations.
Our study has several limitations. First, requiring 2 imaging examinations within 24 hours selects for follow-up MRIs based on nondefinitive CTAHN (work-up bias), but a short time window between examinations is necessary to limit the changes that can occur between examinations based solely on time. Additionally, cases for which a negative CTAHN was considered definitive or cases with symptoms or CTAHN findings too severe to have warranted or tolerated additional short-interval MRI were not included. Furthermore, at our institution, this selection criterion excludes patients who undergo thrombectomy and therefore is biased against cases of large-vessel occlusion. This design was meant to enrich less severe presentations, with the assumption that prospective NeuroMix + MRA trials would target patients with minor neurologic symptoms. For example, meta-analyses have shown a high negative predictive value for large-vessel occlusion using clinical symptoms, such as NIHSS <4.42 Another limitation is that we were unable to retrospectively quantify wait time for CT or MRI or overall room time, though this quantification would not have much meaning given that initial time-sensitive triage was performed with CT. While imaging times for NeuroMix + MRA (7.5 minutes) and full CTAHN (17 minutes, inclusive of noncontrast stroke code communication and IV thrombolysis decision-making) were comparable, patients can typically access CT scanners more quickly than MR scanners due to differences in patient screening and availability of scanners. To fully understand these important timing considerations requires a prospective trial.
CONCLUSIONS
In our patient population, NeuroMix + MRA provided equivalent or better information compared with CTAHN in 95% of cases, detecting unique findings in 36% of cases. These results, along with comparable acquisition times, indicate that NeuroMix + MRA can be considered as an alternative to CTAHN in patients with acute neurologic presentations. Future prospective work is needed to confirm this hypothesis and define appropriate patient populations for such a protocol.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received March 4, 2024.
- Accepted after revision June 11, 2024.
- © 2024 by American Journal of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.