Abstract
BACKGROUND: The effective treatment for patients with acute ischemic stroke (AIS) with cervical internal carotid pseudo-occlusion (cICA-PO) requires comprehensive research on the safety and outcomes of endovascular thrombectomy (EVT). However, there are limited data available, highlighting the need for further research to ensure better treatment strategies and improve the quality of care for these patients.
PURPOSE: This study aims to assess the management and outcomes in this population group compared with patients with true carotid occlusion.
DATA SOURCES: Following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines, a comprehensive systematic review was conducted by using PubMed, Embase, Web of Science, and Scopus from database inception to November 2023.
STUDY SELECTION: The size of the included studies ranged from 16 patients to 146 patients. Through the 4 full-text articles, a total of 259 patients were collected. We compared outcomes between patients with cICA-PO compared with patients with true carotid occlusions undergoing EVT due to AIS. We excluded studies with patients with carotid pseudo-occlusion without stroke, review articles, duplicate studies, overlapped data that included the same patients presented in another included study, case reports, case series with fewer than 5 patients, and meeting abstracts that did not contain the outcomes of interest. We did not pose any limitations regarding sample size or patient characteristics.
DATA ANALYSIS: We utilized the R statistical software (V.4.3.1; R package meta) to conduct the analysis of all the data obtained. We calculated the OR for binary variables, and the corresponding 95% CI. To synthesize the data, random-effect models, as well as forest plots were generated to visually represent the synthesis of the data. Additionally, we assessed heterogeneity by using Cochran Q and I2 tests. A P value < .05 for the Q statistic or I2 more than 50% suggests notable heterogeneity. Based on a small number of studies (<10), the assessment of publication bias could not be reliably performed.
DATA SYNTHESIS: This meta-analysis encompassed data from 4 studies. Patients with cICA-PO and AIS who underwent EVT (n = 135) exhibited lower rates of functional independence (OR = 0.35; 95% CI, 0.20–0.61; P < .001) compared with patients with true occlusions (n = 103), as well as successful recanalization rates (OR = 0.39; 95% CI, 0.20–0.74; P = .004). In addition, the cICA-PO group experienced higher mortality and symptomatic intracranial hemorrhage (sICH) compared with the group with true carotid occlusions (OR = 2.62; 95% CI, 0.21–7.24; and OR = 2.23; 95% CI, 1.00–4.95; P = .049, respectively).
LIMITATIONS: Individual patient data were not available. Studies were a retrospective design and some of the studies had small sample sizes. The included studies in our meta-analysis did not exclude patients with tandem occlusions that might influence the results of the comparison.
CONCLUSIONS: Compared with patients with true carotid occlusion, the cICA-PO group with AIS undergoing EVT presented poor outcomes with lower functional independence and successful recanalization, as well as higher sICH and mortality rates.
ABBREVIATIONS:
- AIS
- acute ischemic stroke
- cICA-PO
- cervical ICA pseudo-occlusion
- EVT
- endovascular thrombectomy
- sICH
- symptomatic intracranial hemorrhage
SUMMARY
PREVIOUS LITERATURE:
Pseudo-occlusion of the cervical internal carotid artery (cICA-PO) refers to an isolated occlusion of the intracranial internal carotid artery (ICA) that appears as an extracranial ICA occlusion on CTA or digital subtraction angiography because of blockage of distal contrast penetration by a stagnant column of unopacified blood. Previous studies have found that patients with cICA-PO compared with patients with true cICA occlusion have a lower chance of successful recanalization, lower rates of favorable functional outcome (mRS 0–2) and mortality, likely due to the heavier clot burden in cICA-PO cases.
KEY FINDINGS:
This meta-analysis of four studies, encompassing 135 patients, demonstrated endovascular thrombectomy (EVT) in patients with acute ischemic stroke (AIS) with cICA-PO with consistent results with lower rates of successful recanalization and worse functional outcome (mRS 0–2) compared with those with true cICA occlusion. EVT in patients with AIS with cICA-PO was also found to have higher risks of symptomatic intracranial hemorrhage (sICH) and mortality compared with patients with AIS with true cICA occlusion.
KNOWLEDGE ADVANCEMENT:
To improve outcomes in these patients, it is essential to optimize the vascular imaging modalities to help differentiate between cICA-PO and true ICA occlusion in acute settings. This will allow for better decision-making and tailored preparation for EVT procedures based on the actual level of the ICA occlusion.
Cervical ICA pseudo-occlusion (cICA-PO) refers to an apparent occlusion of the cervical ICA on CT angiography or digital subtraction angiography due to unopacified stagnant blood flow in a patent artery caused by a distal intracranial occlusion. It is often mistaken for true occlusions on CT angiography due to their similar imaging findings. Pseudo-occlusion occurs in 6%–15% of patients with acute ischemic stroke (AIS),1 and according to a study published in 2022, suggests that cICA-PO is associated with an increased risk of reperfusion failure and poor outcome after endovascular thrombectomy (EVT) compared with true occlusion.2 Even though ICA pseudo-occlusion is a fairly common scenario, existing studies have been performed only in small population sizes, requiring further evidence to evaluate the role of this imaging finding in patients with AIS. Therefore, the purpose of this systematic review and meta-analysis is to assess the management and outcomes of patients who underwent EVT with pseudo-occlusion compared with true occlusion in the setting of acute stroke.
MATERIALS AND METHODS
Search Strategy
For this systematic review and meta-analysis, a systematic review of the literature was conducted within Nested Knowledge Autolit software version 1.46 (Nested Knowledge), by using PubMed, Embase, Web of Science, and Scopus from database inception to November 2023. Based on each database, different combinations of possible keywords and/or Medical Subject Headings terms were used for that purpose. Keywords and Medical Subject Headings terms included carotid pseudo-occlusion or pseudo-occlusion, stroke. The full search strategy is provided in the Online Supplemental Data. Moreover, we did an extensive manual search through the references of the included articles to retrieve any missed papers. This study is reported following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline (Fig 1).3

PRISMA flowchart detailing the literature review process.
Screening Process and Eligibility Criteria
We included all original studies fulfilling our predetermined population, intervention, comparator, and outcomes approach. The population was patients with carotid pseudo-occlusion in the setting of acute stroke, the intervention was EVT, and the control group was patients with true occlusion in the presence of AIS.
We excluded studies with patients with carotid pseudo-occlusion without stroke, review articles, duplicate studies, overlapped data that included the same patients presented in another included study, case reports, case series with fewer than 5 patients, and meeting abstracts that did not contain the outcomes of interest. We did not pose any limitations regarding sample size or patient characteristics.
Data Extraction
Three authors (M.T., T.M., and K.V.) performed the title and abstract screening against the predefined criteria. This was followed by a full-text screening of any retained studies of the first screening step. In both stages, the senior author (D.F.K.) was consulted to resolve any conflicts in the decisions.
Data extraction was also performed with AutoLit software. The extracted data included study characteristics, baseline data of included patients, and outcomes of interest. Two authors (M.T. and T.M.) independently completed the extraction, which was subsequently evaluated for consensus by a third author (S.G.).
Risk of Bias
To evaluate the potential bias in the observational, nonrandomized studies included in our analysis, we employed the Risk of Bias in Nonrandomized Studies of Interventions tool.4 The tool assesses 7 distinct domains of bias, including confounding, selection of participants in the study, classification of interventions, deviations from intended interventions, missing data, measurement of outcomes, and selection of the reported result. Our assessment yielded an overall judgment of the risk of bias, which we categorized as low, moderate, serious, or critical.
Statistical Analysis
We utilized the R statistical software (V.4.3.1; R package meta, R Foundation for Statistical Computing) to conduct the analysis of all the data obtained. We calculated the OR for binary variables, and the corresponding 95% CI. To synthesize the data, random-effect models, as well as forest plots were generated to visually represent the synthesis of the data. Additionally, we assessed heterogeneity by using Cochran Q and I2 tests. A P value < .05 for the Q statistic or I2 more than 50% suggests significant heterogeneity. Based on a small number of studies (<10), the assessment of publication bias could not be reliably performed.
RESULTS
Search and Screening Results
The search strategy yielded a total of 304 studies; after removing duplicates the remaining 156 studies were further screened. There was a total of 7 studies selected for the title and abstract screening. Eventually, 4 studies were determined to satisfy our inclusion criteria with the appropriate report of outcomes of interest and data were then extracted from these studies.
Study Characteristics and Risk of Bias
All 4 included studies used a retrospective design. The size of the included studies ranged from 16 patients to 146 patients. Through the 4 full-text articles, a total of 259 patients were collected.
Moderate risk of bias was found in 3 of the 4 articles and was determined in 1 study to have a critical risk of bias. Domains of most concerns across studies were: bias due to the selection of participants and measurement outcomes. Patient characteristics, including age, sex, comorbidities, presence of tandem occlusions, site of occlusion, management, and baseline NIHSS score, are detailed in the Online Supplemental Data.
Outcomes
Functional Independence.
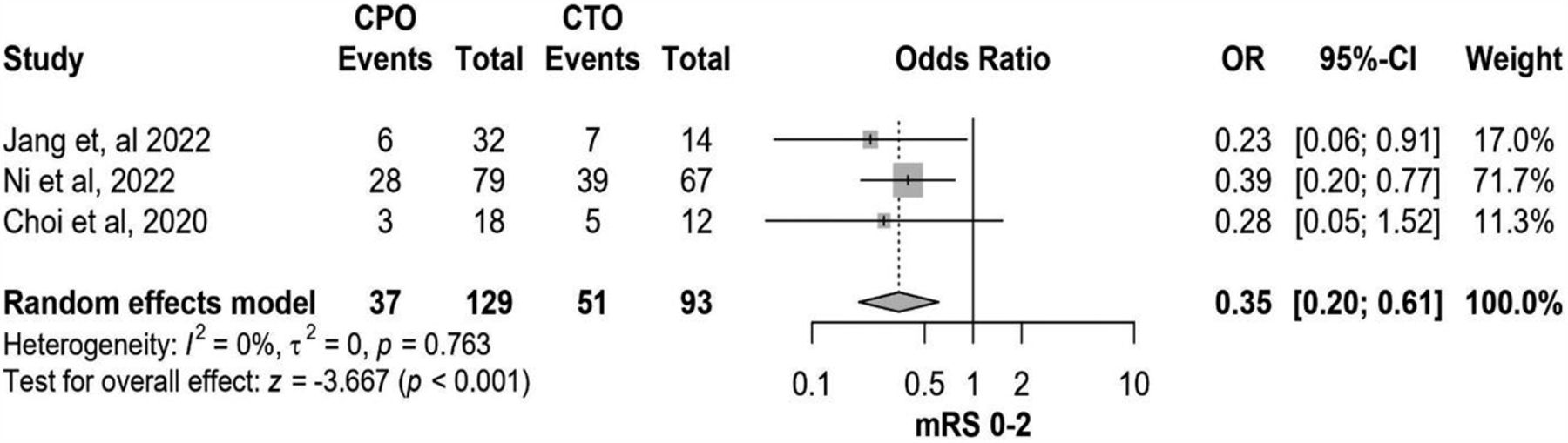
Three studies involving 129 patients compared the rates of mRS 0–2 at 90 days between patients with cICA-PO and those with true occlusion undergoing EVT for AIS. The analysis indicated a lower rate of functional independence in the cICA-PO group (OR = 0.35; 95% CI, 0.20–0.61; P < .001). Notably, no heterogeneity was observed among these studies (I2 = 0%, P = .763; Fig 2).

Forest plot of rates of functional independence.
Recanalization Rate
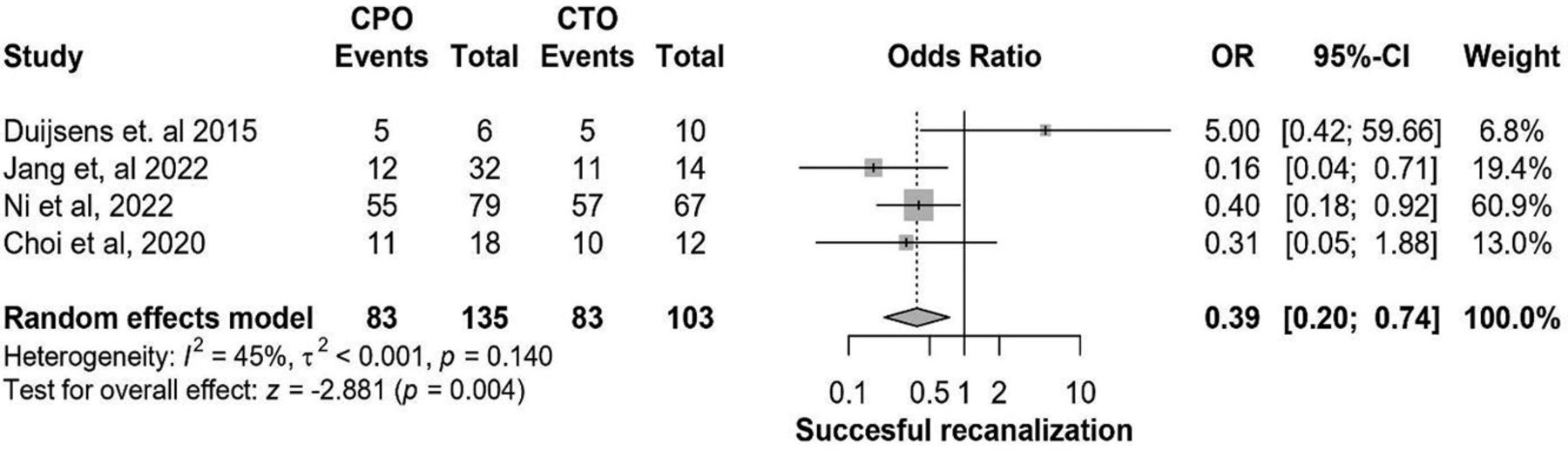
The meta-analysis of 4 studies, encompassing 135 patients, evaluated successful recanalization (TICI 2b–3) in EVT-treated patients. The analysis revealed lower rates of recanalization in the cICA-PO group compared with the true carotid occlusion group (OR = 0.39; 95% CI, 0.20–0.74; P = .004). No significant heterogeneity was detected among these studies (I2 = 45%; P = .140; Fig 3).

Forest plot of rates of successful recanalization.
Symptomatic Intracranial Hemorrhage
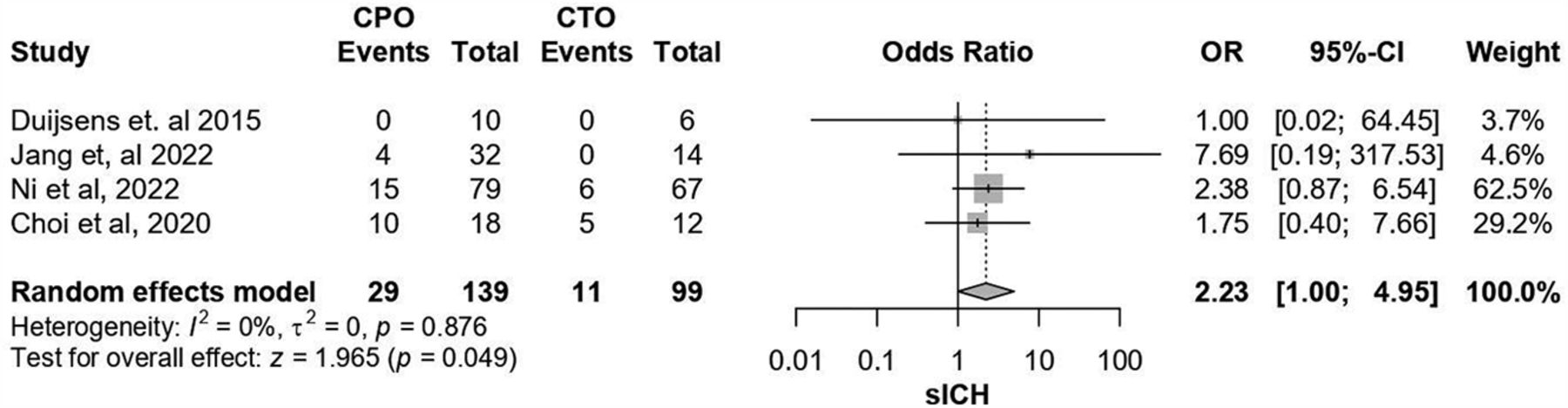
In 4 studies involving 139 patients, >rates of symptomatic intracranial hemorrhage (sICH) were compared between the 2 groups. Patients with cICA-PO undergoing EVT exhibited significantly higher rates of sICH compared with those with true carotid occlusions (OR =2.23; 95% CI, 1.00–4.95; P = .049). No heterogeneity was observed among these studies (I2 = 0%; P = .876; Fig 4).

Forest plot of rates of sICH.
Mortality
Four studies involving 135 patients compared mortality rates between the 2 groups. It was found that patients with cICA-PO had a significantly higher mortality rate compared with those with true carotid occlusion (OR = 2.62; 95% CI, 0.21–7.24), with no heterogeneity noted among these studies (I2 = 0%; P = .001; Fig 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of rates of mortality.
DISCUSSION
Our systematic review and meta-analysis included 4 studies with a total of 259 patients, and our results indicated that EVT in patients with AIS with cICA-PO had lower rates of successful recanalization and favorable functional outcome (mRS 0–2 at 90 days) compared with patients with AIS with true cervical ICA occlusion. Furthermore, EVT in patients with AIS with cICA-PO were found to have higher risks of sICH and mortality compared with patients with AIS with true cervical ICA occlusion. These results were consistent with the results of the studies by Jang et al5 and Ni et al,2 which have larger sample sizes than the rest of the included studies.6,7
The phenomenon of cICA-PO refers to the presence of an unopacified column of blood in the cICA that might be perceived as extracranial ICA obstruction, while it is in fact an isolated intracranial ICA occlusion causing stagnation of blood in the patent extracranial portion of the ICA.8,9 Pseudo-occlusion and true occlusion are 2 different conditions that may only share the common imaging finding of lack of ICA filling. It is very difficult to differentiate with absolute certainty cICA-PO from true occlusion of the cICA on CT angiography.1 This imposes a crucial challenge in clinical practice from both decision-making and technical standpoints. In terms of decision-making, patients with AIS with cICA-PO presenting in the late window of EVT might be deemed not to be good candidates for EVT given the falsely overestimated time needed to overcome the perceived extracranial cervical ICA occlusion. From the technical standpoint, differentiating pseudo-occlusion from true occlusion of the extracranial ICA might influence the choice of the EVT material including guiding sheaths, percutaneous transluminal angioplasty balloons, and distal access catheters.1
The lower rate of successful recanalization in patients with cICA-PO compared with true cervical ICA occlusion is likely due to the heavier clot burden in case of cICA-PO,2,10,11 and lower rates of successful recanalization are associated with lower rates of favorable functional outcome (mRS 0–2) and mortality.12 Furthermore, the heavier clot burden with large clots in the distal ICA segment in cICA-PO might be associated with poor filling of the collateral circulation,10 which is known to be associated with higher rates of poor functional outcomes.13,14 Therefore, it is pivotal to optimize the vascular imaging modalities to enable differentiation between cICA-PO and true ICA occlusion in acute settings, which will allow for better decision-making and tailored preparation for EVT procedure according to the actual level of the ICA occlusion. Moreover, these findings indicate the need for further investigation into the underlying causes of these deficient outcomes.
According to the literature, cICA-PO can also be compared with distal ICA due to their similar disease process and imaging presentations. However, certain imaging characteristics may suggest pseudo-occlusion on CTA, such as an ipsilateral occluded intracranial ICA bifurcation (carotid T-occlusion) and good contrast filling of the carotid bulb followed by a gradual contrast decay. Furthermore, the imaging presentation of isolated distal ICA occlusion demonstrates patency of the cervical ICA carotid terminus. The results between these 2 groups indicated that cICA-PO is also associated with poorer outcomes.1,8,15,16
Strengths and Limitations
Our meta-analysis provides a larger sample of patients to provide a comprehensive analysis of all published literature regarding the outcomes of EVT in patients with cICA-PO in AIS. However, our study has a few limitations. First, a low number of studies met our inclusion criteria. Second, all of the studies were a retrospective design and some of the studies had small sample sizes. Therefore, this meta-analysis may contain insufficient data to allow generalization. Furthermore, access to individual patient data was not available, which resulted in restrictions on the level of analysis that could be performed. Last, it is to be noted that the included studies in our meta-analysis collected patients with and without tandem occlusions that might influence the results of the comparison. For instance, the studies by Jang et al5 and Ni et al2 reported higher percentages of tandem occlusions within the true ICA occlusion patient group compared with the patients with cICA-PO. This is a pivotal point to be taken into consideration given that the EVT outcomes might be better in patients with tandem occlusion than in patients with isolated carotid occlusion from both successful recanalization and functional independence standpoints.17
CONCLUSIONS
Patients undergoing EVT for AIS with cICA-PO have poor outcomes. This is most likely due to heavy clot burden and poor recanalization rates that lead to lower favorable functional outcomes and greater rates of mortality and sICH. The accurate and timely diagnosis of cICA-PO from true carotid occlusions is crucial as it influences the treatment and possesses a worse prognosis than true occlusion. We recommend further research should be conducted with precise definitions regarding the presence of tandem lesions as they may affect the outcomes. In addition, studies should be conducted to identify underlying causes of these poor outcomes and improve management guidelines in such settings.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- Received February 15, 2024.
- Accepted after revision March 25, 2024.
- © 2024 by American Journal of Neuroradiology