Graphical Abstract

Abstract
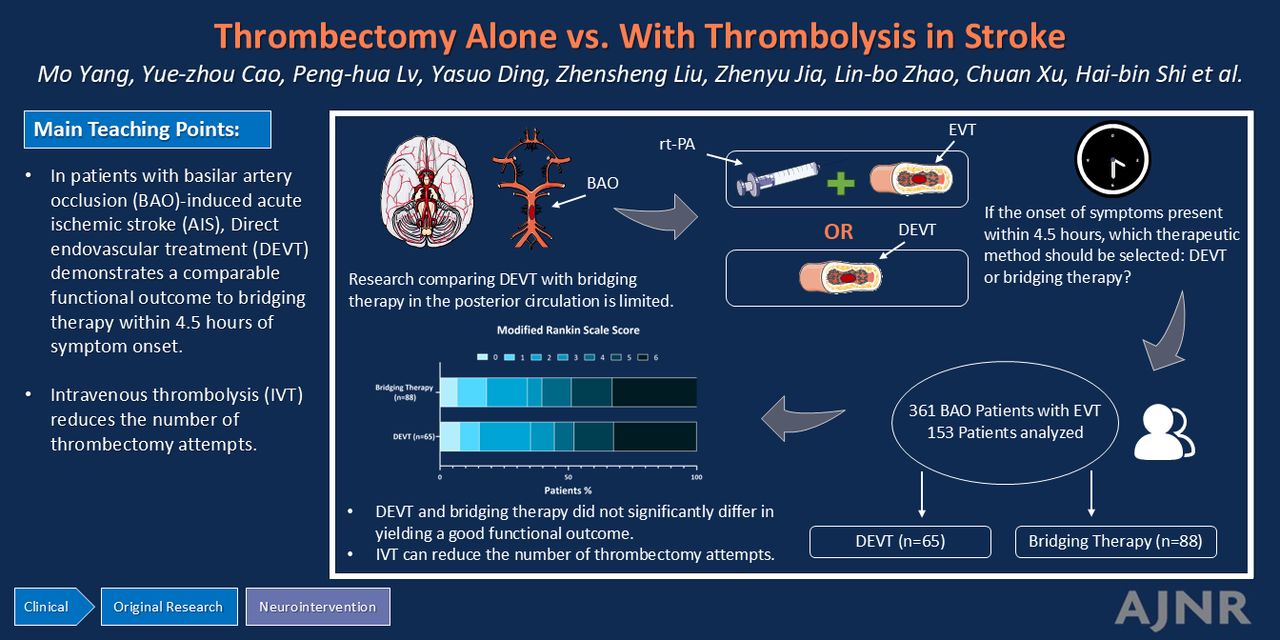
BACKGROUND AND PURPOSE: It remains unclear whether the combination of endovascular treatment (EVT) with intravenous thrombolysis (IVT) results in a more favorable functional outcome than EVT alone in managing cases of acute ischemic stroke (AIS) caused by basilar artery occlusion (BAO). Thus, this study aimed to compare the outcomes of 2 approaches—direct endovascular treatment (DEVT) and bridging therapy (IVT plus EVT)—in patients with acute BAO presenting within 4.5 hours of stroke onset.
MATERIALS AND METHODS: This multicenter retrospective cohort study included 153 patients with acute BAO presenting within 4.5 hours of stroke onset. Of these patients, 65 (42.5%) and 88 (57.5%) underwent DEVT and bridging therapy, respectively. The primary outcome was defined as good functional outcome (mRS, 0–3) at 90 days. Additionally, preoperative clinical features, thrombectomy attempts, successful reperfusion rates, incidences of symptomatic intracranial hemorrhage (sICH), and mortality were compared between the 2 groups.
RESULTS: At 90 days, the rate of good functional outcome was comparable between the DEVT (44.6%) and bridging-therapy (39.8%) groups (adjusted odds ratio [aOR], 1.12; 95% CI, 0.55–2.31; P = .753). The bridging-therapy group exhibited a lower percentage of patients requiring ≥3 attempts of stent retrieval (aOR, 0.39; 95% CI, 0.16–0.93; P = .034). Preoperative clinical features, rate of successful reperfusion, sICH, and mortality were similar between the 2 groups.
CONCLUSIONS: In patients with BAO-induced AIS, DEVT demonstrates a comparable functional outcome to bridging therapy within 4.5 hours of symptom onset, but IVT reduces the number of thrombectomy attempts.
ABBREVIATIONS:
- AIS
- acute ischemic stroke
- aOR
- adjusted odds ratio
- BAO
- basilar artery occlusion
- DEVT
- direct endovascular treatment
- EVT
- endovascular treatment
- ICAS
- intracranial atherosclerotic stenosis
- IQR
- interquartile range
- IVT
- intravenous thrombolysis
- LVO
- large-vessel occlusion
- mTICI
- modified TICI
- RCT
- randomized controlled trial
- SD
- standard deviation
- sICH
- symptomatic intracranial hemorrhage
- TOAST
- Trial of Org 10172 in Acute Stroke Treatment
SUMMARY
PREVIOUS LITERATURE:
Research comparing DEVT with bridging therapy in the posterior circulation is limited. Existing analyses from several studies have yielded inconsistent results regarding the efficacy of bridging therapy. Although several groups have suggested that bridging therapy is more effective than DEVT for patients with posterior large-vessel occlusion, multiple studies have shown no difference in clinical outcomes between DEVT and bridging therapy in patients with BAO-induced AIS. Furthermore, in previous studies comparing bridging therapy with DEVT in the posterior circulation, not all patients in the DEVT group received treatment within 4.5 hours.
KEY FINDINGS:
In patients with BAO-induced AIS, DEVT demonstrates a comparable functional outcome to bridging therapy within 4.5 hours of symptom onset, but bridging therapy reduces the number of thrombectomy attempts.
KNOWLEDGE ADVANCEMENT:
This multicenter retrospective cohort study compares the efficacies of DEVT, and bridging therapy applied within 4.5 hours of stroke onset in patients with BAO-induced AIS. Our findings do not indicate any benefit of pre-endovascular treatment bridging therapy in improving functional outcomes. Nevertheless, bridging therapy can reduce the number of thrombectomy attempts.
Intravenous thrombolysis (IVT) is currently recommended preceding endovascular treatment (EVT) for patients with acute ischemic stroke (AIS) caused by anterior circulation large-vessel occlusion (LVO),1 as indicated by a recent meta-analysis on 6 randomized controlled trials (RCTs). This meta-analysis, known as Improving Reperfusion Strategies in Ischemic Stroke, suggested that IVT should not be skipped in favor of direct endovascular treatment (DEVT) in patients with AIS caused by anterior circulation LVO.2
Regarding posterior circulation LVO, recent RCTs have affirmed that thrombectomy yields a higher percentage of individuals with good functional status at 90 days than medical therapy.3,4 However, studies directly comparing DEVT with bridging therapy in the posterior circulation are limited, a related RCT (NCT05827042) is not expected to be completed before March 2026, and existing prospective or retrospective studies have yielded incongruent conclusions.5⇓⇓⇓⇓-10 Shortly after the completion of our study, 2 guidelines for treatment of basilar artery occlusion (BAO) were published in July and August 2024.11,12 Currently, there are no recommendations on the treatment of patients with BAO scheduled for EVT who are also eligible for IVT within the 4.5-hour time window.
This study presents a multicenter retrospective cohort study comparing the efficacies of DEVT and bridging therapy within 4.5 hours of stroke onset in patients with BAO-induced AIS.
MATERIALS AND METHODS
This multicenter retrospective cohort study was approved by the local institutional ethics committee, which waived the need for informed consent from the patients due to the retrospective nature of the study. All the procedures performed in this study complied with the ethical standards of the institutional and/or national research committee and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Patient Population and Treatment
Given the variability in management protocols for vertebral artery occlusion and tandem occlusion across different stroke centers, we specifically focused on patients with isolated BAO. Individuals with BAO-induced AIS, who were treated with EVT at 4 comprehensive stroke centers between January 2018 and April 2023, were included in the study if they met the following criteria: 1) age >18 years old; 2) presentation within 4.5 hours of symptom onset for patients with basilar artery stroke; 3) AIS diagnosis based on brain imaging with documented BAO, confirmed via CT angiography, MR angiography, or digital subtraction angiography; 4) treatment with mechanical thrombectomy; and 5) a follow-up period of ≥3 months.
After diagnosing patients with BAO in the emergency department, interventional neurologists explained the condition and the associated risks of DEVT versus bridging therapy in detail to the family members. After a thorough discussion and understanding of these complexities, the family members made a decision about whether to proceed with bridging therapy. Patients whose family members consented to IVT received intravenous alteplase (0.9 mg/kg alteplase over 1 hour with a 10% initial bolus, maximum 90 mg) within 4.5 hours. EVT was applied concurrently with IVT, and these patients were subsequently enrolled in the bridging-therapy group. Those whose family members declined IVT skipped this stage and were enrolled in the DEVT group.
EVT
Thrombectomy was performed under local anesthesia or conscious sedation utilizing a large-bore aspiration device (React 68, Medtronic; ACE 60, Penumbra; 6F Sofia PLUS Catheter, MicroVention) or a reusable stent (Embotrap, Cerenovus; Solitaire FR/AB, Covidien) in combination with an aspiration catheter. In cases in which successful reperfusion was not achieved after multiple thrombectomy attempts, the neurointerventionist, at their discretion, implemented a rescue treatment, such as intra-arterial thrombolysis, balloon angioplasty, stent placement, or intra-arterial tirofiban administration.
Data Collection
We collected patient-level data encompassing demographics, medical history, clinical presentation, and procedural details. The demographic data included age, sex, medical history, and clinical presentation. Additional information comprised severity at admission, vascular risk factors, pathogenesis, details of the EVT procedure, the number of thrombectomy attempts, and the time from stroke onset to groin puncture and recanalization.
Vascular risk factors encompassed histories of atrial fibrillation, hypertension, diabetes, smoking, hyperlipidemia, and stroke/TIA. Stroke severity was assessed by using the NIHSS.13,14 Symptomatic intracranial hemorrhage (sICH) was defined according to the Heidelberg Bleeding Classification.15 The pathogenesis of ischemic stroke was defined according to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification.16 Vessel recanalization was defined as good when achieving modified TICI (mTICI) 2b/3.17
All of the patients with BAO were evaluated by a trained nurse. A telephone interview was conducted to assess the functional status of each patient at 90 days (±3 days). The mRS was used for evaluation, with categories defined as functional independence (mRS 0–2), good outcome (mRS 0–3).
Statistical Analysis
Dichotomous data were summarized as absolute values and percentages. Continuous variables were presented as mean ± standard deviation (SD), or median values with the interquartile range (IQR). Univariate comparisons between the 2 groups were conducted by using the χ2 test, Fisher exact test, t tests, or Mann-Whitney U test, as appropriate. Potential confounders were adjusted based on important risk factors, considering clinical judgment and expert consensus. Such confounders included age, baseline NIHSS score, time from stroke onset to puncture, and history of stroke/TIA. Multivariate logistic regression was used to obtain the OR and 95% CI for the associations between the 2 groups and their outcomes. Statistical analysis was performed by using SPSS Version 26 (IBM), and a P value < .05 was considered to indicate statistical significance.
RESULTS
Participants
During the study period, 361 patients with AIS with BAO were treated with EVT. Among them, 155 patients with BAO who were also eligible for IVT presented within 4.5 hours of symptom onset. After excluding 2 patients who were lost to follow-up, a total of 153 patients with AIS and BAO, presenting within 4.5 hours after symptom onset, were enrolled in this study. These patients comprised 65 and 88 patients in the DEVT and bridging-therapy groups, respectively (Fig 1).

Flow chart of the current cohort study.
Baseline Characteristics
Table 1 summarizes this multicenter retrospective cohort study, comparing 65 patients (42.5%) who underwent DEVT (mean ± SD age, 68 ± 13 years) with 88 patients (57.5%) who received bridging therapy (mean ± SD age, 67 ± 12 years). In the DEVT group, median (IQR) NIHSS score was 22 (10, 35), median (IQR) time from stroke onset to groin puncture was 238 (158, 262) minutes, median (IQR) time from groin puncture to recanalization was 85 (60, 114) minutes, and median (IQR) time from stroke onset to recanalization was 311 (248, 349) minutes. In the bridging-therapy group, median (IQR) NIHSS score was 26 (15, 35), median (IQR) time from stroke onset to groin puncture was 237 (150, 310) minutes, median (IQR) time from groin puncture to recanalization was 78 (60, 100) minutes, and median (IQR) time from stroke onset to recanalization was 313 (230, 438) minutes. The NIHSS scores and the duration at each stage were similar between the 2 groups. Regarding pathogenesis, 33.3% resulted from intracranial atherosclerotic stenosis (ICAS), 46.4% were cardioembolic, and 20.3% were of other types, showing a homogeneous distribution of stroke mechanisms in both the DEVT and bridging-therapy groups (P = .507). No significant differences were found in the details of the EVT procedure and remaining baseline data between the 2 groups.
Baseline characteristics of patients between DEVT and bridging-therapy groups (n=153)
Primary and Secondary Outcomes
The primary and secondary outcomes are presented in Table 2. At 90 days, a total of 50 (32.7%) patients had died, and 64 (41.8%) had good outcomes (mRS 0–3). The proportion of patients achieving good functional outcomes at 90 days showed no significant difference between the DEVT and bridging-therapy groups (44.6% versus 39.8%, P = .548) (Fig 2). Following adjustments for potential confounding factors, the frequency of good functional outcomes remained comparable between the 2 groups (adjusted odds ratio [aOR], 1.12; 95% CI, 0.55–2.31; P = .753).

{kind=link}
{kind=link}
{kind=link}
Distribution of mRS score at 90 days.
Comparison of outcomes between DEVT and bridging-therapy groups (n=153)
After adjusting for potential confounders, secondary outcomes were found similar between the DEVT and bridging-therapy groups, except for the number of thrombectomy attempts. Analysis of the secondary outcomes revealed that fewer patients required ≥3 retrieval attempts in the bridging-therapy group than in the DEVT group (aOR, 0.39; 95% CI 0.16–0.93; P = .034). The percentage of patients with functional independence at 90 days was comparable between the bridging-therapy and DEVT groups (35.4% versus 34.1%) (aOR, 1.25; 95% CI, 0.59–2.65; P = .553). Mortality at 90 days was 32.3% in the DEVT group and 33.0% in the bridging-therapy group. There was no significant difference in mRS 0–1 or sICH between the 2 groups at 90 days. Successful reperfusion (mTICI 2b/3) of the basilar artery on final angiography was observed in 132 (86.3%) patients, with no statistical difference between the 2 groups (86.2% versus 86.4%) (aOR, 1.14; 95% CI, 0.43–3.06; P = .795).
DISCUSSION
In this multicenter retrospective study, we evaluated the outcomes of EVT with or without IVT within 4.5 hours of symptom onset in patients with BAO-induced AIS. No significant difference was observed in the proportions of patients who achieved a good functional outcome between the DEVT (44.6%) and bridging-therapy (39.8%) groups. Likewise, secondary outcomes, including the rate of recanalization, sICH, and other functional outcomes, were not significantly different between the 2 groups, except for the number of thrombectomy attempts. Hence, our findings do not indicate a benefit of bridging IVT before EVT for the primary functional outcome at 90 days. Nevertheless, the analysis of the secondary outcomes revealed that IVT bridging may reduce the number of retrieval attempts required.
There is limited research on the comparison of DEVT versus bridging therapy in the posterior circulation. Existing analyses from several studies have yielded inconsistent results regarding the efficacy of bridging therapy.5⇓⇓-8 Several authors have suggested that bridging therapy is more effective than DEVT for patients with posterior large vessel occlusion,5,8,9 whereas multiple studies have shown that the outcomes for patients with BAO-induced AIS who are treated with DEVT do not significantly differ from those treated with bridging therapy.6,7,10 In previous studies comparing bridging therapy and DEVT in the posterior circulation, not all the patients in the DEVT groups received treatment within 4.5 hours. Patients who are treated late may experience increased neuronal death due to the extended time, ultimately contributing to a poor prognosis.18,19 To mitigate the impact of major confounders, we aimed to enroll only patients who presented within 4.5 hours of symptom onset, enabling a precise comparison of the effects of the 2 therapeutic methods.
In this study, DEVT and bridging therapy did not significantly differ in yielding a good functional outcome. This conclusion aligns with previous reports by Siow et al6 and Guo et al.7 However, in the study of Siow et al,6 the subgroup analysis of patients with BAO with ICAS demonstrated an association between bridging therapy and improved functional outcomes. Additionally, the study of Nie et al,5 in which 81% of the patients with BAO had ICAS, also suggested bridging therapy to be advantageous, potentially leading to better outcomes, over DEVT. Several studies have shown that patients with ICAS tend to exhibit better collateral circulation than those with other types of stroke.20 The collateral circulation of the basilar artery may compensate for the decrease in blood flow.7 Presumably, the thrombolytic agent also flows with the blood through collateral vessels, reaching the distal end of the thrombus more effectively, enhancing the efficacy of EVT, and contributing to improved functional outcomes.21 In the present study, patients with ICAS constituted only 33.6% of the cohort. Therefore, we suspect that bridging therapy might have a limited impact on our patients, thus resulting in the absence of significant prognostic differences between the DEVT and bridging-therapy groups. Additionally, our study observed the safety of DEVT and bridging therapy for acute BAO, including the mortality and the occurrence of sICH at 90 days poststroke. Nevertheless, we observed a higher mortality rate than those reported in previous studies despite a similar rate of sICH. This discrepancy may be attributed to the relatively higher baseline NIHSS scores and ages in our cohort than in previous studies.
Although our study did not reveal divergent prognoses, variations were observed in the number of thrombectomy attempts. The DEVT group consisted of a larger proportion of patients who required 3 or more passes with stent retrievers. Our observations appear to corroborate the hypothesis that rtPA mitigates the challenges of mechanical thrombectomy by dissolving fibrin and softening and loosening the thrombus.22,23 In a study utilizing rats with cerebral artery occlusion as a model, fibrinogen concentration was dramatically decreased 1 hour after the end of the infusion treatment in the alteplase group.22 The authors indicated that rtPA might induce clot softening by preventing platelet aggregation and promoting platelet disaggregation through the induction of fibrinolysis.22 Furthermore, rtPA aids in the removal and aspiration of clots by detaching them from the endovascular surface and dissolving clots that may have escaped distally during the procedure, thus reducing the number of thrombectomy attempts.7 Given the findings of the aforementioned studies, we observed that the bridging-therapy group typically had a shorter median time from groin puncture to recanalization (78 minutes with an IQR of 60–100 minutes) than the DEVT group (85 minutes with an IQR of 60–114 minutes). This difference can be attributed to fewer thrombectomy attempts in the bridging-therapy group than in the DEVT group. However, the lack of statistical significance may be due to the limited sample size.
This study has several limitations. First, the nonrandomized design, coupled with treatment decisions made at the discretion of family members, introduces potential biases. The retrospective nature of this study limited our ability to explore factors influencing treatment choices. Specifically, we could not fully investigate the reasons for choosing direct thrombectomy, a decision that may have significantly impacted the observed outcomes. Second, thrombus size, which is likely a significant factor influencing treatment outcomes,24⇓-26 was not prospectively measured in our stroke database in a standardized manner, and retrospective measurement was not possible due to technical imaging limitations. Consequently, we could not incorporate these factors into the matching analysis. Finally, our sample size was relatively small. In the future, further analysis with a larger sample group and long-term follow-up is needed to confirm our results.
CONCLUSIONS
In the management of patients with BAO-induced AIS, DEVT demonstrates comparable functional outcomes to bridging therapy within 4.5 hours of symptom onset. Nevertheless, IVT can reduce the number of thrombectomy attempts. Further confirmation of these findings is essential through prospective randomized controlled trials.
Footnotes
Mo Yang and Yue-zhou Cao contributed equally to this article.
This work was supported by the Social Development Project of the Jiangsu Provincial Science and Technology Department (BE2022809) and the Clinical Capacity Improvement Project of the Jiangsu Provincial People’s Hospital (JSPH-MA-2022-4).
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- Received May 21, 2024.
- Accepted after revision September 29, 2024.
- © 2025 by American Journal of Neuroradiology