Graphical Abstract

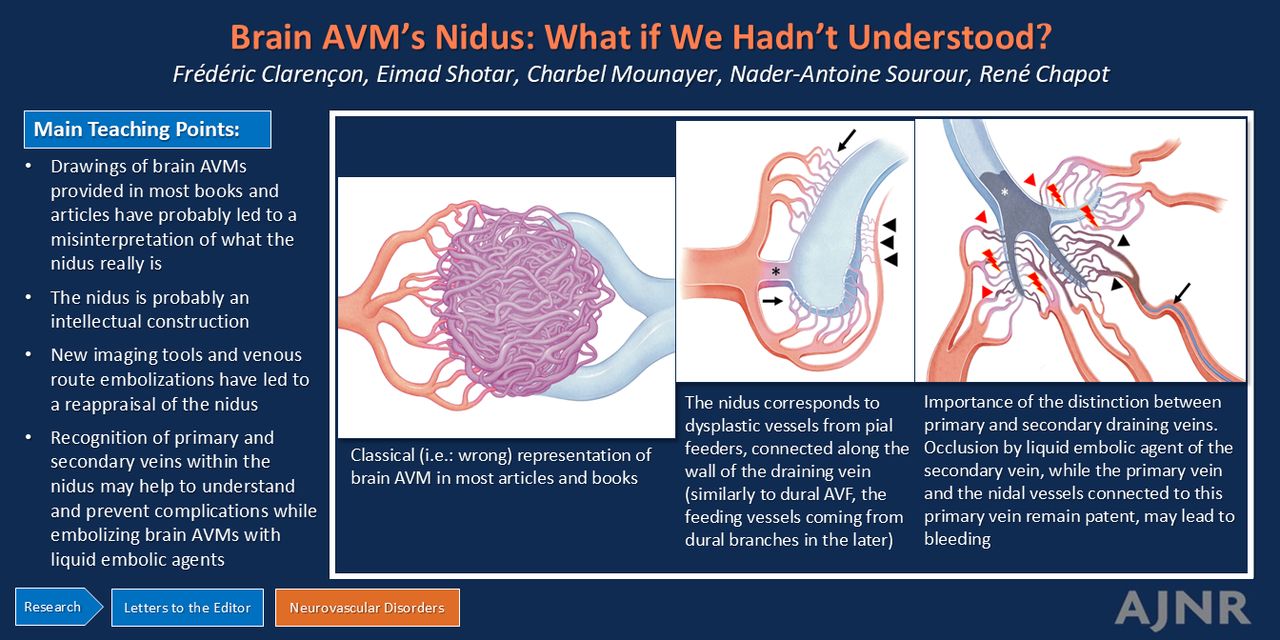
Brain arteriovenous malformations (bAVMs) are complex and aggressive vascular malformations that were, until recently, thought to be congenital. More data on the genetics and biology of these malformations support them being acquired lesions that develop on a predisposing background (the so-called “response to injury” theory) rather than congenital malformations. Additionally, there has been a major breakthrough in understanding AVM pathophysiology with the identification of somatic activation mutations in the KRAS proto-oncogene, specifically in the endothelial cells of AVMs.
The nidus is composed of dysplastic vessels with an ambiguous nature, sharing the pathologic characteristics of arteries and veins. These vessels do not supply the normal brain parenchyma.
Geibprasert et al1 define the nidus as “The transition between artery and vein can take place via a so-called nidus (i.e., a tangle of abnormal vessels located in the brain parenchyma) or can be direct (i.e., fistulous) without any intervening network.” In Forsting and Wanke,2 Intracranial Vascular Malformations and Aneurysms, Cognard and Pierot,3 in the chapter focused on brain AVMs (chapter 3), describe the nidus, “Anatomically speaking, they are constituted by a complex, tangled web of afferent arteries and draining veins linked by an abnormal intervening capillary bed–the so-called nidus–which may or not harbor direct arteriovenous shunts.” Most interesting, Newton and Potts,4 Radiology of the Skull and Brain: Angiography, in chapter 83 by Newton and Troost, focused on brain AVMs; the meaning of the term “nidus” is nowhere detailed.
The nidus (from the Latin language nidus = nest) is the center of gravity of the bAVM. Indeed, the shunt points of the bAVM are located in the nidal component of the bAVM. The nidus is, thus, the target of the exclusion treatment, whatever treatment technique is chosen.
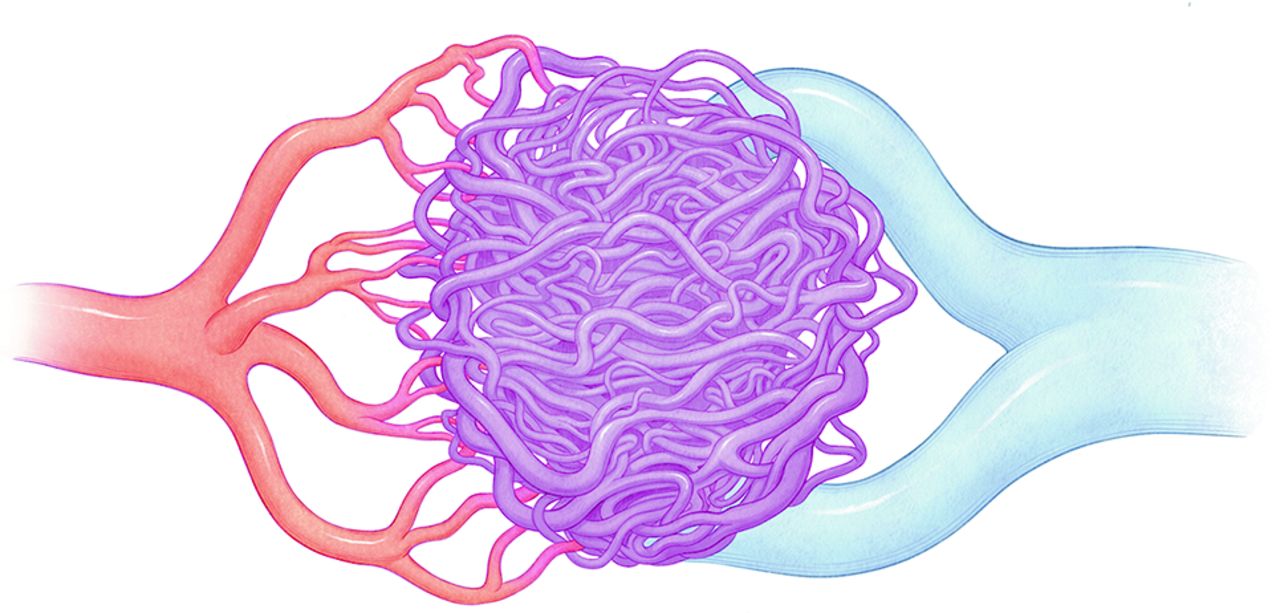
The nidus is often represented in books and articles as a tangled web of dysplastic vessels, which can be more or less compact. In most drawings available in the literature and books, the nidus is displayed as a coherent vascular net fed by arterial feeders from one side, which exit one or several draining veins from the other side (Fig 1).

Classic representation of the nidus in most articles and books focused on brain AVMs.
According to our experience in analyzing the angioarchitecture of bAVMs with new imaging tools like segmentation or anamorphosis algorithms, and to the recent advances of the transvenous approach for bAVM embolization that offered a reappraisal of the relationship between the nidus and the draining veins, the usual representation of the nidus in the literature appears to be more an intellectual construct than a faithful representation of the real details.
A very different understanding of the nidus has appeared since AVMs have been treated by transvenous embolization. The retrograde filling of the main vein of the AVM and later the primary veins has been playing a key role in redefining the angioarchitecture of the nidus.
The epicenter of the bAVM is the draining veins. The nidus may present as a “ball of yarn” and is called “plexiform” in such a configuration. Conversely, it may present a purely fistulous aspect. Some nidi may have a mixed pattern (Fig 2A). When the nidus is plexiform, it may present a spectrum of configurations depending on the compactness of the nidus, ranging from a very compact nidus to a widespread nidus. The nidus may drain directly into a main draining vein (Fig 2A), or it may drain in primary draining veins, draining themselves in a secondary draining vein (Fig 2B). The ball of yarn aspect of the nidus is because the main draining vein is usually rolled up on itself.

{kind=link}
{kind=link}
{kind=link}
A, Drawing summarizing the different connection patterns of the arterial feeders with the draining vein through the nidus: via terminal branches (arrows), via “en passage” branches (arrowheads), or directly through the arteriovenous fistula (*) B, Drawing showing the connection of the vessels belonging to the nidus to the primary veins (*), which are draining themselves in a main secondary vein (**). C, An example of a liquid embolic agent (LEA) injection pattern at risk of secondary bleeding. The LEA is injected through a dimethyl-sulfoxide-compatible microcatheter (black arrow) feeding the target compartment of the nidus (black arrowheads). The LEA has filled the primary vein draining the target compartment, but the embolic agent has also refluxed in nidal vessels belonging to another adjacent compartment (red arrowhead). Because all the nidal vessels of this adjacent compartment are not occluded and the primary draining vein is compromised, the remaining nidal vessels of this second compartment are at high risk of bleeding (red lightning). D, Second, an example of an LEA injection pattern at risk of secondary bleeding. The LEA is injected through a dimethyl-sulfoxide-compatible microcatheter (black arrow) feeding the target compartment of the nidus (black arrowheads). All the nidal vessels of the target compartment are occluded, as well as the primary draining vein and all the nidal vessels of the adjacent nidal compartment. Inopportune progression of the LEA has occluded the secondary draining vein (*), as well as some nidal vessels from other compartments (red arrowheads). Because their venous outflow is compromised, these other compartments are at high risk of bleeding (red lightnings).
This more precise understanding of the organization of the nidus helps to better appreciate and anticipate the behavior of liquid embolic agents, especially ethylene-vinyl alcohol (EVOH) copolymer when injected via the arterial side and the pathomechanism of delayed hemorrhagic complications. Indeed, according to our experience, the different compartments of the nidus do not communicate with one another, except marginally via pial anastomoses. The main means (and almost the only one, without considering the pial anastomoses) to occlude some portions of the nidus distant from the EVOH injection site while performing arterial side embolization is to penetrate via the draining vein and to retrogradely fill other portions of the nidus (in the same fashion as in embolization of intracranial dural arteriovenous fistulas treated with nonadhesive liquid embolic agents). No complication will be observed if all the nidal vessels communicating with the draining vein are occluded, even if this primary draining vein is occluded by the liquid embolic agent. If the secondary draining vein is occluded or slowed down, no bleeding will occur only if all vessels belonging to the nidus are occluded. Conversely, bleeding events may be observed in 2 scenarios: when the primary vein is occluded (or dramatically slowed down) and all the nidal vessels communicating with this vein are not occluded (Fig 2C) and when the secondary vein is occluded (or dramatically slowed down), while all the nidal vessels (ie, nidal vessels of all the compartments) are not occluded (Fig 2D).
In conclusion, the representation of the nidus of brain AVMs for many years in drawings may have negatively influenced our understanding of the angioarchitecture of bAVMs. Additionally, it may have led to a misunderstanding of the causes of embolization-related hemorrhagic complications, while contaminating the draining veins with liquid embolic agents.
Acknowledgments
The authors kindly thank Diane Rottner for providing the drawings illustrating this letter.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- 1.
- 2.
- 3.
- 4.
- © 2025 by American Journal of Neuroradiology